소아 청소년에서 하악공 및 하악소설의 위치에 대한 CBCT 분석
Assessment of the Position of the Mandibular Foramen and Mandibular Lingula in Children and Adolescents using CBCT
Article information

Abstract
이 연구의 목적은 CBCT를 이용해 소아에서 연령에 따른 하악공과 하악소설의 위치 및 하악소설의 형태를 평가하고, 하치조신경 전달마취 시 고려할 수 있는 자입점을 제시하는 것이다.
과잉치 발거 또는 매복치 평가를 위해 CBCT를 촬영한 만 6 - 16세의 영상을 수집하였다. 연령에 따라 만 6 - 7세, 10 - 11세, 15 - 16세의 3군으로 분류하였으며 군당 남녀 각 30명씩을 포함하여 총 180명의 하악지 좌우가 분석되었다. 좌우 측의 하악소설로부터 하악지의 전연, 후연, 상연, 하연까지의 최단거리를 계측하고 하악소설과 하악공 사이의 최단거리, 교합평면에 대한 하악소설과 하악공 사이의 수직거리를 각각 측정하였다. 하악소설의 형태를 기준에 따라 4가지 형태로 분류하여 평가하였다.
하악지의 전후방 및 수직적 기준점으로부터 하악소설의 위치는 연령에 따라 모든 방향으로 증가하는 양상을 보였으며 하악소설과 하악공 사이의 거리 역시 연령에 따라 증가하는 양상을 보였다. 교합평면에 대한 하악소설 및 하악공의 거리는 연령에 따라 상방으로 이동하는 양상을 보였다. 하악소설의 형태는 삼각형 형태가 가장 많았고 결절형, 절두형, 동화형 순이었으며 연령에 따른 차이는 보이지 않았다.
연구를 통해 수평적인 마취의 자입점은 하악지의 전연으로부터 연령에 따라 각각 17 mm, 18 mm, 19 mm로 증가된 지점이 권장되며, 수직적인 마취의 자입점은 연령에 따라 교합평면 상방 2 - 3 mm, 5 - 6 mm, 9 - 10 mm로 자입점을 높이는 것이 권장된다.
Trans Abstract
The purpose of this study is to evaluate the position of the mandibular foramen and location and morphological characteristics of the mandibular lingula using Cone-Beam Computed Tomography (CBCT).
Mandibular CBCT images of children aged 6 - 16 years were collected. A total of 180 patients were divided into 3 groups, 6 - 7, 10 - 11 and 15 - 16 years, with 30 male and female patients per group. Either side of the ramus was analyzed. The shortest distances from the anterior, posterior, superior and inferior border of the ramus to the mandibular lingula were measured. The shortest distance between the mandibular lingula and the mandibular foramen was also measured. The vertical distance from the mandibular lingula and the mandibular foramen to the occlusal plane was measured. The shapes of the mandibular lingula was classified into 4 types according to the criteria.
The distances of the mandibular lingula from the anteroposterior and vertical reference points of the ramus increased in all directions with age. The distance between the mandibular lingula and the mandibular foramen also increased with age. The location of the mandibular lingula and the mandibular foramen in relation to the occlusal plane moved upwards with age. The most common shape of the mandibular lingula was triangular, followed by nodular, truncated and assimilated, and there was no difference in the shape according to age.
It is recommended that the horizontal insertion point of the anesthesia from the anterior border of the ramus increased to 17 mm, 18 mm, and 19 mm according to the age groups. It is also suggested that the vertical insertion point increased by 2 - 3 mm, 5 - 6 mm and 9 - 10 mm above the occlusal plane according to the age groups.
Ⅰ. 서 론
치과 시술 중 통증 조절은 치료의 효율뿐만 아니라 환자와 치과의사 사이에 신뢰를 쌓고 환자의 두려움과 불안을 완화시키기 위해 중요하다. 하치조신경 전달마취는 치과치료 시 효과적인 통증 조절을 위해 흔히 시행되는 술식이지만 15 - 20%의 실패율이 보고된다[1,2]. 실패의 원인은 해부학적 구조의 다양성, 부가적인 신경의 분포, 심리적 공포, 환자의 병리 상태, 주사침의 부정확한 위치로의 자입 등과 연관되어 있다[3]. 마취의 실패로 인해 국소 마취제가 반복 적용될 경우 소아환자의 부정적인 행동을 초래할 수 있으며 필요 이상의 용량이 투여될 위험이 있다.
하악소설(Mandibular lingula)은 하악지의 내측면에 있는 혀 모양의 골 융기로 하악공(Mandibular foramen) 및 하악신경에 근접해 있어 하치조신경 전달마취를 위한 해부학적 지표로 고려되며 하악골의 외과적 수술 시 하치조신경의 손상을 피하기 위해 평가되는 기준점이다[4]. 성공적인 하치조신경 전달마취의 효과를 얻기 위해서는 하치조신경이 하악공으로 들어가기 전에 국소마취제가 주입될 수 있도록 주사침의 자입 시 하악소설을 포함하는 익돌하악간극(Pterygomandibular space)을 향해 정확하게 접근하는 것이 중요하다[5].
