


I. Introduction
Turner syndrome (TS) is a chromosomal disorder caused by monosomy of the X chromosome, with complete or partial absence of the second sex chromosome[1]. The estimated prevalence of TS is approximately 1 in 2,500 live female births[2]. The syndrome has some typical characteristics: short stature, hormonal disorders such as estrogen deficiency; and cardiac or renal malformations[3]. TS has been associated with aortic coarctation and dissection, and thoracic vascular anomalies occur in 50% of cases[4].
The most common oral findings in patients with TS are small teeth, short roots, mandibular sagittal deficiency, and a high palatal arch[5]. Abnormal mandibular premolar root numbers have also been observed[6,7].
This study reports on the dental treatment of mandibular premolars in patient with TS, with dens evaginatus and taurodontism, which is known to be associated with abnormalities in the sex chromosomes[8]. It was performed with the aid of a dental microscope due to the complex root canal anatomy and anomalies of root morphology that is often seen in patients with TS.
II. Case report
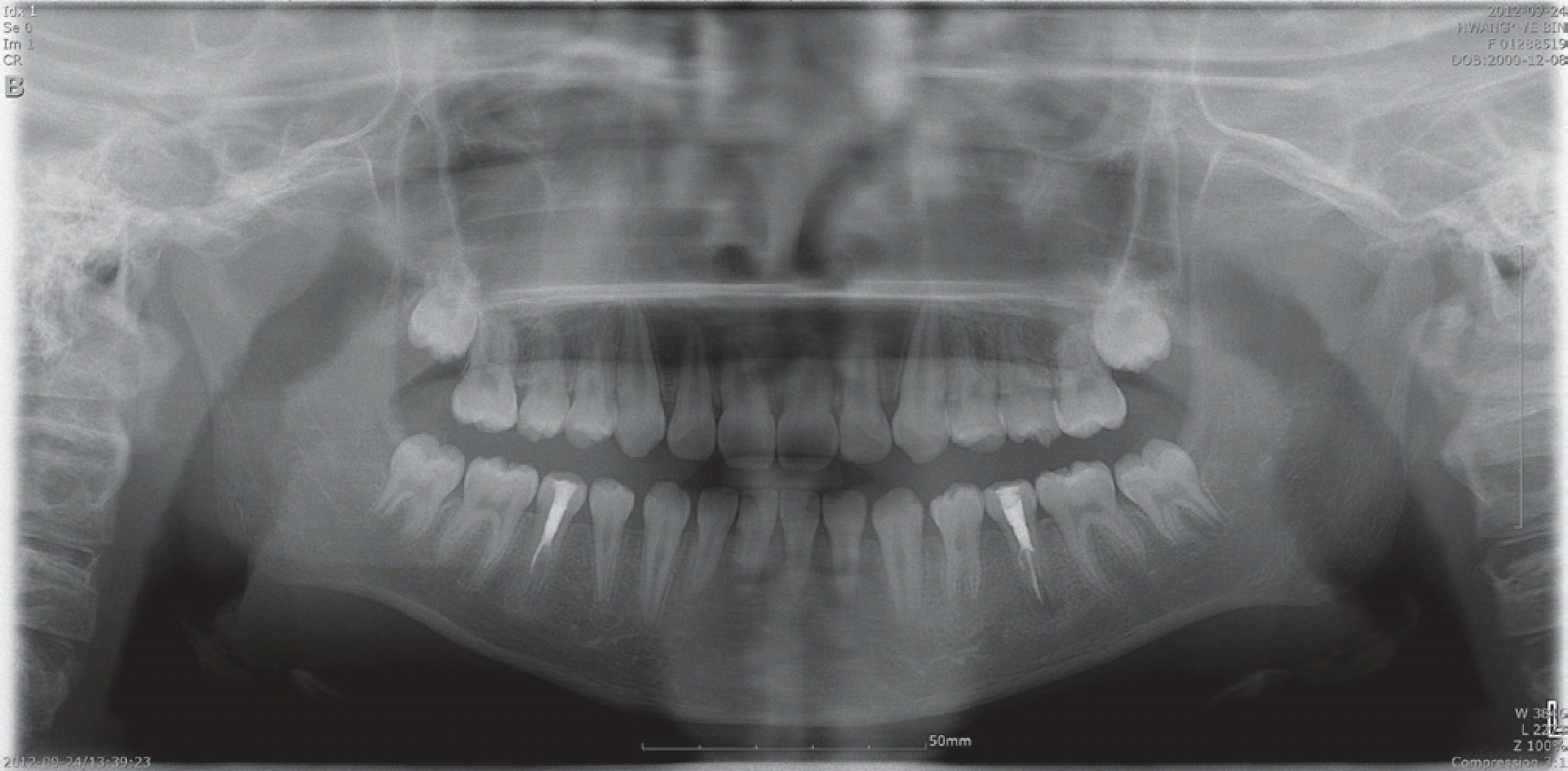
An 12-year-old girl was referred from a local dental clinic to the Department of Pediatric Dentistry, complaining of discomfort in the bilateral mandibular premolar regions. Endodontic treatment of both mandibular second premolars had been initiated 2 days previously in a local dental clinic, and the root canals were temporarily filled with a root canal filling material (Fig. 1).
