


ŌģĀ. Introduction
Pit and fissure is considered the area most susceptible to dental caries. Early diagnosis and treatment of pit and fissure caries are essential since it is not easily visible and can rapidly progress downward. Traditional treatment for occlusal caries is very invasive, requiring cutting of not only the carious structure, but also the intact pits and fissures. Recently, there has been a shift toward minimally invasive dentistry to preserve the tooth structure with the development of adhesive systems and flowable resins with improved properties[1,2].
As the concept of minimally invasive dentistry is becoming more common, the treatment of occlusal caries has shifted into a combination of treatment and prevention by sealing the fissures regardless of the presence of caries. To prevent or treat occlusal fissure caries, the penetration and microleakage of sealants have the greatest impact on treatment success. It is also known that these factors are most strongly affected by the anatomical shape of the fissure. Nagano[3] categorized the shape of occlusal fissures into four types, and suggested that types K and I are more difficult for sealants to penetrate than types U and V. Therefore, the mechanical modification of fissure shape, so called fissurotomy or enameloplasty was suggested to widen the fissure opening and improve the penetration depth of the sealants[4].
Although there is some controversies about the effectiveness of fissurotomy on retention rate of sealants, it is clear that fissuorotomy has a positive effect on the penetration of sealant[5-8].
There are no definitive criteria for the treatment of early occlusal caries regarding whether to suppress the progress of a carious lesion through preventive measures or prepare a cavity and fill it with restorative material. Several studies have reported that the sealing of fissure caries inhibits the progression of the carious process[9-11]. However, other studies have reported that the sealing of carious fissures can create secondary caries through microleakage due to a lack of adhesion[12,13]. In order to solve such a problem, some attempts have been made to apply restorative material such as flowable resin using adhesive system to the carious fissure[14].
Recently, the physical properties such as viscosity, modulus of elasticity of flowable resins have improved, allowing them to be used as sealants. When flowable resin is used as a sealant, retention is expected to increase because of good abrasion resistance. However, penetration may be detrimental since the fluidity is relatively weak compare to conventional sealants. So, major concern is focused on the additional techniques such as fissurotomy to compensate the weakness of flowable resin as sealant in both sound and carious fissure.
The aim of this study is to evaluate the effect of fissurotomy on the penetration and microleakage of flowable resins for carious fissures.
ŌģĪ. Materials and methods
1. Materials
A total of 250 premolars with early pit and fissure caries that were extracted for orthodontic purposes were used in this study. Samples were examined by visual inspection, probing, and DIAGNOdent┬« (Kavo, Biberach, Germany) for the diagnosis of initial caries. The DIAGNOdent┬« value was measured for each sample on carious fissures in accordance with the manufacturerŌĆÖs instructions. The diagnostic criteria for initial caries proposed by the manufacturer of DIAGNOdent┬« ranged between 14 and 20.
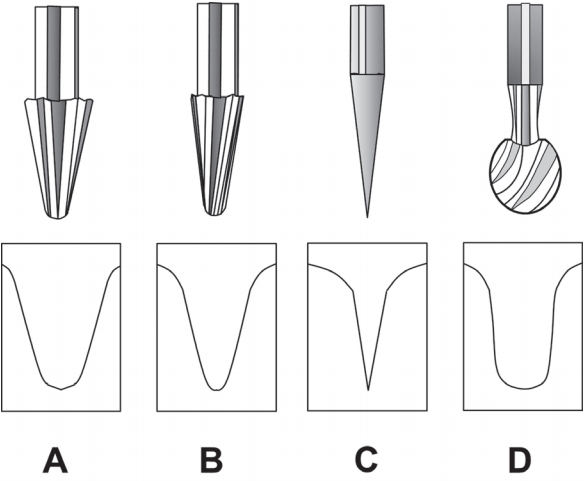
Fissurotomy® Original Bur (SS WHITE, USA), Fissurotomy® Miro NTF bur (SS WHITE, USA), SF104R tapered diamond bur (Shofu, Japan), and 1/2 round carbide bur (SS WHITE, USA) were used for the fissurotomy. Two flowable resins (Unifil® Flow, GC, Japan and Filtek®Flow, 3M-ESPE, USA), etchant (Ultra-Etch®, Dentsply, USA), and dentin adhesive (Single Bond®, 3MESPE, USA) were used in this study.
