


ŌģĀ. Introduction
Chronic infantile neurological cutaneous articular (CINCA) syndrome, also known as Neonatal Onset Multisystem Inflammatory Disease (NOMID), is one of the groups of cryopyrinassociated periodic syndromes (CAPS), or periodic fever syndromes. CINCA is the most severe type of CAPS and causes fever with inflammation in multiple organs. These diseases are related to mutations of the NLRP3 gene, which is located on chromosome 1[1,2]. NLRP3 is known to encode protein cryopyrin, which can increase the levels of pro-inflammatory, pyrogenic interleukin-1-beta (IL-1╬▓)[2]. IL-1╬▓ plays an important role in inflammatory response and various cellular activities. Due to elevated levels of IL-1╬▓, patients with CINCA syndrome have maculopapular skin rash, musculoskeletal problem, periodic fever and flare-up, eye inflammation, and central nerve system impairment[3]. Before the association between CINCA and upregulated IL-1╬▓ was identified, 20% of the children with CINCA died in their early childhood[4].
In the oral environment, IL-1╬▓ is known to act as a potential etiological agent for periodontitis[5]. IL-1╬▓ is also associated with Streptococcus mutans (S. mutans ), which is involved in dental caries[6,7]. Patients with CINCA syndrome are vulnerable to dental diseases.
In particular, the uncooperative behavior of most children with CINCA makes it difficult for the clinician to perform dental treatment effectively. In such cases, general anesthesia would be useful. Pro-inflammatory characteristics in patients with CINCA syndrome should be considered before conducting dental treatment under general anesthesia. In this article, we report a case of an uncooperative child with CINCA syndrome, who was treated under general anesthesia, and discuss the points that should be taken into consideration before dental treatment.
ŌģĪ. Case report
A 3-year-old girl with CINCA syndrome was referred to Seoul National University Dental Hospital for multiple caries. She had symptoms of skin rash, elevated levels of inflammatory factors (complete blood count [CBC], 18460-8.1/26.9-763K; erythrocyte sedimentation rate [ESR], 66; C-reactive protein [CRP] 71.4 mg/dL), and motor disorder of legs immediately after birth. She was diagnosed with CINCA syndrome based on genetic analysis and had been treated with injectable IL-1╬▓ antagonist, anakinra (13 mg). After anakinra injection, her symptoms had subsided and the blood test results were within normal range.
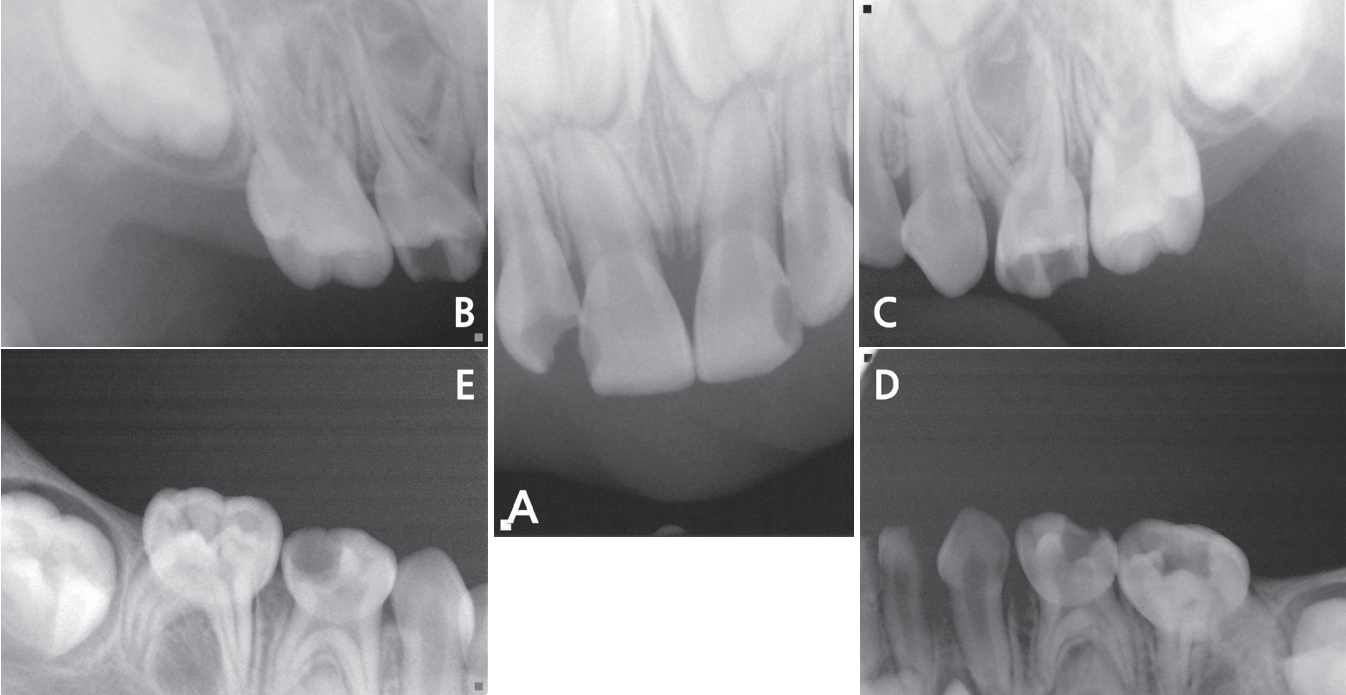
Clinical and radiographic examinations revealed multiple caries (Fig. 1, 2A - 2C). Dental caries were found in the left and right upper anterior primary central and lateral incisors, 1st primary molars, and lower left and right 1st and 2nd primary molars. In addition, an impacted inverted mesiodens was found between #51, 61, in the periapical region.
