


ŌģĀ. Introduction
A new type of coronavirus infection (COVID-19) has spread throughout the world since it first was discovered in Wuhan, China, in December 2019. It is a respiratory syndrome caused by infection with SARS-CoV-2, an RNA virus[1].
In Korea, the first case of COVID-19 was confirmed in a citizen who visited Wuhan on January 20, 2020. On April 9, 2020, only 100 days after the outbreak of COVID-19 was first reported in China, the cumulative number of confirmed cases in the international community reached 1,500,800, and 87,700 people had died from the disease[2]. Because of the spread and risks of COVID-19, the World Health Organization has declared a ŌĆśpandemicŌĆÖ, which is a global epidemic[3]. The Korean Central Disaster and Safety Countermeasures Headquarters requested that citizens practice strong social distancing or refrain from going out altogether from March 22 to April 5, 2020. Citizens were also asked to postpone or cancel meetings, events, and travel within the time frame[4].
The spread of COVID-19 has changed peopleŌĆÖs daily lives. Religious activities were restricted as a result of large-scale outbreaks at Daegu religious meetings. At work, telecommuting was recommended during the social distancing period. In addition, the Korean Ministry of Education delayed the opening of kindergartens and elementary and secondary schools to prevent COVID-19 transmission. When the social distancing period was extended, online schooling began on April 10, and remote classes began to be conducted.
As a result, there are growing concerns about childcare for infants and school-age children. With postponement of school opening, parents and guardians are seeking ways to minimize care gaps, such as finding new care institutions or resources and taking vacations from work. Thus, parents and children are placed in stressful situations due to the combination of a limited social life, concerns over disease prevention, and childcare problems caused by COVID-19.
The outbreak of a new type of infectious disease causes emotional distress such as depression and anxiety[5]. In previous studies, the negative psychological experiences of the new epidemic were mainly examined from the perspective of fear or worry about the epidemic and emotional distress[5-7].
In February 2020, the number of new confirmed cases per month in Korea surged to 3,319 due to the mass infection centered on Daegu branch of the Shincheonji Church of Jesus, and the first wave of infections resulted in 6,636 confirmed cases in March 2020[8]. In April 2020, when the survey was conducted, the spread eased to 979 cases[8], but strong social distancing and online schooling were implemented. In Seoul, there were 372 confirmed cases in March 2020, and 183 confirmed cases in April 2020[8].
Against this background, this paper aims to study the effect of spread of COVID-19 on the mental state of school-age children and parents. Ultimately, the purpose of this study is to understand the potential emotional states within the coronavirus pandemic to determine needed considerations in the treatment and counseling process.
ŌģĪ. Materials and Methods
1. Participants
A survey was conducted for 113 school-age children and 123 parents of patients who visited Department of Pediatric Dentistry, Kyung Hee University Dental Hospital at Gangdong.
2. Study design
The survey, which was conducted from April 2, 2020 through April 25, 2020, consisted of a questionnaire that was administered via the direct writing method. The planning and informed consent process for this study was performed under the review of the Kyung Hee University Dental Hospital at Gangdong Institutional Review Board (IRB File No. KHNMC 2020-05-035).
In the questionnaire, basic questions asked of the adults were sex, age, occupation, monthly average household income, age of children, employment status of the couple, and primary caregiver for the child. To understand the changes in daily life caused by transmission of coronavirus infections, questions about recent weekly childcare arrangements, time spent retrieving coronavirus news and information, emotions around coronavirus related news, emotional changes due to the coronavirus pandemic, stress caused by closed schools and online learning, and the stress of contacting coronavirus related news were included. Self-examination scales for anxiety, depression and sleep disorders were included to measure the psychological state of the adults. The questionnaire for children consisted only of self-examination scale for anxiety, which can be answered relatively easily, to assess the psychological state of the children.
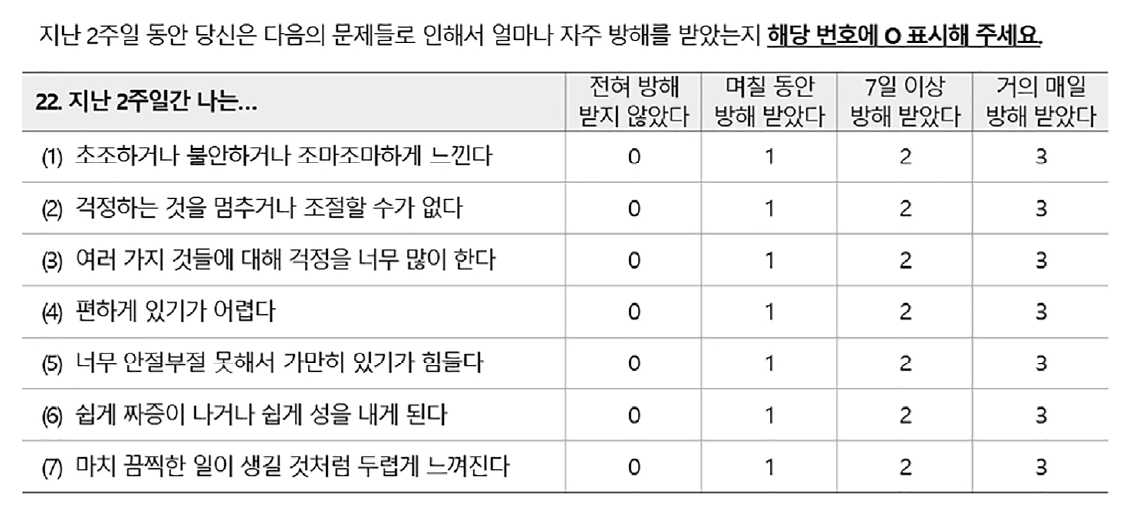
1) Generalized Anxiety Disorder-7 scale
The Generalized Anxiety Disorder-7 scale (GAD-7), one of the most widely used tools for anxiety self-examination, was developed in 2006 by Spitzer et al .[9]. It consists of a total of 7 questions, with each question answered on a scale of 0 - 3 points depending on the frequency of symptoms during the past 2 weeks (Fig. 1). The total scores ranged from 0 - 21, a score greater than 5 points indicates that anxiety is present[9].