2. Sealing of carious fissures with flowable resin
Teeth were randomly assigned to 10 groups of 25 teeth based on the types of flowable resin and fissure preparation method (Table 1). Fissurotomy was performed with the Fissurotomy ® Original bur, Fissurotomy® Miro NTF bur, SF104R tapered diamond bur, and 1/2 round carbide bur (Fig. 1), followed by acid etching for 20 s with 35% phosphoric acid, rinsing, and drying. A dentin adhesive was applied to the etched surface and cured for 10 s with BeLite® LED (B&L Biotec, South Korea), followed by placement of flowable resins and curing for 20 s.
3. Assessment of penetration depth and microleakage
Samples were stored in distilled water at room temperature for 24 h and then samples were subject to thermocycling for 500 cycles between 5┬░C and 55┬░C water baths for 30 seconds each. All tooth surfaces, excluding 1 mm outside the sealant margin, were coated twice with nail varnish to prevent unnecessary dye penetration into spaces other than the sealant areas, and were then stored in 2% methylene blue dye solution for 24 h. Following immersion, teeth were washed under running water to remove the remaining dye and were then embedded in epoxy resin.
Samples were sectioned in the buccolingual direction with an Isomet low-speed diamond wheel saw (Model 650, South Bay Technology, USA) to expose the vertical section of the fissure, and were then polished with 1000, 1200, 2400, and 4000 grit silicon carbide paper under water cooling. The penetration depth and microleakage of the exposed section were observed using a stereomicroscope (Olympus SZ61┬«, Japan) at 40 ├Ś magnification.
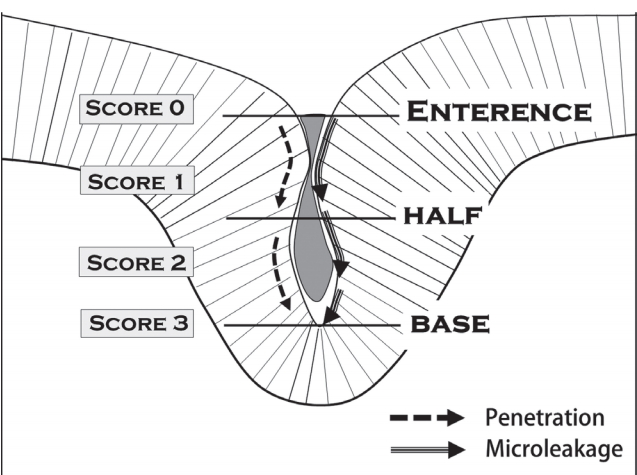
The penetration depth and microleakage were evaluated according to the criteria proposed by Hevinga et al .[15] (Fig. 2).
ŌĆó 0 : No penetration;
ŌĆó 1 : Penetration down to half of the fissure;
ŌĆó 2 : Penetration extending beyond half of the fissure;
ŌĆó 3 : Penetration into the base of the fissure.
4. Evaluation of adaptation
Samples were dried using a vacuum desiccator and plated using an ion sputter with a voltage of 2 kV, current of 20 mA, and a vacuum status of 4 ├Ś 10-2 bar/pa, after which the flowable resin and fissure enamel interface was examined by scanning electron microscopy (JOELJSM-840A, JOEL Co., Japan).
5. Statistical analysis
SPSS (ver. 23.0) was used for data analysis. Statistical significance was set at 95% (p= 0.05). FisherŌĆÖs exact test was used to verify the significance of penetration depth and microleakage among groups, as well as between each group, and the Mann-Whitney test was performed to verify the significance between the types of flowable resin.
Ōģó. Results
1. Assessment of penetration depth and microleakage
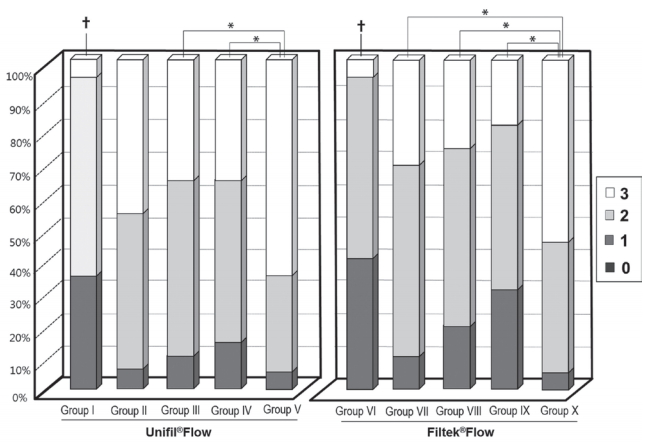
For the penetration score, control group samples (group I and VI) were mostly distributed at scores of 1 and 2. However, experimental groups were distributed at scores of 2 and 3. The difference in sample distribution between the control and experimental groups showed statistical significance (p < 0.05) (Fig. 3).