하악공과 하악소설의 위치는 어린이가 성장함에 따라 달라지므로 연령에 따른 자입점의 높이를 고려하는 것은 중요하다. 선행된 연구에 따르면 하악공의 높이는 유치열에서 교합면에 가깝고 연령에 따라 점차 높아진다고 보고되었다. 이러한 하악공의 위치 변화를 고려하여 하치조신경 전달마취 시 유치열에서는 교합면 가상선보다 약간 후하방으로 자입하며 연령에 따라 높여서 자입할 것을 제시하고 있다[6]. 하악소설의 형태 또한 개인에 따른 해부학적 다양성이 크며 이러한 차이는 하치조신경 전달마취 실패의 원인으로 작용할 수 있다[7].
Cone-Beam Computed Tomography (CBCT) 영상은 하악의 해부학적 지표들을 시각화하기에 파노라마 방사선 영상에 비해 우수하고, Medical CT와 비교했을 때 방사선 노출량이 적고 스캔 시간이 짧으며 데이터 재구성이 쉽다는 장점이 있다[8,9]. 이처럼 3차원 CBCT는 복잡한 구조물이 중첩되는 두경부 영역에 적용되기에 다양한 이점이 있으나 소아에서 CBCT를 촬영하는 경우가 드물고 한국인 소아 청소년을 대상으로 하악공 및 하악 소설의 위치와 형태에 대해 CBCT를 이용하여 평가한 연구는 많지 않다.
이 연구는 소아 청소년에서 CBCT를 이용해 연령에 따른 하악골 내 하악공과 하악소설의 위치를 계측하고 하악소설의 형태에 대하여 분석하여, 하악지의 해부학적 구조에 대한 이해를 돕고 하치조신경 전달마취의 성공률을 높이는 데 도움이 되고자 수행되었다.
Ⅱ. 연구 대상 및 방법
1. 연구 대상
2016년 1월부터 2020년 5월까지 과잉치 발거 및 매복치 평가를 위해 전남대학교 치과병원에 내원하여 CBCT를 촬영한 만 6 - 16세 환자의 영상을 수집하였다. 연구 대상의 선정 기준은 다음과 같았다.
1) 포함 기준
(1) CBCT 촬영 당시의 연령이 만 6 - 16세에 해당하는 자
(2) CBCT 촬영 동의서에 서명한 자
(3) 전체 하악골을 포함하여 촬영한 영상
2) 제외 기준
(1) 하악에 병리학적 병변이 있는 자
(2) 악안면 기형이 있는 자
(3) 하악의 외상 또는 수술의 기왕력이 있는 자
(4) 악골의 비대칭을 보이는 자
(5) 환자의 움직임에 의해 심한 왜곡이 있는 영상
총 180명의 환자를 초기 혼합치열기, 후기 혼합치열기, 영구치열기에 해당하는 만 6 - 7세, 10 - 11세, 15 - 16세의 3군으로 각각 분류하였으며 각 군당 60명(남: 30명, 여: 30명)의 하악지 좌우를 분석하였다(Table 1). 해당 연구 대상의 표본 수는 G power (version 3.010, Franx Faul. Universitat kiel, Germany)에서 유의수준 α = 0.05, 95% power, effect size = 0.80로 계산하여 산정하였다. 방사선 영상을 바탕으로 한 이 연구의 프로토콜은 전남대학교 치과병원 생명의학연구윤리심의위원회(Institutional Review Board, IRB)의 승인을 받고 진행되었다(IRB NO.: CNUDH-EXP-2020-015).

The distribution of the study subjects
2. 연구 방법
CBCT 영상은 CS9300(Carestream Dental, USA)로부터 얻어졌으며 이는 OnDemand3D software(Cybermed, Korea)프로그램의 2차원 및 3차원 이미지로 구현되었다. 하악지의 전연, 후연, 상연, 하연의 최심점을 각각의 기준점으로 설정하고, 하악의 제1유구치 또는 제1소구치의 설측 교두로부터 동일 분악의 제1대구치 또는 제2대구치까지의 설측 교두를 잇는 선을 교합평면으로 설정하였다(Table 2, Fig. 1). 각 기준점과 하악소설 사이의 거리를 측정하기 위해 직선 계측 도구가 사용되었다. 모든 항목의 계측은 양측에서 이루어졌다.
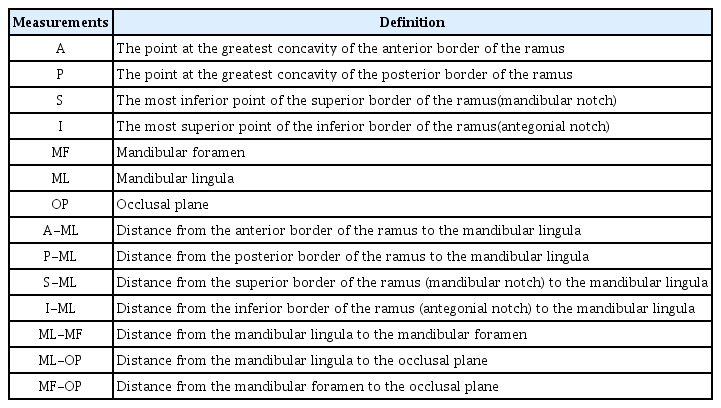
Measurements of mandibular ramus morphology

Reference points of the mandibular ramus. A: anterior border, P: posterior border, S: superior border(mandibular notch), I: inferior border(antegonial notch), ML: mandibular lingula, MF: mandibular foramen, OP: occlusal plane.
1) 하악소설의 전후방적 및 수직적 위치
하악지 내에서 하악소설의 위치를 평가하기 위해 하악지의 전연, 후연, 상연, 하연의 가장 깊은 지점으로부터 하악소설까지의 최단거리(A-ML, P-ML, S-ML, I-ML)를 각각 측정하였다(Table 2, Fig. 2A).