2) Pittsburgh Sleep Quality Index
Sleep quality was assessed using the Pittsburgh Sleep Quality Index (PSQI), a self-report scale. It was developed by Buysse et al .[10] and was measured using the PSQI-K, the Korean version of the PSQI, which Sohn et al .[11] confirmed to ensure reliability and validity.
It consists of a total of 19 questions across the following 7 component areas: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, sleep drug use, and daytime dysfunction (Fig. 2). Scores for each component were calculated according to the PSQI evaluation method. The higher was the total score, the lower was the quality of sleep. A score greater than 5 points indicates a poor sleeper, while a score below 5 indicates a good sleeper.
3) Center for Epidemiologic Studies for Depression Scale
The Center for Epidemiologic Studies Depression Scale (CES-D) was developed by Radloff[12] in 1977 as a major screening tool for depression.
It consists of 20 questions that ask about the symptoms of the past week, with each question answered on a scale of 0 - 3 points (Fig. 3). A total score of 15 points or less is normal, 16 to 20 points corresponds to mild depression, 21 - 24 points corresponds to serious depression, and a score of 25 points or more corresponds to severe depression in need of expert treatment[12].
3. Statistical analysis
Frequency analysis was performed to analyze the basic characteristics of the participants. The following variables were analyzed among parents: employment status (employed or unemployed), monthly household income (less than or greater than six million won), changes in childcare arrangements, and coronavirus-related information searching time (less than 30 minutes, 30 minutes to an hour, over an hour). The independent samples t-test was conducted to compare the GAD-7, CES-D, and PSQI scores. In addition, by performing logistic regression analysis, odds ratios (OR), significance levels, and 95% reliability were calculated to evaluate factors affecting sleep quality, general anxiety disorder, and depression. In school-age children, the independent samples t-test was conducted to compare the GAD-7 scores between sexes. In addition, factors affecting GAD of school-age children were evaluated through logistic regression analysis. An independent t-test was conducted to compare changes in emotional state, stress levels due to online learning and Emergency Alert Messages about COVID-19, actual sleep time, and GAD-7 scores of parents and school-age children. SPSS Statistics 22.0 (Statistical Package for Social Science, version 22.0, IBM corporation, Chicago, IL, USA) was used for statistical analysis of the collected data.
Ōģó. Results
A total of 132 parents and 113 students was surveyed. Of these, 9 parents and 5 students who gave insincere answers were excluded. Of the 123 parents who were included in the study, 63.4% (n = 78) experienced emotional changes after the occurrence of COVID-19, and 61.8% (n = 76) answered that they felt anxiety (Table 1). Of the parent respondents, 54.5% and 55% felt the stress due to postponement of their childrenŌĆÖ s school and online learning and the stress of receiving Emergency Alert Messages about COVID-19, respectively (Table 1). In 108 school-age children, 19.5% experienced emotional changes, while 48.1% responded that they felt anxiety (Table 1). The stress felt by the children due to receiving Emergency Alert Messages was lower than that of the parents (Table 2, p = 0.000), and there was no significant difference between children and adults in GAD-7 score (Table 2).
Sleep disorders were experienced by 44.7% of the parents, 34.1% had an anxiety disorder and 17.1% had at least mild depression (Table 1).
ŌģŻ. Discussion
Previous research on new types of infectious diseases has focused on the fact that new types of infectious diseases induce severe, uncontrolled levels of distress that are more severe than stress in everyday life[13-15]. The outbreak of a new type of infectious disease causes emotional distress such as depression and anxiety[5]. In previous studies related to SARS and MERS, the negative psychological experiences of the new epidemic were mainly examined from the perspective of fear or worry about the epidemic and emotional distress[5-7]. This study investigated the emotional changes and stress of the participants due to COVID-19 and media usage time for collecting coronavirus-related information or news and compared them to identify differences between parents and children. GAD, CES-D, and PSQI were confirmed to investigate the psychological status of the participants. Finally, we investigated how individual characteristics of participants and coronavirus-related factors affect anxiety, depression, and quality of sleep.