The patient had been diagnosed with TS at the age of 10 years. At the first visit, the patient's height and weight were 122.5 cm and 28.4 kg, respectively, and they were below the third percentile according to the Korean Children and Adolescents Growth Standards.
The patient exhibited abnormally low posterior hairline which is characteristically found in patients with TS (Fig. 2).
Fig. 2.
Extraoral lateral photograph. The patient exhibited low and webbed neck and abnormally low posterior hairline which is characteristically found in patients with TS.

The patient underwent balloon dilatation at the age of 1.5 years due to coarctation of the aorta, a congenital heart disease. At the age of 10.5 years, the patient received growth hormone therapy to improve the short stature associated with TS, and underwent strabismus surgery under general anesthesia.
Oral examination showed the hypomineralized type of generalized enamel hypoplasia, with opaque lesions and brown discoloration, in the entire erupted dentition (Fig. 3). Dens evaginatus was detected in all premolars, but not in the bilateral mandibular second premolars where endodontic treatment had been undergoing. The previous crown shape of the bilateral mandibular second premolars, which were pain sites, could not be confirmed as the treatment had been initiated already. However, given that acute pain occurred suddenly on both sides without caries, the pain was presumed to be due to the fracture of the tubercle of dens evaginatus.
Fig. 3.
Initial intraoral photographs. Hypomineralized type of generalized enamel hypoplasia were observed with opaque lesions and brown discoloration, in the entire erupted dentition.

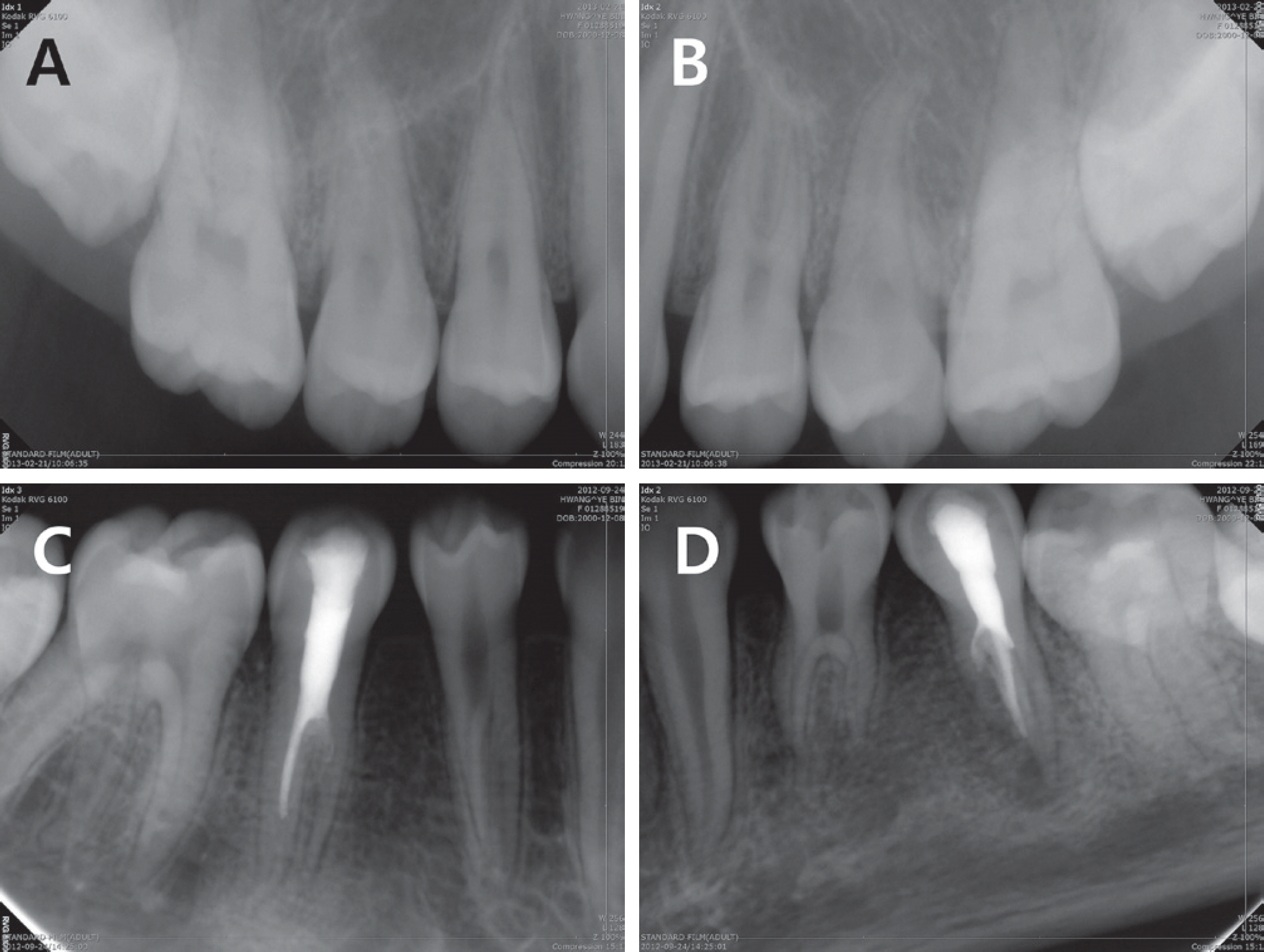
Radiographic examination showed that the maxillary right first and second premolars, the maxillary left second premolar, and the mandibular left and right second premolars had two roots; the maxillary left first premolar and the bilateral man-dibular first premolars had three roots (Fig. 4). All the mandibular premolars showed elongated pulp chambers and apical displacement of pulpal floor, suggesting taurodontism.