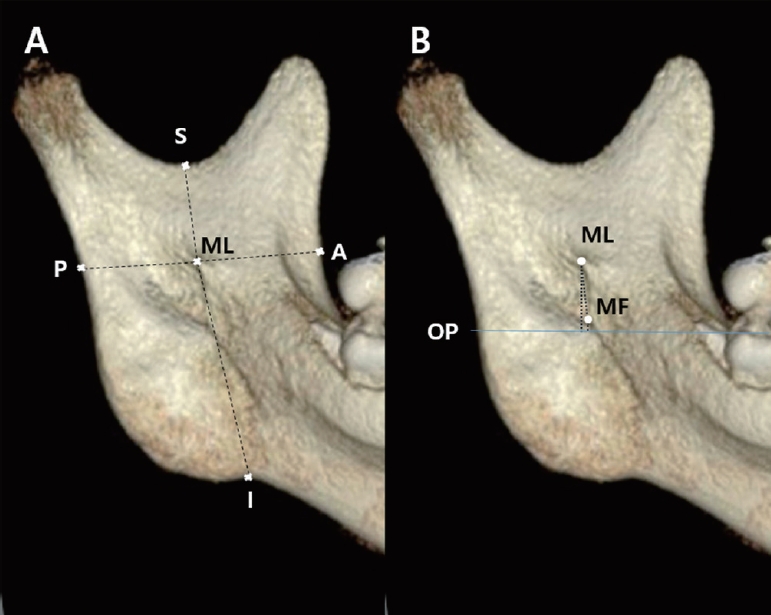
Measurements of mandibular lingula and mandibular foramen from the various landmarks. (A) A-ML: Distance from the anterior border of the ramus to the mandibular lingula, P-ML: Distance from the posterior border of the ramus to the mandibular lingula, S-ML: Distance from the superior border of the ramus to the mandibular lingula, I-ML: Distance from the inferior border of the ramus to the mandibular lingula. (B) ML-MF: Distance from the mandibular lingula to the mandibular foramen, ML-OP: Distance from the mandibular lingula to the occlusal plane, MF-OP: Distance from the mandibular foramen to the occlusal plane.
3) 교합평면에 대한 하악소설 및 하악공의 위치
교합평면에서 하악소설과 하악공까지의 수직거리(ML-OP, MF-OP)를 각각 측정하였으며 교합평면보다 상방은 양수로, 하방은 음수로 표시하였다(Table 2, Fig. 2B).
4) 하악소설의 형태
하악소설의 형태는 Tsai 등[10]이 제안한 분류를 이용하여 결절형(Nodular), 삼각형(Triangular), 절단형(Truncated), 동화형(Assimilated) 4가지로 분류하였다(Fig. 3). 결절형의 하악소설은 결절 모양으로 크기가 다양하며 정점을 제외하고 하악지에 병합되어 있다. 삼각형의 하악소설은 밑면이 넓고 둥글거나 뾰족한 꼭짓점이 있는 형태이며, 절단형의 하악소설은 상단이 절단된 형태로 사각형의 형태를 가진다. 동화형의 하악소설은 하악지와 완전히 합쳐진 형태이다.
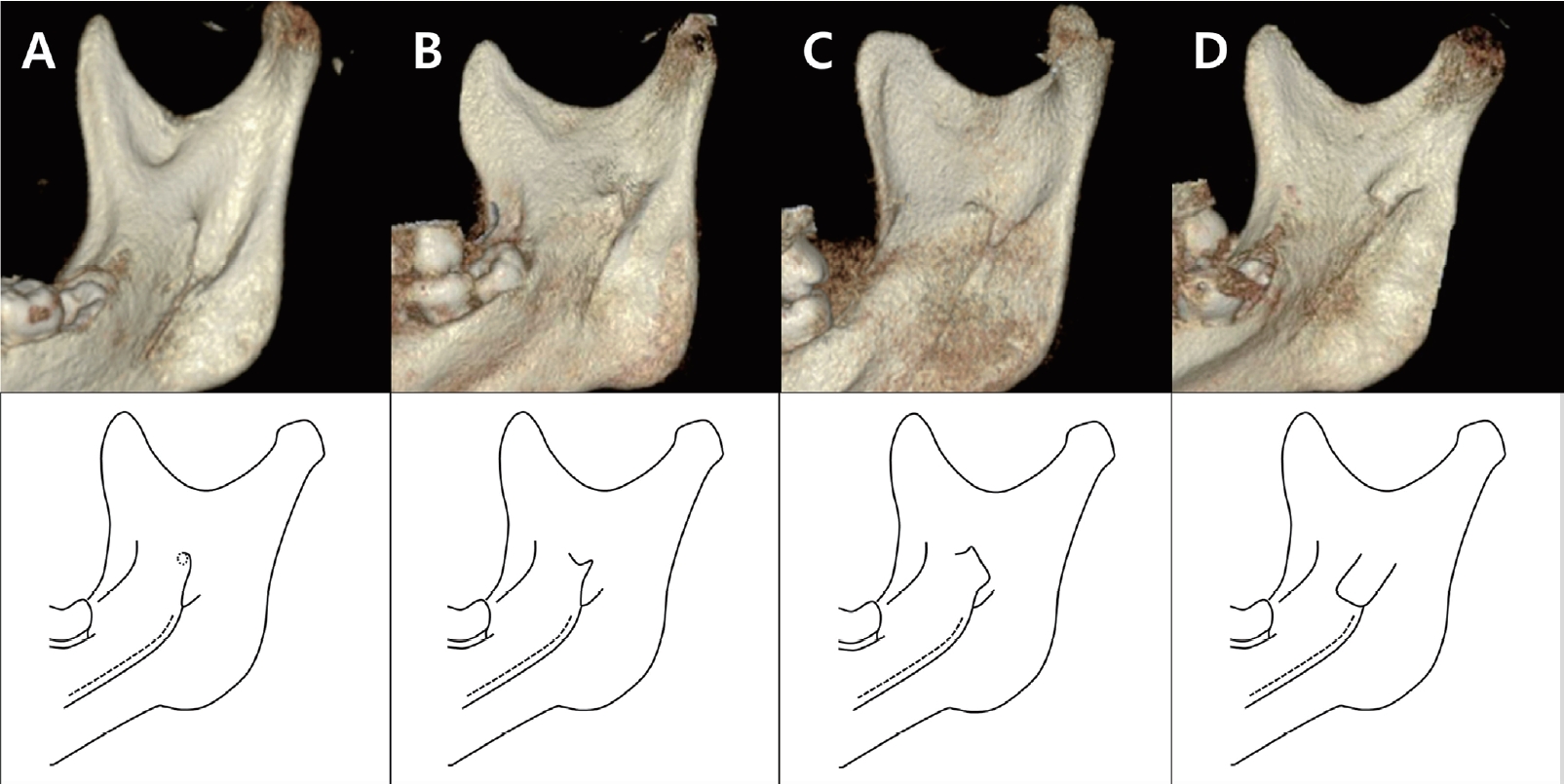
The shapes of the lingula are classified into 4 types on CBCT images. (A) Nodular. (B) Triangular. (C) Truncated. (D) Assimilated.
3. 표준 일관성 평가
