양산시 거주 청소년의 MIH 유병률과 임상적 특성
Prevalence and Clinical Features of Molar-Incisor Hypomineralization in Adolescents in Yangsan
Article information
Abstract
본 연구는 영구치열이 완성된 청소년을 대상으로, MIH를 포함한 영구치 법랑질 저광화의 유병률과 분포를 조사하고, 심미적 만족도와의 연관성을 파악할 목적으로 시도되었다.
양산시 거주 14 - 16세 청소년 1371명을 대상으로 횡단연구가 수행되었다. MIH를 포함한 법랑질 저광화는 유럽소아치과학회 기준에 의거하여 평가하였다. 전치부 심미성에 대한 설문 조사를 병행하여 전치부 법랑질 저광화의 연관성을 분석하였다
MIH에 이환된 경우는 189명으로 13.8%의 유병률을 보였다. 모든 영구치 중 1개 이상에서 저광화 병소가 나타난 경우는 318명(23.2%)으로 일반적인 MIH 기준 적용시에 비해 매우 높게 나타났다. 영구치에 나타난 법랑질 저광화 이환 빈도는 하악 제1대구치, 상악 중절치, 하악 제2대구치 순이였다. 전치부에 대한 평가에서는 상악 중절치의 절단연이 가장 높은 이환 빈도를 보였다. 전치부에서 저광화 병소가 존재하는 경우 높은 심미치료 요구도가 관찰되었다.
Trans Abstract
This study aimed to investigate the prevalence and distribution of enamel hypomineralization, including molar-incisor hypomineralization (MIH), among adolescents and assess their correlation with esthetic satisfaction.
A total of 1371 adolescents between the ages of 14 and 16 years in Yangsan city were evaluated for enamel hypomineralization, including MIH, according to the European Academy of Paediatric Dentistry (EAPD) criteria. In a parallel survey, esthetic satisfaction about anterior teeth and its correlation with incisor enamel hypomineralization were analyzed.
The prevalence of MIH was 13.8% (n = 189), while that of hypomineralization in any permanent tooth was 23.2% (n = 318), which was substantially greater compared to the national prevalence of MIH. Mandibular first molars exhibited the highest prevalence of hypomineralization, followed by maxillary central incisors and mandibular second molars. Among anterior teeth, the most frequently affected site was the incisal edge of maxillary central incisors. A high degree of hypomineralization in anterior teeth was associated with a high demand for esthetic treatment.
I. Introduction
With recent improvements in the level of oral care, the prevalence of dental caries, a prominent oral disease, has been decreasing [1,2]. In contrast, the prevalence of enamel hypomineralization due to systemic factors has increased, which has heightened interest regarding this condition [3,4].
Crown formation in first permanent molars and incisors occurs at approximately the same time [5], during which enamel hypomineralization is frequently observed. Enamel hypomineralization in first permanent molars and anterior teeth was first reported in 1970 in Sweden [6]. In 2001, Weekheiim et al. [7] defined MIH as demarcated, qualitative enamel defects of systemic origin, affecting one or more permanent molars with or without involvement of incisor teeth. Since then, several studies worldwide have actively investigated the etiology, conditions, and prevalence of MIH, with most focusing on first permanent molars and incisors.
However, the clinical categorization of hypomineralization is broad, and clinically, all primary teeth, permanent canines, premolars, and second permanent molars can be affected by enamel hypomineralization [8-10]. Therefore, in a recent policy, the European Academy of Paediatric Dentistry (EAPD) recommended that whole dentition be included in future studies on enamel hypomineralization [11].
Several studies have investigated the causes of MIH [12]. A recent study reported that, while a significant correlation existed between MIH and polyvinyl chloride/dioxin discharge, MIH was only weakly correlated with nutritional status, birth conditions, childhood diseases, and fluoride intake [13]. In another study, water fluoridation and pregnancy at an older age were identified as risk factors for MIH [14,15]. High vitamin D concentration in blood has also been reported to be negatively correlated with MIH. While it appears that MIH is caused by various risk factors, no definite risk factors have been identified yet [16].
Teeth affected by MIH exhibit enamel defects and rapid progression of caries; therefore, in many cases, affected teeth require restorative treatment right after eruption. However, owing to the high organic content of enamel, the success rate of adhesion of restorations is low [17,18]. If the defect is deep and widespread, it can lead to severe loss of tooth material and early loss of permanent teeth because of caries progression. In addition, in adolescents with active social lives and a developing interest in appearance [19], slight defects can have a serious impact on self-esteem, depending on the location of the defect.