The results of the study showed that 44.7% of the parents suffer from sleep disorders, 34.1% suffer from anxiety disorders, and 17.1% suffer from depression (Table 1). Most of the guardians were female, and the difference in mental health by gender was not confirmed. Some studies found that women feel more anxious than men[16,17]. Since the number of participants was not enough to identify the differences according to gender, so more studies will be needed in the future.
One side, anxiety disorders occurred in 20.4% of the 108 children (Table 1). Children had less time for searching coronavirus-related information or news and more sleep time than parents (Table 2), but nearly half (42.6%) of children were stressed by online lectures and 48.1% felt anxious when hear the news about COVID-19 (Table 1). Based on this, it was found that the spread of a new coronavirus infection also affects the emotional state of children.
Logistic regression analysis was performed to determine the factors, among demographic variables and COVID-19-related variables, that affect mental status.
In Korea, when various disasters such as typhoons, floods, earthquakes, fine dust, wars, and pandemic infectious diseases occur, Emergency Alert Messages are sent to mobile phones through the Cell Broadcasting Service system. Because of this, it is possible to selectively display a customized alarm in the disaster area. Due to the spread of COVID-19, Emergency Alert Messages with information on safety rules and areas of confirmed cases occurrence are being sent to each person in the area[18]. The stress experienced when parents received Emergency Alert Messages was identified as a contributor to changes in mental status (Table 3). Whether the cause of the stress was simply fatigue due to frequent text reception or distrust of the governmentŌĆÖs ability to cope, further research seems to be necessary.
Household income had a significant impact on the quality of sleep. however, this study did not take into account the potential variables and effects associated with income levels such as changes due to coronavirus situation. further studies can evaluate the influence of these socioeconomic variables.
In this study, coronavirus-related news or information searching time had no effect on mental state, and it was similar to the results of previous research. The study on the distress experienced by the general public for MERS infection also showed that media use frequency collecting MERS-related information did not affect the emotional distress experience[6].
Looking at the analysis of changes in daily life caused by COVID-19, changes in the childcare methods used were found in 26% of the respondents, but this was not related to the emotional changes experienced by the parents (p = 0.38).
So far, no research has been conducted about the emotions and stress of children in pandemic situation. In this study, emotional changes, stress, and anxiety caused by COVID-19 in children were investigated at an exploratory level in the absence of any previous studies on the psychological effects of the new infectious disease on school-age children. Future studies will be able to accumulate the results of our research and contribute to understanding the emotional state of children in a pandemic situation and applying them to medical treatment and counseling process. In children, 48.1% felt anxious when they heard the news about COVID-19 (Table 1) and anxiety disorders appeared as the level of emotional change after COVID-19 increased (Table 4). This mental status could cause anxiety about dental visits, which could ultimately lead not to visit appointments such as regular check-ups if children do not have symptoms, or poor cooperation in dental care. Behavior control and counseling with guardians are important part of the dental treatment in pediatric dentistry. Under the epidemic of new infectious diseases, we should understand the anxiety of children and guardians who report to the hospital and consider it in the dental care and counseling process.
Several studies have shown that psychological condition impacted on oral health. According to a study, people with depression brushed their teeth less frequently and more likely not to receive dental treatment even if they had dental problems[19]. A survey of adolescents showed both males and females who reported symptoms of depression had an increased poor hand and oral hygiene including brushing their teeth less than daily[20]. As children spend more time living at home due to the spread of COVID-19, the intake of sugars such as snacks and instant foods increases[21,22]. In Korea, tooth brushing after meals is not carried out in schools or kindergartens to prevent the transmission of coronavirus. Such changes of situations and oral health behavior due to mental status can have deleterious effects on oral health, such as an increased risk of caries. In this situation, Oral management and dental caries prevention education for children should be emphasized. If it were possible to compare oral hygiene status of children before and after COVID-19 situation, it might have been possible to study the effects of epidemics such as COVID-19 on the oral health of children. Further research on this may help to evaluate the relationship between the pandemic situation and oral health.
The first limitation of this study is the small sample size, which limits the generalizability of these results to the psychological state of all parents and children. Second, the questionnaire did not include many questions about changes in daily life after COVID-19, so others factor may exist. Third, psychological evaluations were conducted using subjective scoring questionnaires, as opposed to through professional counseling. In addition, evaluation of changes in prevalence before and after COVID-19 situation was not possible.
Ōģż. Conclusion
In light of COVID-19 transmission in the community, a survey was conducted of parents and children who visited Department of Pediatric Dentistry. It was determined that 17.1% of parents had depression, 44.7% had sleep disorders, and 34.1% had anxiety. Of the children, 20.4% were experiencing anxiety. The higher was the stress due to receiving emergency alerts related to COVID-19, the more severe was the depression and anxiety symptoms. In children, the greater was the degree of emotional change felt after COVID-19, the more severe were the symptoms of anxiety.
Under the epidemic of new infectious diseases, we should understand the mental status of children and guardians who report to the hospital.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