50개의 표본을 무작위로 골라 조사자 내 재현성을 평가하였다. 하악소설의 위치와 형태에 대해 1명의 치과의사가 같은 CBCT 이미지를 4주 간격으로 판독하였고 조사자 내 신뢰도인 Intraclass Correlation Coefficient (ICC) 값을 구하였을 때 모든 항목에서 0.87 이상으로 나타났다.
4. 통계분석
각 항목에 대해 평균 및 표준편차를 구하였다. 각 항목에서 좌우에 따른 차이 유무를 확인하기 위하여 대응 표본 t-검정(Paired t-test)을, 성별에 따른 차이 유무를 확인하기 위하여 독립 표본 t-검정(Independent t-test)을 사용하여 분석하였다. 또한 연령별 차이가 있는지 통계적으로 검증하기 위해 일원 분산분석(One-way ANOVA)을 사용하였으며, 형태에 대해서는 카이제곱검정(Chi-square test)을 사용하여 분석하였다. 통계분석은 SPSS 22.0(Statistical Package for Social Sciences, IBM Corp., USA)을 이용하여 평가하였다.
Ⅲ. 연구 성적
1. 하악지에 대한 하악소설의 전후방적 위치
하악지 전연에서 하악소설까지의 거리(A-ML)는 6 - 7세 16.68 ± 1.64 mm, 10 - 11세 18.28 ± 2.25 mm, 15 - 16세 19.43 ± 2.47 mm로 연령에 따라 증가하는 양상을 보였다(Table 3, p = 0.000). 모든 연령에서 동일한 군 내에서는 좌측과 우측의 측정값에 차이를 보이지 않았고(Table 4, p = 0.063, 0.055, 0.423), 남녀 간 차이도 나타나지 않았다(Table 3, p = 0.410, 0.631, 0.283).

Comparison of measurements in males and females per age category
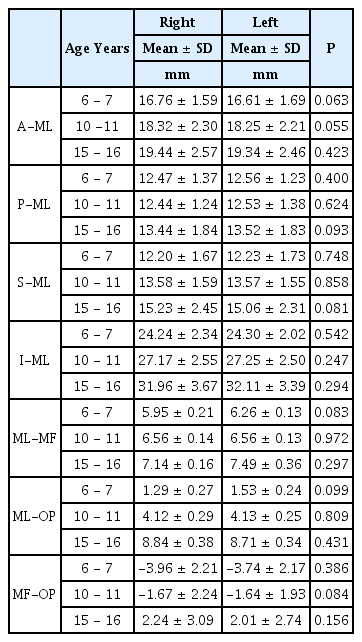
Comparison of measurements between the right and left sides
하악지 후연에서 하악소설까지의 거리(P-ML)는 6 - 7세 12.52 ± 1.30 mm, 10 - 11세 12.49 ± 1.31 mm, 15 - 16세 13.48 ± 1.83 mm로 15 - 16세 연령에서 유의하게 증가하는 양상을 보였다(Table 3, p = 0.000). 동일한 연령에서는 성별에 따른 차이를 보이지 않았다(Table 3, p = 0.177, 0.794, 0.134).
하악지의 전후방 거리에 대해 하악지 전연에서 하악소설까지의 거리의 비(A-ML/A-P)는 6 - 7세 57.12%, 10 - 11세 59.31%, 15 - 16세 58.93%로 모든 연령에서 하악지의 전연과 후연의 중앙보다 약간 후방에 위치하였으며, 남녀 모두 10 - 11세에 증가하는 양상을 보였다(Table 5, p = 0.000, 0.039).
