



ŌģĀ. Introduction
With advances in the understanding of the causes and mechanisms of dental caries, the paradigm of dental caries treatment has shifted from the classical method of surgical intervention to the novel methods that prevent dental caries by intensive oral healthcare[1]. Prior experience of caries renders a vital indicator to predict the occurrence of dental caries in the future, and it is well established that the risk of developing permanent teeth caries is the highest at 6-12 years of age, that is, in the first few years after permanent teeth eruption[2]. Despite its decreasing trend, the prevalence of dental caries experience and the DMFT index remain high at 56.4% and 1.84 in permanent teeth of 12-year-old children and at 68.5% and 3.43 in primary teeth of 5-year-old children, respectively, based on Korea National ChildrenŌĆÖs Oral Health Survey in 2018[3].
The Korean government has provided free dental examination services for children and adolescents, but preventive dental care was not included in the public services. In this context, Seoul, the capital of the Republic of Korea, has provisioned a preventive dental healthcare services package named the Dental Preventive Health Services for Children (DPHSC) for kids at the age of 10 years, before the permanent dentition is fully developed. DPHSC, which was initially provided to approximately 19,000 students in 6 of 25 districts in Seoul in 2012, has been expanded annually and has been implemented for more than 46,000 students in all 25 districts since 2017. It is the first public service for preventive dental care, and includes dental examination, oral hygiene education, and preventive dental treatment. Dental examination includes visual examination, history taking, and panoramic X-ray visualization. Oral hygiene education includes proper plaque control using tooth brushing and flossing and instructions for diet and fluoride use. Preventive dental treatment includes professional oral prophylaxis, topical fluoride application, pit and fissure sealant, and scaling. The recipients of DPHSC visit designated dental clinics to avail services.
The aim of DPHSC is to establish an oral health care system that emphasizes prevention, rather than only being treatmentoriented; moreover, it is known that the participants have benefited from community-based dental care similar to DPHSC in clinical aspects such as decreased levels of dental caries and improved oral hygiene[4]. However, in view of the increasing importance of awareness on oral health or oral disease in recent years, the efficacy of DPHSC should be evaluated in more than just clinical terms[5].
Oral health-related quality of life (OHRQoL) refers to the impacts of oral health or dental diseases on daily functioning, activities and physical or psychological wellbeing and function[6]. The concepts of OHRQoL have been widely accepted in the medical or research area, especially in the case of chronic oral disease such as dental caries, which need active participation of patients themselves. It is vital to set a goal of treatment and establish the benefits of daily oral healthcare[6,7]. Approximately 20 OHRQoL scales have been developed for adults, but the scales for children are very limited[8]. Among these, the Child Oral Health Impact Profile (COHIP) questionnaire is the only instrument confirmed through validity and reliability testing for elementary school students in Korea[9]. Therefore, this study aims to examine the effects of DPHSC on the OHRQoL using COHIP.
ŌģĪ. Materials and Methods
1. Participants
This study was performed under the review of the Seoul National University School of Dentistry Institutional Review Board (#S-D20180020).
The beneficiaries of the DPHSC were 10-year-old elementary school students living in Seoul, and DPHSC was conducted from July to December in 2018. The inclusion criteria for this study were healthy students with age-appropriate literacy. The exclusion criteria were as follows: students with intellectual and cognitive disabilities and students who underwent orthodontic treatment. The participants of this study were randomly selected from all 20,802 beneficiaries from 11 districts of urban areas in Seoul where DPHSC data could be collected using computerized system. The number of samples was targeted to 110 with an effect size of 0.8 for the overall COHIP score and 0.5 for each subscale score (critical probability ╬▒ = 0.01, power 1- ╬▓ = 0.99, loss rate = 0.05, calculated with G*Power ver.3.1.9.2.) [10]. For randomization, we used a simple random sampling method by using random number generated by a computer.
2. Study design
The researchers approached the selected participants individually by phone and fully explained the study design to the students and their legal guardians on the day they visited the designated dental clinics to participate in the DPHSC. The participants with written informed consent were included in this study.