Considering the patientŌĆÖs age and compliance with the dental treatment procedure, dental treatment under general anesthesia was planned. Before treatment, her physician was consulted to ensure that she did not require any premedication. General anesthesia was induced with sevoflurane and maintained with desflurane, nitrous oxide, and oxygen. Maxillary anterior teeth except the upper right primary lateral incisor were treated with composite resin restoration. Pulpectomy and resin restoration were performed in the upper right lateral incisor. The lower right and left 2nd primary molar were restored with composite resin. Pulpotomy and stainless steel crown restoration were performed in the rest of the upper and lower molars (Fig. 2D - F). Finally, fluoride varnish was applied to prevent progression and occurrence of caries. Extraction of impacted mesiodens was postponed due to the risk of damage to the permanent tooth germ during surgical intervention. Successful dental procedure was carried out under general anesthesia. Periodic follow-up was planned (once every 3 months), to maintain oral health.
Ōģó. Discussion
CINCA syndrome, the most severe type of CAPS disorder, is a very rare chronic auto-inflammatory disorder. NLRP3 gene mutation, which leads to excessive IL-1╬▓ production, is the cause of this syndrome[8]. Currently, the best treatment for patients with CINCA syndrome is administration of one of various IL-1╬▓ inhibitors, such as anakinra, rilonacept, and canakinumab[9-13]. Anakinra is one of the IL-1 antagonists that inhibits the activity of IL-1╬▒ and IL-1╬▓ and are commonly used for the treatment of rheumatoid arthritis. Successful management of CINCA syndrome with continued anakinra medication has been reported[9,12-14]. Often, dramatic improvements appear within days to weeks of starting administration of these medications[9,14].
In this case, genetic analyses revealed a mutation in the NLRP3 gene and hence the patient was diagnosed with CINCA syndrome. The patient had typical symptoms of CINCA syndrome such as skin rash, elevated ESR, elevated CRP levels, and joint disorder. After administration of anakinra, the symptoms improved.
Since IL-1╬▓ is a mediator of inflammatory reaction, elevated IL-1╬▓ levels are closely associated with rheumatoid arthritis, type 2 diabetes, and osteoarthritis[15-17]. These patients also have associated dental problems. In the oral environment, upregulated IL-1╬▓ level is associated with dental caries. Some reports suggested that increase in the concentration of IL-1╬▓ in the saliva is related to the proliferation of S. mutans which is a major microbial species for dental caries formation, especially smooth surface caries and multiple caries[6,7]. Wang et al .[18] also reported that IL-1╬▓ gene is positively correlated with dental caries. Therefore, elevated levels of IL-1╬▓ can be thought to be one of the contributing factors of dental caries.
IL-1╬▓ also affects the periodontal tissue. Many reports revealed that IL-1╬▓ is correlated with periodontal bone destruction and periodontal tissue inflammation, and aggravates periodontitis. For this reason, IL-1╬▓ is currently used for an index for periodontitis[19,20]. Elevated IL-1╬▓ levels increase the susceptibility to periodontitis, resulting from Aggregatibacter actinomycetemcomitans, which is one of the causes of destructive periodontitis[21]. Thus in patients with CINCA syndrome, the periodontal condition should be assessed regularly.
As mentioned earlier, patients with CINCA syndrome are prone to oral diseases, especially when IL-1╬▓ is unregulated. Moreover, children whose oral health care cannot be maintained have an increased risk of developing dental caries. Developmental delay associated with this syndrome may require behavioral guidance techniques for dental treatment. When children are uncooperative and cannot accept dental treatment, general anesthesia could be a helpful behavior management technique.
Lauro et al .[22] reported that without active infection, even in the presence of fever and chronic aseptic meningitis, general and regional anesthesia may be adminstered in patients with CINCA without complications. In this case, considering the patientŌĆÖs age and treatment non-compliance, general anesthesia was planned. General anesthesia was induced with inhalation anesthetics. Although intravenous anesthetics are reported to have an immune modulatory effect, inhalational anesthetics can be safely used in these patients. However, in patients with CINCA syndrome, general anesthesia may have to be postponed as they have higher chances of developing unexpected fever[22]. Furthermore, inflammation of the laryngeal muscles during laryngoscopy may hinder airway management during and after general anesthesia[22]. Therefore, when dental treatments are performed under general anesthesia, dentists should collaborate with anesthesiologists during the perioperative period. Considering joint anomalies that can lead to impairment of function and deformities, careful positioning of these patients is necessary during dental treatment under general anesthesia. As postoperative pain is less likely to induce alterations in the immune system, postoperative analgesic should be considered[23]. However, there are no reports about the stress adversely effects of general anesthesia on the patientŌĆÖs condition.
Although dental treatment was successfully performed under general anesthesia in this case, prevention of oral disease is important. Early detection is essential to prevent and avoid the progression of oral diseases, as more surgical trauma causes more changes in the immune system[23]. Therefore, dentist and dental hygienist must cooperate with other health care providers and family members to provide professional dental and home care. Moreover, observation of eruption of permanent teeth will be necessary as Syed et al .[24] have reported an overall delayed eruption of permanent dentition in a 16-year-old girl with CINCA syndrome. However, oral manifestations in patients with CINCA syndrome has not been well investigated[25].
ŌģŻ. Summary
In this case, dental treatment under general anesthesia was successfully performed in a patient with CINCA syndrome. Before dental treatment, the medical conditions should be thoroughly examined in a patient with CINCA syndrome. Since elevated IL-1╬▓ level is associated with dental caries and periodontal conditions, professional oral prophylaxis and topical fluoride application should be considered through periodic visits.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