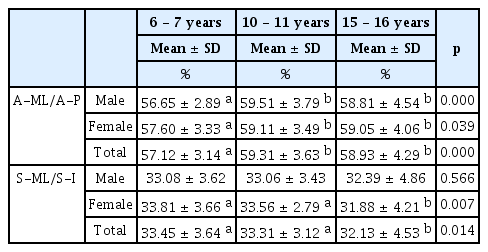
Comparison of the horizontal and vertical location of the mandibular lingula among age groups
2. 하악지에 대한 하악소설의 수직적 위치
하악지 상연에서 하악소설까지의 거리(S-ML)는 6 - 7세 12.21 ± 1.69 mm, 10 - 11세 13.58 ± 1.56 mm, 15 - 16세 15.14 ± 2.37 mm이었으며, 하악지 하연에서 하악소설까지의 거리(I-ML)는 6 - 7세 24.27 ± 2.18 mm, 10 - 11세 27.21 ± 2.51 mm, 15 - 16세 32.04 ± 3.52 mm로 연령에 따라 각각 증가하는 양상을 보였다(Table 3, p = 0.000). 좌우의 측정값은 동일한 군에서 차이를 보이지 않았다(Table 4, p = 0.748, 0.858, 0.081, p = 0.542, 0.247, 0.294). 하악지 상연에서 하악소설까지의 거리는 15 - 16세 군에서 남자가 큰 값을 보였고(Table 3, p = 0.000) 하악지 하연에서 하악소설까지의 거리는 6 - 7 세와 15 - 16세 군에서 남자가 여자보다 유의하게 큰 값을 보였다(Table 3, p = 0.036, 0.000).
하악지의 상하 높이에 대해 하악지 상연에서 하악소설까지의 거리의 비(S-ML/S-I)는 6 - 7세에 33.45%, 10 - 11세에 33.31%, 15 - 16세에 32.13%로 모든 연령에서 하악지의 상연에서 1/3높이에 하악소설이 위치하는 값을 보였으며, 15 - 16세 여자에서 유의하게 감소하는 양상을 보였다(Table 5, p = 0.007).
3. 하악소설과 하악공 사이의 거리
하악소설과 하악공 사이의 거리(ML-MF)는 6 - 7세 6.18 ± 0.97 mm, 10 - 11세 6.56 ± 1.02 mm, 15 - 16세 7.15 ± 1.19 mm로 연령이 증가할수록 증가하는 값을 보였다(Table 3, p = 0.000). 남자에서는 15 - 16세 군에서 증가하는 양상을 보였고(Table 3, p = 0.000), 여자에서는 10 - 11세 군에서 증가하는 양상을 보였다(Table 3, p = 0.000). 6 - 7세 군에서 남자가 여자에 비해 유의하게 큰 값으로 나타났다(Table 3, p = 0.008).
4. 교합평면에 대한 하악소설의 위치
교합평면에 대한 하악소설의 위치(ML-OP)는 6 - 7세 1.47 ± 1.94 mm, 10 - 11세 4.13 ± 2.06 mm, 15 - 16세 8.78 ± 2.78 mm에 위치하는 것으로 나타났다(Table 3). 남녀 모두 연령에 따라 하악소설이 교합평면을 기준으로 점차 상방으로 이동하는 양상을 보였다(Table 3, p = 0.000). 하악소설의 위치는 모든 연령대에서 남자보다 여자에서 상방에 위치하는 것으로 나타났으나 남녀의 차이는 10 - 11세에서만 유의한 것으로 나타났다(Table 3, p = 0.031). 하악소설이 교합평면 하방에 위치하는 경우가 6 - 7세에 21.7%였고 나머지 연령에서는 모두 상방에 위치하였다(Table 6).

Position of the mandibular lingula and mandibular foramen relative to the occlusal plane
5. 교합평면에 대한 하악공의 위치
교합평면에 대한 하악공의 위치(MF-OP)는 6 - 7세 -3.85 ± 2.19 mm, 10 - 11세 -1.65 ± 2.08 mm, 15 - 16세 2.12 ± 2.91 mm에 위치하는 것으로 나타났다(Table 3). 남녀 모두 연령에 따라 하악공이 교합평면 하방에서 상방으로 이동하는 양상을 보였다(Table 3, p = 0.000). 하악공의 위치는 모든 연령에서 남자보다 여자에서 상방에 위치하는 것으로 나타났으며 통계학적으로 유의한 차이가 있었다(Table 3, p = 0.002, 0.047, 0.017). 하악공이 교합평면 하방에 위치하는 경우가 6 - 7세에 남녀 모두 100%, 10 - 11세 남자에서 90%, 여자에서 70%, 15 - 16세 남자에서 26.7%, 여자에서 6.7%로 나타났다(Table 6).
6. 하악소설의 형태
하악소설의 형태는 양측성으로 동일한 형태가 편측성으로 다른 형태를 보이는 경우보다 많았다(Table 7). 모든 연령에서 가장 흔한 형태는 삼각형이었으며 결절형, 절단형, 동화형 순으로 나타났다. 연령 증가에 따른 형태의 차이는 나타나지 않았다(Table 8, p = 0.818). 형태에 따른 하악소설의 하악골 내 위치는 15 - 16세 연령에서 삼각형 형태가 결절형과 동화형보다 후방에 위치하였으며(Table 9, p = 0.000), 10 - 11세 연령에서 삼각형 형태가 결절형과 동화형에 비해 상방에 위치하였다(Table 9, p = 0.037).