After the surveys were completed manually, DPHSC including dental examination, oral hygiene education, and preventive dental treatment was conducted on the same day. Prior to the implementation of DPHSC, all participating dentists have completed a national education program for oral examination. Dental examination in DPHSC yielded clinical results such as numbers of decayed and missing permanent teeth, malocclusion, and oral hygiene status, based on the contents of the program. Extent of dental caries was evaluated using the International Caries Detection and Assessment System (ICDAS) [11], and when a permanent tooth showed caries greater than ICDAS code 4, it was recorded as ŌĆ£decayed.ŌĆØ If agenesis of a permanent tooth was confirmed in a panoramic radiograph, it was recorded as ŌĆ£missingŌĆØ. Malocclusion was recorded based on the Index of Orthodontic Treatment Need (IOTN)[12,13]. If IOTN grade was greater than 3, the case was recorded as ŌĆ£malocclusion.ŌĆØ Oral hygiene status was evaluated by Patient Hygiene Performance (PHP) index[14], from a 0 (excellent) to 5 (poor) scale. Professional oral prophylaxis and topical fluoride application were conducted for all participants, and sealant and scaling were conducted for those diagnosed with the need for treatment. The same survey was conducted online, using a mobile link with Google Forms within 3 months after DPHSC.
3. Survey
The survey used COHIP, which contains 5 subscales and 34 items[7]. The Oral Health (OH) subscale contains ten items: ŌĆ£Pain/toothache,ŌĆØ ŌĆ£Breathing through the mouth,ŌĆØ ŌĆ£Discoloration of teeth,ŌĆØ ŌĆ£Crooked teeth or spaces,ŌĆØ ŌĆ£Sores or sore spots,ŌĆØ ŌĆ£Bad breath,ŌĆØ ŌĆ£Bleeding gums,ŌĆØ ŌĆ£Food sticking,ŌĆØ ŌĆ£Sensitivity with hot/cold,ŌĆØ and ŌĆ£Dry mouth.ŌĆØ The Functional Limitation (FL) subscale contains six items: ŌĆ£Trouble with chewing firm foods,ŌĆØ ŌĆ£Difficulty in eating,ŌĆØ ŌĆ£Trouble with sleeping due to teeth/face,ŌĆØ ŌĆ£Difficulty in pronouncing,ŌĆØ ŌĆ£Difficulty in being understood,ŌĆØ, and ŌĆ£Difficulty in keeping teeth clean.ŌĆØ The Social-Emotional Satisfaction (SES) subscale contains eight items: ŌĆ£Unhappy or sad due to teeth/face,ŌĆØ ŌĆ£Felt worried or anxious due to teeth/face,ŌĆØ ŌĆ£Avoided smiling,ŌĆØ ŌĆ£Felt looked different,ŌĆØ ŌĆ£Worried about othersŌĆÖ thinking,ŌĆØ ŌĆ£Felt shy or withdrawn due to teeth/face,ŌĆØ ŌĆ£Been bullied due to teeth/face,ŌĆØ and ŌĆ£Been irritated by questions about teeth/face.ŌĆØ The School Environment (SCE) subscale contains four items: ŌĆ£Absent from school due to teeth/face,ŌĆØ ŌĆ£Difficulty in paying attention due to teeth/face,ŌĆØ ŌĆ£Unwilling to speak due to teeth or face,ŌĆØ and ŌĆ£Unwilling to go to school due to teeth or face.ŌĆØ The Self-Image (SI) subscale contains six items: ŌĆ£Been confident due to teeth or face,ŌĆØ ŌĆ£Felt attractive with oneself due to teeth or face,ŌĆØ ŌĆ£Felt positive impression on teeth of oneself,ŌĆØ ŌĆ£Felt doing well on the behavior of oneself,ŌĆØ ŌĆ£Anticipate fine teeth after getting old,ŌĆØ and ŌĆ£Anticipate good health after getting old.ŌĆØ
The scores to each items in the survey utilized the 5-point Likert scale, which ranged from 0, being ŌĆ£almost all the time,ŌĆØ to 4, being ŌĆ£neverŌĆØ in OH, FL, SES, and SCE subscales asking negative symptoms of OHRQoL. In contrast, the scores of the items in the SI subscale asking positive perceptions about OHRQoL were ŌĆ£Strongly disagreeŌĆØ (0), ŌĆ£somewhat disagreeŌĆØ (1), ŌĆ£DonŌĆÖt agree or disagreeŌĆØ (2), ŌĆ£Somewhat agreeŌĆØ (3), and ŌĆ£Strongly agreeŌĆØ (4). The subscale scores were calculated by summing up the items scores included and the overall COHIP score by summing up the subscale scores. The overall COHIP score ranged from 0 to 136, of which a higher COHIP score indicated a better OHRQoL.