Fig. 4.
Initial periapical views. The maxillary premolars exhibited dens evaginatus. Taurodontic root morphology and complicated root canals were observed in all mandibular premolars. (A) Maxillary right premolars, (B) Maxillary left premolars, (D) Mandibular right premolars, (E) Mandibular right premolars.
Clinical and radiological examinations revealed periapical abscesses with sinuses in the bilateral mandibular second premolars, and we decided to perform root canal treatment. Due to the cardiac history of the patient, we consulted the pediatrician about precautions before endodontic treatment.
Selective grinding and pit and fissure sealing were scheduled for the other premolars with dens evaginatus, and after 4 days a flowable, light-cured composite resin was layered incre-mentally on the tubercles and surrounding surfaces.
About 2 weeks after the patient's first visit, the patient took 1500 mg of amoxicillin for prophylaxis 1 hour before root canal treatment as the pediatrician had recommended the use of prophylactic antibiotics before each treatment. Root canal washing and Vitapex® (Neo Dental Chemical Products Co. Tokyo, Japan) removal were performed on the mandibular bilateral second premolars. Due to taurodontism, the root canal orifices were difficult to identify and the root canal was C-shaped. We thus decided to operate under a dental microscope (Global Surgical, St. Louis, MO) to ensure adequate visualization. The mandibular bilateral second premolars were confirmed to had two roots and three root canals, which were mesiobuccal, mesiodistal and lingual, respectively. After Vitapex removal, the root canals were measured and instrumented with ProTaper (Dentsply Maillefer, Ballaigues, Switzerland) NiTi instruments. But the treatment had to be delayed for 2 months since the patient were scheduled to undergo strabismus surgery again. During that period, root canals were filled with calcium hydroxide paste.