For Unifil®Flow flowable resin, group V showed deeper penetration than group III and IV (p < 0.05). However, there was no significant difference in penetration depth between groups V and II. For Filtek®Flow flowable resin, group X showed the highest penetration depth among the experimental groups (p < 0.05) (Fig. 3).
For the penetration depth according to the type of flowable resin, the mean score of the Unifil®Flow flowable resin was 2.67 ± 0.67, which was greater than that of the Filtek®Flow flowable resin with 2.04 ± 0.32 (p < 0.05) (Table 2).
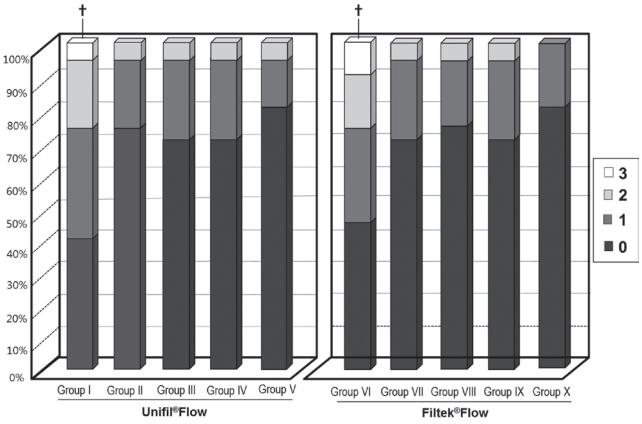
For the microleakage, control group samples were evenly distributed at all scores (0 - 3); however, experimental group samples were distributed at a score of 0 and not a score of 3. Experimental groups showed lower microleakage scores than the control group (p < 0.05) and there were no significant differences in microleakage scores among experimental groups (Fig. 4). For the microleakage according to flowable resin types, there were no significant differences between groups (Table 3).
2. Assessment of the adaptation
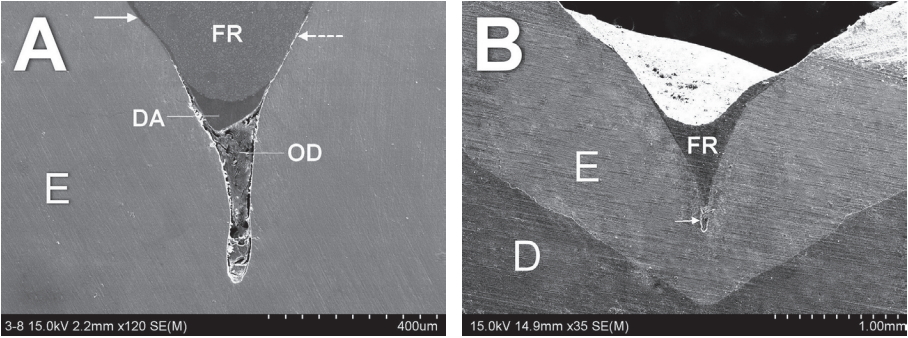
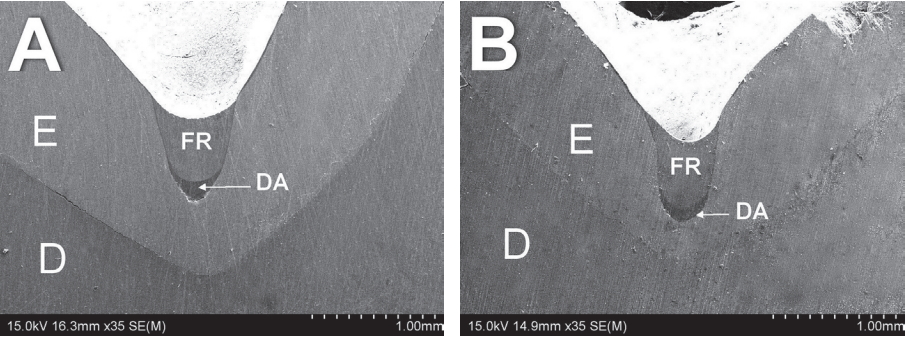
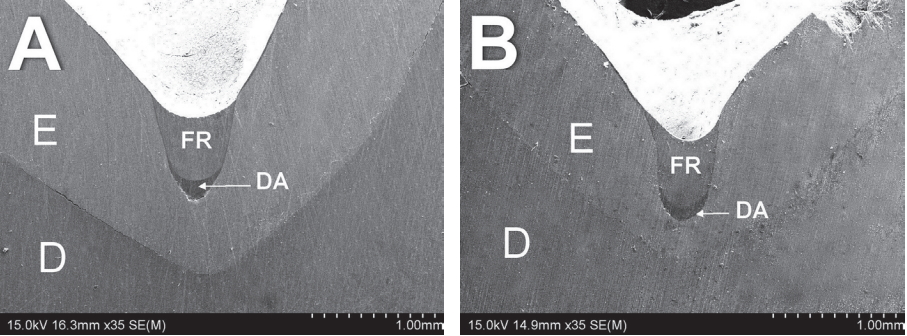
Many samples in the control group showed incomplete penetration of flowable resin into the fissure, particularly samples with long and narrow fissures. Experimental groups generally showed better penetration and closer contact with the fissure wall than the control group; however, there were some differences according to the shape of the fissure prepared by the various burs (Fig. 5 - Fig. 7).