In the pre-survey, the participants were asked to respond based on their experiences for the past 3 months, while their experience after DPHSC was recorded in the post-survey.
4. Statistical analysis
In the pre-survey, split-half reliability for CronbachŌĆÖs alpha was used to validate the internal consistency. The construct validity of the questionnaire was examined with a correlation test between each subscale, and the discriminant validity was explored with a correlation test between the pre-survey and the results of the dental examination. SpearmanŌĆÖs rank correlation coefficient was used for all correlation tests. A Wilcoxon ranksum test was used to compare findings based on the dental examination results such as number of decayed teeth, number of missing teeth, malocclusion and PHP scores.
A Wilcoxon signed rank test was used to compare the COHIP scores between the pre- and post-surveys. CohenŌĆÖs d was used to identify the effect size, which was calculated by dividing the average difference between the pre- and post-survey by pooled standard deviation.
Ōģó. Results
A total of 110 students from urban areas in Seoul were enrolled and completed the pre-survey, and 107 students completed the post-survey (97.3%). The data from these 107 cases were analyzed (49 males and 58 females). Compared with the whole population of beneficiaries of DPHSC, the enrolled samples did not show any significant differences in gender ratio, the number of decayed permanent teeth, the number of missing permanent teeth, malocclusion, or oral hygiene status. Moreover, there were no significant differences in the number of decayed permanent teeth, missing permanent teeth, malocclusion, oral hygiene status, and pre-survey COHIP scores according to gender (Table 1).
A total of 32 students showed dental caries, having 2.94 ┬▒ 2.76 decayed teeth per average. Five missing teeth were observed in two students, one had one, and another had four. Malocclusion was observed in 18 students. The average PHP score of students was 2.23 ┬▒ 1.10. All 107 participants were given dental examination, oral hygiene education, professional oral prophylaxis, and topical fluoride application. Sealant was applied on 85 teeth from 36 students. Sixty students got their teeth scaled.
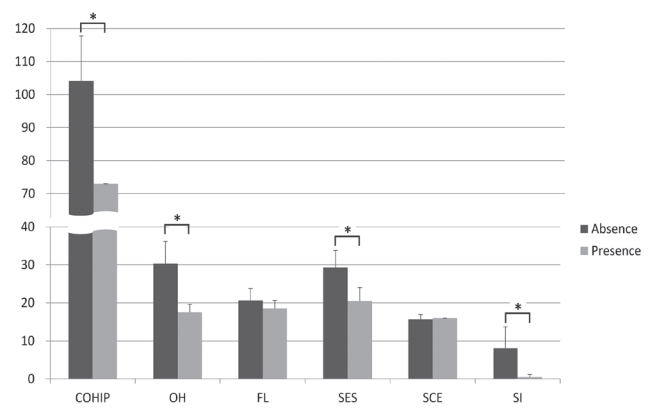
Table 2 shows the reliability and validity test results from the pre-survey. With CronbachŌĆÖs alpha above 0.75 (p < 0.01), high reliability was confirmed for the overall COHIP and the subscale scores. In terms of construct validity, the correlations between each subscales were less than 0.5 and significant (p < 0.05) except for the SI subscale, and all correlations between each subscales and overall COHIP were significant (p < 0.01). On the discriminant validity, the participants with missing teeth showed lower overall COHIP score, OH score, SES score, and SI score than those without missing teeth (p < 0.05). The subjects with decayed teeth showed lower FL score than those without decayed teeth (p < 0.01). With regard to malocclusion and PHP scores, there were no statistically significant results. Similar results were obtained using the Wilcoxon rank-sum test according to the presence or absence of decayed and missing teeth, as shown in Fig. 1 and Fig. 2.