The symmetry of the shape of the mandibular lingula

Comparison of the lingula shape between the age groups
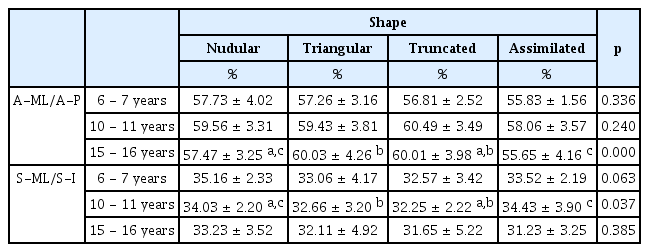
Position of the mandibular lingula according to the shape
Ⅳ. 총괄 및 고찰
하악공과 하악소설의 위치는 성장과 발달에 의해 영향을 받는다. 성장기에 하악지의 전방 경계와 치조골의 치조정 부분에서 일어나는 치아의 맹출과 탈락, 하악골의 성장은 하악공의 위치 변화를 야기하여 하치조신경 전달마취의 성패에 영향을 미칠 수 있으므로, 연령에 따른 하악공과 하악소설의 위치 변화를 이해하는 것은 중요하다[11].
하악소설의 전후방적 위치에 대한 분석은 전달마취 시 자입점의 수평적인 위치 정보를 제공한다. 이러한 고려는 마취 주사가 너무 전방으로 위치되어 골 접촉이 이루어지지 않거나, 후방으로 위치되어 이하선 또는 안면신경이 손상되는 것을 피하기 위해 중요하다[12]. Johan 등[13]은 6 - 18세 환자의 CBCT를 이용하여 하악소설의 위치를 평가한 연구에서 하악지의 전연과 하악소설 사이의 거리를 연령에 따른 큰 차이 없이 약 18 mm라고 보고하였으며, 이 위치를 하치조신경 전달마취의 수평적인 자입점으로 권장하였다. 이 연구에서도 전체 연령의 평균은 약 18 mm로 나타났으며, 연령에 따라 약 17 - 19 mm까지 증가된 결과를 보였다. 또한 이전에 수행된 연구들[13,14]에서와 유사한 결과로 이 연구의 모든 연령에서 하악소설이 하악골의 중심보다 후방인 57 - 59%의 지점에 위치하였다. 이를 종합적으로 고려해 볼 때, 하악지의 전연과 후연을 동시에 촉지하여 중앙보다 후방인 약 60% 지점, 하악지의 전연을 기준으로는 연령 증가에 따라 각각 17 mm, 18 mm, 19 mm 위치에 자입점을 설정하는 것이 마취의 성공률을 높일 수 있다.
하악지의 상연과 하연으로부터 하악소설까지의 거리는 하악골 내에서 하악소설의 수직적인 해부학 정보를 제공한다. 다만 하악지 상연은 촉지가 어려워 임상적인 참고가 어렵다. 이 거리는 연령이 증가함에 따라 각각 유의하게 증가하였다. 증가의 정도는 다르지만 모든 연령에서 하악소설의 수직적인 위치가 하악지의 상연을 기준으로 32 - 33% 지점에 있는 결과를 통해 하악 소설이 하악골의 중심보다 상방에 위치함을 알 수 있었다. 특히 이러한 결과는 이전의 소아를 대상으로 평가한 연구[15]뿐만 아니라 한국인 성인을 대상으로 평가한 연구[16]에서도 유사하게 보고되었으며, 이는 연령에 따른 큰 차이없이 비교적 일정한 수직적 위치 관계가 유지되는 것으로 보인다. 즉, 상대적으로 하악지의 상방에 비해 하방의 성장량이 크나 전체적인 비율에는 큰 차이가 없는 것으로 해석된다.
하악소설과 하악공 사이의 거리는 마취 시 자입점으로부터 하치조신경이 하악골 내부로 들어가는 지점 사이의 거리이며, 마취액이 확산되는 범위이다. 연구 결과 이 거리는 6 - 7 mm의 범위에서 연령에 따라 유의하게 증가하는 양상을 보였으며 이는 하악골의 전후방적, 수직적 성장에 따른 증가로 생각된다. Sekerci 등[17]과 Monnazzi 등[18]은 어린이를 대상으로 한 연구에서 이 거리를 약 5 - 6 mm로 보고하였으며, 성인을 연구한 Sekerci와 Sisman[4]는 7.9 mm, Alves와 Deana[7]는 8 - 10 mm로 보고하여 어린이에 비해 성인에서 더 증가된 값을 보였다. 그러나 연구마다 계측 기준에 차이가 있기 때문에 동일 선상에서 결과 값을 비교할 수는 없고, 추후 이 연구와 동일한 기준으로 성인의 하악골을 분석하여 다양한 연령에 대한 비교가 필요할 것이라 생각된다.
교합평면에서 하악공과 하악소설까지의 수직거리의 측정은 해부학적인 위치 정보를 얻고, 국소 마취제를 투여하기 위한 자입점의 높이를 설정하는 데에 도움이 되며 이는 곧 전달마취의 성패로 이어질 수 있다. 개구 및 견인에 따라 변위되는 연조직에 비해, 구치부 교합평면은 자입점의 설정과 관련된 경조직 참고점으로서 의미가 있다. 그러나 소아의 하치조신경 전달마취 시 교합평면을 기준으로 한 자입점의 위치 설정에 대해서 아직까지 일치된 사항은 없으며 다양한 권고사항만이 제시되고 있다.