ŌģŻ. Discussion
As the flowable resin has become more popular, itŌĆÖs range of use is expanded from restorative material for cavity to sealing material for occlusal fissure. Recently, flowable resin tends to be used for sealing the occlusal carious fissure in conjunction with non-invasive preparation.
This study was performed to evaluated the effect of fissurotomy on the penetration and microleakage of flowable resins for carious fissures. In the present study, the penetration score was higher in groups with fissurotomy than in groups without it for both Unifil®Flow and Filtek®Flow flowable resins. This suggests that mechanical preparation of the fissure is more favorable for increasing the penetration of flowable resin by achieving widening and smoothening of the fissure wall, as well as removing organic materials from the fissure[16,17].
In the present study, fissurotomy with a 1/2 round carbide bur showed higher penetration depth compared with other burs in both Unifil┬«Flow and Filtek┬«Flow flowable resin. This result indicated that a U-shape fissure formed by a 1/2 round carbide bur is more favorable for flowable resin to flow into the fissure than the V-shape fissure formed by other fissurotomy burs or a tapered diamond bur. However, there were no differences between the preparation burs regarding microleakage. This suggests that penetration does not necessarily affect microleakage. Unlike some studies on conventional sealant in healthy fissures, it is possible that the shape of the bur affects the penetration of flowable resin in carious fissures[18]. When comparison was done between Unifil┬«Flow and Filtek┬«Flow, the former showed higher penetration score. According to the technical product files provided by the manufacturers, viscosities at 40 gf for 90 seconds are 33.5 mm for Unifil┬«Flow and 26.4 mm for Filtek┬«Flow. This indicated that the flow of Unifil┬«Flow is better than that of Filtek┬«Flow when used as a fissure sealant, and this difference in flowability is reflected in our results. Several reports[19,20] demonstrated significant correlation between retention of sealant and itŌĆÖs viscosity.
When comparing microleakage, the fissurotomy groups showed less microleakage than the control group. This decrease in microleakage in the fissurotomy groups can be explained by removing the porous component of early carious lesions and debris that increased the micromechanical bonding of the flowable resin to fissure enamel. Another reason for better microleakage of flowable resin placed on the enlarged fissures by fissurotomy could be explained that removal of prismless enamel from the outmost layer of the fissure enamel enhanced the etching effect[21,22].
It was observed in SEM findings that a few samples of control group showed loose adaptation of the flowable resin to fissure wall. This is considered to be a lack of micromechanical bonding due to the increased porosity of carious enamel and organic materials in the fissure wall[23]. We observed that dentin adhesive responsible for filling the gap between flowable resin and fissure wall or fissure base. Further study is needed as to whether the dentin adhesive can play a role in enhancing adhesion in carious fissures.
In this study, fissurotomy clearly affect the penetration and microleakage of flowable rein, but in clinical practice, technical sensitivity of fissurotomy may not show the consistent result depending the dentists. If the fissurotomy is performed too shallow then the materials cannot penetrate as intended. In contrast, if the fissurotomy is performed too deep or wide, healthy structures may be removed and the quantity of materials would increase, resulting in increasing polymerized shrinkage and microleakage.
The limitation of this study is considered to be difficulty for standardization of samples because of the variety in fissure shape of natural teeth.
V. Conclusions
Based on this in vitro comparative study, fissurotomy can increase the penetration depth of flowable resin and decrease the microleakage in carious fissures. Fissure preparation with a 1/2 round bur showed the deepest penetration of flowable resin into the carious fissure, but fissure preparation methods did not show any difference in microleakage. There was a significant difference in penetration depth between the two flowable resins (Unifil®Flow and Filtek®Flow), but there was no significant difference in microleakage.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