The overall COHIP score, each subscale scores, and item scores in the pre- and post-survey are shown in Table 3. It was found that the average overall COHIP score was significantly increased after DPHSC (p < 0.001), as well as OH, FL, SES, and SI subscales; however, SCE subscale did not show any significant difference. Overall COHIP, OH and FL subscales showed large effect sizes. The distribution of the response frequencies before and after DPHSC is shown in Table 4. The majority of respondents reported ŌĆ£Almost neverŌĆØ or ŌĆ£NeverŌĆØ at the negative items (OH 58.0%, FL 82.2%, SES 86.0%, SCE 98.1%) while ŌĆ£strongly disagreeŌĆØ or ŌĆ£somewhat disagreeŌĆØ at the positive items (SI 42.0%). The most frequently reported symptoms were ŌĆ£Bad breathŌĆØ and ŌĆ£Food stickingŌĆØ in OH and ŌĆ£Difficulty in keeping teeth cleanŌĆØ in FL, and these items also showed the greatest improvement after DPHSC.
Among the participants with decayed teeth, the overall COHIP score and subscale scores did not change significantly after the implementation of DPHSC. In those with missing teeth, the overall COHIP, OH subscale and SES subscale scores increased significantly after the implementation of DPHSC (p= 0.009, 0.007 and 0.015, respectively).
ŌģŻ. Discussion
Socioeconomic inequalities are known to affect physical and mental health of children, which means that children living in socioeconomically deficient environments are in poor health[15]. These health inequalities are associated with material deficiencies, psychosocial factors, health related behavioral factor and socio-structural factors, and begin early in life and continue through childhood and adolescent to adulthood[15]. The same pattern occurs with oral health[16,17], and which is influenced by structural factors such as socioeconomic position, social capital, and social and economic policies and behavioral ones such as oral hygiene care, dietary regulation, and dental clinic visits[17-20]. Therefore, public oral care for all children is essential to ensure equity of oral health and to reduce the prevalence of dental caries[21-23].
The Korean government provides a total of three infant oral examinations for preschoolers and parent education services free of charge according to the Child Welfare Act, as well as oral examination services for 7, 10, 13, and 16 years of age according to the School Health Law. However, there has been little public preventive management intended for school-age children. Hence, DPHSC began to be implemented for some elementary schools in Seoul in 2012, being the first project in Seoul where public preventive program was targeted at school age. Expanding subjects every year, it is being conducted for all students in the fourth grade of elementary schools since 2017.
In the study that analyzed the effectiveness of communitybased dental care 2 years later in Korea[4], the participants showed decreased dental caries prevalence by 0.3% during 2 years, but the prevalence of dental caries in students not participating in the case increased by 11.4%. The occurrence of permanent teeth with caries experience increased by 0.09 in participating students but increased by 0.88 in nonparticipating students. In addition, the participants showed increased brushing frequency after lunch and decreased snack consumption rate[4]. The results mentioned above confirmed the effectiveness of the prevention and are consistent with other studies about public oral health care[21-23]. However, oral health does not simply mean absence of oral disease such as dental caries or good oral hygiene practice itself but refers to the state of the oral cavity and its related tissues that enable a person to eat, talk, and socialize without feeling ill or discomfort. Hence, multidimensional evaluation is required for proper evaluation[24]. Assessing OHRQoL is vital for multidisciplinary assessment of chronic diseases such as dental caries and can be used for public health policies[25,26]. In this study, we used COHIP, one of the questionnaires utilized for OHRQoL for children, to evaluate the effectiveness of DPHSC.