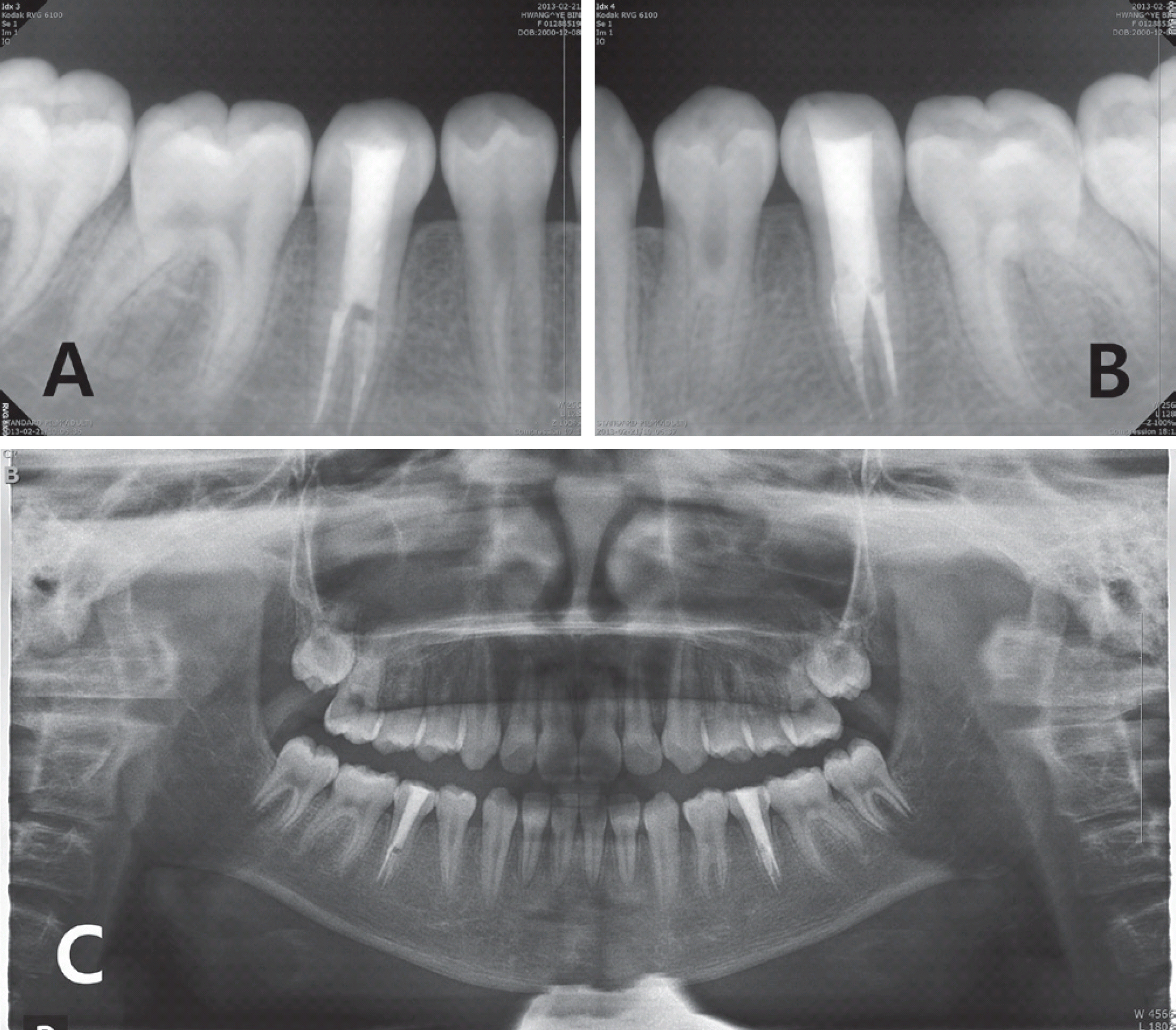
At the patient's next visit, the root canals were instrumented with a ProTaper NiTi file, with canal formation and dilatation. The symptoms were confirmed to have disappeared and the canals were filled with gutta percha (GP) cones. After root canal filling, the upper core was formed with composite resin (Fig. 5, 6).
Fig. 5.
Endodontic treatment procedures of mandibular right second premolar. (A) Initial periapical view, (B) Working length determination, (C) Master cone adaption, (D) Filling of three canals.

Fig. 6.
Endodontic treatment procedures of mandibular left second premolar. (A) Initial periapical view, (B) Working length determination, (C) Master cone adaption, (D) Filling of three canals.