여러 연구들에 따르면 유치열의 하악공은 교합평면 하방에 위치하므로 교합평면 후하방으로 자입하며 연령 증가에 따라 자입점을 높이도록 하였다[6,19]. 한편 Kanno 등[1]은 7 - 8세에서는 교합평면 상방 6 mm, 9 - 10세에서는 교합평면 상방 10 mm에 자입하도록 권고하였으며, Pereira 등[20]은 8세 미만에서는 자입점을 교합평면 하방에, 8세 이상은 교합평면 상방에 둘 것을 제안했다. 또 다른 연구에서 Poonacha 등[11]은 3 - 13세에서 교합평면 위치에서의 자입이 하치조신경 전달마취의 높은 성공률을 가져온다고 하였으나 Afsar 등[21]은 연령이나 성별에 따른 차이가 없다고 하여 연구마다 그 결과가 상이하게 보고된다.
과거 많은 연구들에서 성장기 환자의 마취 자입점 설정의 근거로 교합평면에 대한 하악공의 위치가 주로 평가되었으나[6,10,11,19,20,22-24], 하악소설의 위치에 대한 고려 또한 중요하다[1,13]. 하악소설에 부착하는 접형하악인대는 주사바늘로부터 하치조신경을 보호할 수 있는 구조임과 동시에 주사침이 하악소설의 내측 또는 정점 하방에 접촉했을 때에는 국소마취액이 하치조신경으로 확산되는 것을 방해할 가능성이 있다[25]. 따라서 하악소설의 약간 상방의 골에 자입점을 두어 하치조신경이 하악공으로 들어가기 전에 마취액이 확산되게 하는 것이 권장된다[1,12,26]. 성인에서는 그 위치로 교합평면 상방 1 cm를 목표로 하고 있으며, 하치조신경 전달마취 후 완전한 마취 효과를 보지 못하여 추가로 마취 시행 시 이전 자입 위치보다 상방으로 자입하도록 한다[12]. 또한 주 신경가지에 보다 확실하게 근접 될 수 있도록 과두돌기 경부 내측에 자입하는 Gow-gates 하악 전달마취법이 사용되기도 한다[27]. 소아에서도 Gow-gates 전달마취가 시행될 수 있으나 마취 발현까지의 시간이 길고 필요 이상의 영역까지 마취의 범위가 확대될 수 있다는 단점이 있기 때문에[27,28], 하악소설 또는 그 상방의 높이에서 정확한 자입을 통해 마취의 성공률을 높이는 것이 더욱 효율적이다[1,13].
이 연구에서 하악소설의 수직적 위치는 7 - 10세 어린이를 대상으로 연구한 Kanno 등[1]의 연구와 유사하게 연령에 따라 유의미하게 증가하여, 6 - 7세 1.47 mm, 10 - 11세 4.13 mm, 15 - 16세 8.78 mm로 나타났으며, 교합평면 상방에 위치하였다.
하악공은 교합평면에 대해 6 - 7세에 -3.85 mm, 10 - 11세에 -1.65 mm, 15 - 16세에 2.12 mm에 위치하였으며, 주로 후기 혼합치열기에 해당하는 10 - 11세 시기에 교합평면 하방에서 상방으로 이동하는 양상을 보였다. 이는 다른 연구들에서와 유사한 결과로 Hwang 등[24]은 9세, Hong 등[15]은 10 - 11세를 기준으로 하악공이 교합평면 하방에서 상방으로 이동한다고 하였다. 연구 대상과 방법에 따라 구체적인 수치는 차이를 보였으나 이외의 많은 연구에서도 연령에 따라 하악공의 높이가 점차 높아진다고 보고되었다[11,21-23].
이 연구의 결과를 종합적으로 고려했을 때, 하치조신경 전달마취의 자입점을 초기 혼합치열기에 교합평면 상방 2 - 3 mm, 후기 혼합치열기에 5 - 6 mm, 영구치열기에 9 - 10 mm 높이로 설정하는 것이 마취의 성공률을 높일 수 있다. 제안된 높이는 교합평면에 대한 하악소설 위치의 평균보다 상방에 위치하면서, 하악소설의 90% 이상을 하방에 위치시키는 높이에 해당된다. 또한 각 연령에서 하악공의 100% 상방에 위치하며, 교합평면에 대한 하악공과 하악소설의 위치가 연령에 따라 각각 약 3 - 4 mm씩 증가하는 것이 반영된 결과이다. 물론 마취는 단일 지점이 아닌 영역에서 이루어지며 동일한 연령에서도 해부학적 위치의 다양성이 크기 때문에 제시된 값을 일반화하기는 한계가 있겠지만, 소아 청소년의 마취 시에 임상적으로 적용할 만한 결과로 생각된다.
하악소설의 형태에는 다양성이 있다. Tuli 등[10]은 건조된 성인 하악골을 분석하여 처음으로 하악소설의 다양한 형태를 삼각형, 절단형, 결절형, 동화형으로 분류하여 설명했고 삼각형이 68%로 가장 흔하다고 보고했다. 접형하악인대의 부착이 하악소설의 모양에 영향을 줄 수 있으며, 하악소설을 포함하는 하악골의 외과적 수술 과정 동안 중요한 구조물을 보존하기 위해 하악 소설의 형태를 파악하는 것은 의미가 있다고 하였다[14]. 이 연구에서는 삼각형 형태가 가장 높은 비율을 차지하였고 동화형이 가장 낮은 비율을 보여 이전의 연구들과 동일하게 나타났으며[10,14,29-35], 연령 및 성별에 따른 차이는 나타나지 않았다.