In this study, a high reliability based on >0.75 CronbachŌĆÖs alpha coefficient was verified in the five subscales as well as overall COHIP (p < 0.001). In the case of construct validity, there was a statistically significant relationship, not as high as 0.5 or less between inter-category correlation. It means that the questionnaire was useful to analyze the studentsŌĆÖ OHRQoL in various perspectives. However, the correlations between SI subscale and other subscales were not significant, and this may be related to the finding that the responses on the SI subscale showed a relatively even distribution compared with the responses on the other subscales (Table 4). Likewise, discriminant validity was also verified in that carious or missing tooth reduced COHIP score, and similar results are shown in the comparison of COHIP scores by Wilcoxon rank sum test (Figs 1 and 2). This is consistent with previous studies[27-31]. Overall, the COHIP questionnaire used in this study is thought to have adequate reliability and validity.
The mean score of overall COHIP was 103.59, and it was very similar to the results of a previous Korean study (103.3 ┬▒ 13.3), which targeted 2236 school-aged students in Gyeonggi province[9]. Seoul and Gyeonggi province are close to each other, with similar living standards and environment. So OHRQoL of students in these two regions was expected to be similar, and the result confirmed this, which enables us to conclude that the randomization process used in this study was valid.
In addition, this study confirmed that DPHSC improves the OHRQoL of children. The overall score of COHIP increased statistically after DPHSC and the effect size was very high (1.05). In the subscales, all but the SCE subscale showed a statistically significant improvement. Especially, OH and FL subscales showed very high effect sizes of 1.36 and 1.00. This result is meaningful, considering that DPHSC was aimed at all fourth grade elementary school children in Seoul, regardless of presence of oral diseases and oral education and preventive dental treatment being the main contents rather than dental restorative treatment. In fact, among 107 subjects, 32 students had dental caries, and the average number of carious teeth was only 0.88, <1 per patient, and only 2 students had missing teeth. In other words, these results came from the situation where there is not a great deal of discomfort from oral health status, and these results showed the possibility that DPHSC promoted participantsŌĆÖ awareness of oral health[5]. The effect size of SES, SCE, and SI was as low as <0.4, and the percentage of respondents with no or little in FL, SES, and SCE was >80%. This is also related to the fact that the oral health status of the participants was not so poor and the influence on these subscales was not significant. Also, the most frequent items reported by participants before DPHSC were ŌĆ£Bad breathŌĆØ, ŌĆ£Food stickingŌĆØ and ŌĆ£Difficulty in keeping teeth cleanŌĆØ, and these three items showed the greatest improvement after DPHSC. This may be because the participants have acquired and practiced knowledge about oral hygiene management through DPHSC.
The participants with decayed teeth did not show any significant changes after DPHSC; this could be because the number of decayed teeth was small, and dental restorative treatment was not included in DPHSC. Participants with missing teeth showed improvement in OHRQoL; probably because dentists provided thorough consultation about how to manage missing teeth and long-term treatment plan. However, because of the small number of participants with missing teeth, the results should be generalized with caution.
The limitations of this study are as follows. It is difficult to tell which factors have had the greatest impact on the OHRQoL because DPHSC is ongoing with dental examination, oral hygiene education, and preventive dental treatment. In addition, since the analysis included only the questionnaire within 3 months after DPHSC based on the results of previous study[32], there is a limitation to evaluate the long-term effect of the project. Moreover, we analyzed the data only from the students who participated in DPHSC; no control group was available to confirm the effects of confounders other than DPHSC because all 10-year-olds in Seoul are beneficiaries of DPHSC. Another limitation is that the dental examination results are based on the data from multiple dentists participating in DPHSC, despite the national education program before DPHSC. Also, the fact that the ways to fill out the OHRQoL questionnaire are different before and after DPHSC can be another confounder. The validity and reliability of OHRQoL using a mobile link with Google Forms should be verified.
In 2018, the DPHSC was performed only for 10-year-olds and limited in a one-time project. It is clear that prevention and oral health education are more effective than traditional dental treatment both clinically and cost-effectively[33] and a continuing preventive approach adhered causes changes in oral health behavior and cognition and in turn reduces oral disease[21,34]. But the long-term effect of a one-time project still needs clarification[35]. Hence, the researchers express that more sustained preventive health services and studies are needed to maintain oral health of children.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