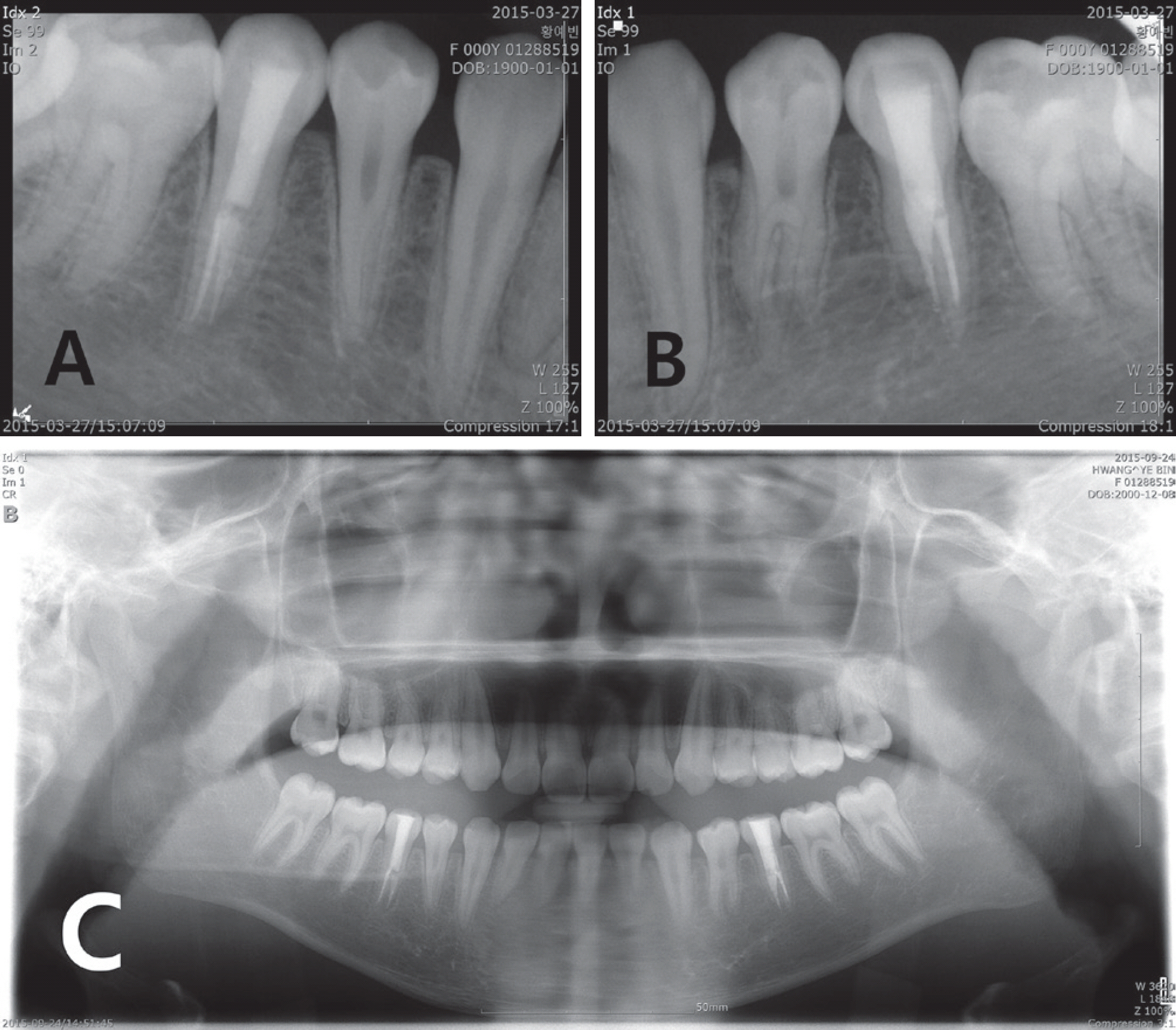
One month after root canal filling, clinical and radiological examinations were performed to confirm the prognosis of the treatment site. Periodic screening was performed every 3 months thereafter (Fig. 7). At the 2-year follow-up examination, no clinical sign or symptom associated with the teeth, and no periapical lesion, was found on panoramic radiographs (Fig. 8).
III. Discussion
TS is a chromosomal disorder characterized by complete or partial absence of an X chromosome in females. On karyotype examination, approximately 50% of patients show complete loss of the X chromosome and the remaining patients show a multitude of chromosomal abnormalities, including partial loss of the X chromosome and mosaicism[9].
Most patients with TS have characteristic clinical features, such as short stature, delayed pubertal growth spurt, primary amenorrhea, and gonadal dysgenesis[10]. They may also have visual or hearing abnormalities, and/or an elevated risk of thyroiditis and other autoimmune diseases[11]. Approximately 30% of patients with TS have congenital heart defects[12-15]. Therefore, when establishing dental treatment plans for patients with TS, dentists should consider the need for prophylactic antibiotics to prevent infective endocarditis and, in some cases, cardiological consultation. The development of intel-ligence is normal in most patients with TS, and these patients have no unusual difficulty with behavioral control.