하악소설의 형태에 따른 하악골 내에서 하악소설의 위치에 대해 브라질 성인을 대상으로 평가한 이전 연구에서 하악소설의 형태와 위치는 연관성이 있으며, 삼각형이 결절형보다 약간 더 후방에 위치한다고 보고했다[7]. 또 다른 연구에서는 삼각형 형태가 다른 형태들 보다 더 상방에서 관찰되는 결과를 보였고 하악지를 포함한 수술 시에 이러한 경향성에 대한 고려를 강조하였다[36]. 이 연구에서는 다른 형태들에 비해 삼각형 형태가 15 - 16세 연령에서 후방, 10 - 11세 연령에서 상방에 관찰된 결과를 보였으나 나머지 연령에서는 유의미한 차이를 보이지 않았고, 제한된 수로 일관된 경향성을 평가하기에는 한계가 있었다. 다만 지금까지 한국인 소아 청소년을 대상으로 하악소설의 형태에 대해 연구한 결과는 드물기 때문에, 이 연구에서 그 분포에 대해 평가하고 이전의 연구들과 비교하는 것으로 제한적인 의미가 있다. 하악소설의 인대 부착과 형태와의 관계, 하악소설의 형태와 위치와의 관계에 대해서는 추가적인 연구가 필요할 것으로 생각된다.
소아치과 의사는 다양한 연령층의 어린이와 청소년을 만나게 되며 이들은 성장 중에 있다. 이 연구 결과에서 나타나듯이 성장 중인 어린이는 고려해야 할 해부학적 다양성이 많으므로 세심한 주의를 기울여야 하며 치료 전에 정확한 영상 판독이 중요하다. 이 연구에서는 CBCT를 이용하여 하악골을 3차원적으로 분석하였다. 이는 2차원 방사선 촬영 영상에서 보일 수 있는 상의 확대, 왜곡, 구조물의 중첩, 허상의 문제나[37,38] 건조된 두개골에서의 수축, 미세한 골절의 문제없이[39] 높은 해상도로 정량적인 해부학 정보를 얻을 수 있는 이점이 있다[8,9,39].
이 연구의 한계점은 단일 조사자에 의해 측정되었다는 점이다. 다수의 평가자가 CBCT 영상을 판독하고 측정값이 일치된다면 연구의 신뢰성이 더 높아질 것이다. 또한 하악지와 시상면이 이루는 각도, 주사침의 자입 각도와 같은 다른 변수들도 함께 고려한 연구가 추가적으로 필요할 것이다. 한편, 개인의 해부학적 다양성은 측정값에 오차를 증가시킬 수 있기 때문에 향후 연구에서는 더 많은 수를 대상으로 한 연구가 필요하며, 동일한 환자에서 성장에 따른 변화를 측정하는 전향적 연구를 통해 신뢰성 높은 계측이 필요할 것이라 생각된다.
Ⅴ. 결 론
전남대학교 치과병원에 내원하여 CBCT를 촬영한 만 6 - 16세 180명의 환자를 대상으로 6 - 7세, 10 - 11세, 15 - 16세의 3군으로 나누어 연령에 따른 하악공과 하악소설의 위치변화를 평가하고, 하악소설의 형태에 대하여 후향적으로 분석하였다.
연구 결과 하악소설의 전후방 및 수직적 거리는 연령이 증가함에 따라 모든 방향으로 증가하였으며, 하악지 전연으로부터 하악소설의 거리는 연령에 따라 각각 약 17 mm, 18 mm, 19 mm로 측정되었다. 모든 연령에서 하악소설은 하악지의 전방 경계로부터 57 - 59% 지점에 위치해 있어 수평적으로 하악골의 중심보다 후방에 위치하였으며, 상방 경계로부터 32 - 33% 지점에 위치해 있어 수직적으로 하악골의 중심보다 상방에 위치하였다.
교합평면에 대한 하악소설의 높이는 연령이 증가함에 따라 각각 1.47 mm, 4.13 mm, 8.78 mm높이로 나타났으며, 하악공의 높이는 -3.85 mm, -1.65 mm, 2.12 mm로 증가하는 양상을 보였다.
이를 바탕으로 하치조신경 전달마취 시의 자입점은 하악지의 전연에서 수평적으로 약 60% 지점을 목표로 하되, 초기 혼합치 열기, 후기 혼합치열기, 영구치열기에서 각각 17 mm, 18 mm, 19 mm로 증가된 위치가 권장된다. 수직적으로는 연령이 증가함에 따라 교합평면 상방 2 - 3 mm, 5 - 6 mm, 9 - 10 mm로 자입점을 높이는 것이 마취의 성공률을 높일 수 있다.
하악소설의 형태는 모든 연령에서 삼각형 형태가 가장 많았으며, 연령에 따른 형태의 차이는 보이지 않았다.
이상의 연구를 통하여 소아 청소년의 하악공 및 하악소설의 해부학적 구조에 대한 정보를 제공하고, 하악 수술 및 하치조신경 전달마취 시에 도움이 될 수 있는 자료를 제시하고자 한다.