In the case reported here, the patient visited the Department of Pediatrics with the chief complaint of short stature. The patient had been diagnosed with TS at the age of 10 years and had received growth hormone therapy since that time. Height and weight of the patient were below the third percentiles, according to the Standard Growth Curve for Korean Children and Adolescents. As a result of the balloon dilatation procedure that the patient underwent at the age of 1.5 years to treat coarctation of the aorta, the patient had to take preventive antibiotics before invasive procedures. As the patient's intellectual level was normal, and the patient was very adaptive to treatment, no special behavioral control was necessary[16].
The facial features of TS are a senile (frequently heart-shaped) face; multiple ocular findings, depressed corners of the mouth; prominent, low-set ears[10]; and a short, broad, webbed neck[17,18]. In this case, the patient exhibited several features consistent with TS, such as a short and webbed neck and low posterior hairline (Fig. 3).
Reduced tooth crown size and altered tooth morphology have been observed in patients with this syndrome[5,19,20]. Many authors have explained that the X chromosome controls tooth size and shape, as well as tooth root morphology[21,22]. Enamel hypoplasia is observed frequently in patients with TS. Abnormalities of the X chromosome affect the secretion of enamel, thinning it, as demonstrated quantitatively, and causing enamel dysplasia, as observed qualitatively[23]. In the case reported here, intraoral findings included opaque white lesions and brown discoloration in the entire erupted dentition, caused by the hypomineralized type of generalized enamel hypoplasia.
Anomalies of root morphology also have been found to occur more often in patients with TS than in control subjects[23]. Increased numbers of first- and second-premolar roots have also been observed[24-27]. The most frequently observed deformities are two-rooted mandibular first and second premolars[26,27]. Kusiak et al.[24] examined the morphology of the mandibular premolar roots in 40 females with TS; they reported that two-rooted mandibular first premolars were observed in 34% of cases in the X monosomy (45,X) group, and two-rooted mandibular second premolars were observed in 39% of cases in the monosomy group. On the other hand, approximately 98% of the mandibular first premolars were single rooted; the incidence of two roots was 1.8% and three roots were found in 0.2% of all teeth studied. In anatomic studies, almost all (99.6%) mandibular second premolars were found to be single rooted. The occurrence of two roots (0.3%) and three roots (0.1%) is extremely rare[28,29]. Thus, it is extraordinary that all the mandibular premolars of this patient had two or three roots.
Furthermore, considering that the general prevalence of taurodonts was reported to range 2.5 - 11.3% of the human population, it is assumed to be a very rare case that all the mandibular premolars were diagnosed to be taurodonts[30]. Varrela et al.[31] suggested that the X chromosome influencing development of enamel may also be involved in the development of taurodontism. Taurodontism also has been reported that it is sometimes associated with several syndromes and anomalies, including amelogenesis imperfecta, ectodermal disturbance, Down syndrome, Klinefelter's syndrome, and oth-ers[31,32].
As the canal orifices of the bilateral mandibular second premolar roots were difficult to navigate, we decided to use a dental microscope during root canal treatment to ensure adequate visualization and treatment completion. It was also reported that careful exploration of the grooves between all orifices, especially with magnification had been recommended, since each taurodont tooth may have extraordinary root canals in terms of shape and number[33].
Patients with TS have an elevated risk of caries due to weak and thin enamel structure[21]. In addition, complicated root structures in the premolar region render root canal treatment difficult in these patients. And awareness and consideration of endodontic treatment difficulties in patients with TS is a crucial clinical factor.
In the treatment of TS patients, dentist should be aware of the possibility of systemic complications and strive for periodic dental follow-up for preventive maintenance. And if endodontic treatment is needed, the dentist should also take account for the complexity of the root shape and the variation of the root number in these patients.
IV. Summary
The patient in this case had TS and showed dental anomalies, such as dens evaginatus and taurodontism in all the mandibular premolars. Anomalies of root morphology have been found to occur more often in patients with TS, which make endodontic treatment challenging and require special handling. Due to the complexity of the root canal anatomy of the mandibular premolars of the patient, root canal treatment were completed with a dental microscope to ensure adequate visualization. Due to cardiac history, the patient had to take prophylactic antibiotics before each treatment.
The patients with TS may also have systematic problems such as cardiac or renal malformations, so in treating these patients it is important for clinicians not only to be aware of the characteristic intraoral findings, but also to make the patients have regular dental check-ups to prevent oral complications in advance.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