Despite the significant impact of MIH on adolescents, previous studies have only investigated MIH among elementary school students [20], and no study till date has evaluated MIH among a teenage population. The subjects of the present study were middle-school students with complete eruption of permanent dentition. The prevalence, defect patterns, and distribution of permanent tooth enamel hypomineralization, including MIH, and their effects on tooth condition and esthetic satisfaction were evaluated.
II. Materials and Methods
1. Subjects
An inspector performed oral examination of 1371 adolescent students between the ages of 14 and 16 years at a middle school in Yangsan province, South Korea, between May and August 2013. Water fluoridation had not been enforced in this area, and the fluoride concentration in water was lower than the detection limit of 0.15 ppm. To eliminate potential confounders, subjects with primary teeth remaining or preemergent second permanent molars were excluded from the study. Subject age and sex distribution are presented in Table 1.
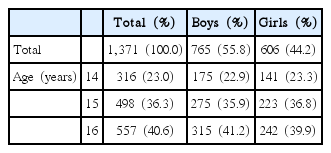
Distribution of sex and age of the subjects
2. Research Methods
1) Preliminary investigation and ethical considerations
Prior to the survey, the inspector underwent training with clinical images and patients who visited the Pediatric Dentistry department at Pusan Dental Hospital, in order to establish consistency in diagnosis. With the help of an expert, the inspector was administered a blind test using 50 images of teeth with MIH, enamel hypoplasia, or fluorosis, with the accuracy set initially at 96.0%. The same images were retested a month later, and the findings of the first and second tests exhibited a very good agreement, with a Kappa value of 0.87.
This study was approved through review by the Bioethics Committee of Pusan University Dental Hospital (PNUDH-2013-017).
2) Oral examination
Oral examination was performed using a head light, dental mirror, and community periodontal index probe, with the examinee seated in a chair in the health service room of the school. Subjects were instructed to brush their teeth prior to examination, and, when necessary, a gauze was used to remove food debris and dental plaques.
(1) Enamel hypomineralization
Hypomineralization in the dentition-from the central incisor to the second permanent molar-was evaluated. Enamel hypomineralization was considered present when an impervious enamel defect with a clearly visible white or brown-colored boundary was observed while the tooth was wet. However, cases in which the lesion was less than 1 mm diameter, cases of trauma and cases of periapical inflammation in primary teeth were excluded [21]. Teeth diagnosed with enamel hypomineralization were classified according to the criteria proposed by the EAPD in 2003 (Table 2) [22]. Further, the labial surfaces of incisors, lateral incisors, and canines were divided into nine compartments, and the presence and distribution of enamel defects in each compartment were also recorded for evaluation of esthetics. Subjects were assigned to one of three groups: the normal (no defects), EH (permanent dentition with defects in at least one tooth), or MIH (defects in first permanent molars) groups.

EAPD criteria for molar incisor hypomineralization
3) Questionnaire survey
A questionnaire survey was conducted to determine the correlation between state of enamel hypomineralization and esthetic satisfaction about anterior teeth. The questionnaires were distributed at the examination site, and subjects completed them under the guidance of teachers.
4) Data analysis
The collected data were analyzed using SPSS 13.0 (SPSS Inc., USA) for Windows. The level of significance was set at 0.05 for all statistical data. The significance of sex and age with regard to prevalence was verified by the chi-square test. Incidence of tooth-specific defects was determined by frequency analysis. The correlation between first permanent molars and the rest of the permanent teeth in affected individuals was determined by correlation analysis.
III. Results
1. Prevalence of enamel hypomineralization
The distribution of prevalence of enamel hypomineralization among the subject pool is presented in Table 3. Of the total 1371 subjects, 318 (23.2%) were assigned to the EH group and 189 (13.8%) to the MIH group. In both groups, the prevalence of enamel hypomineralization among female subjects was greater compared to that among men, although the difference was insignificant (p > 0.05); however, there were significant differences in prevalence of enamel hypomineralization according to age (p < 0.05).

Prevalence of enamel hypomineralization
The average numbers of affected teeth in the EH and MIH groups were 3.82 (boys, 3.88; girls, 3.76) and 5.18 (boys, 5.22; girls, 5.13), respectively, with no significant differences according to sex (p > 0.05; Table 4).
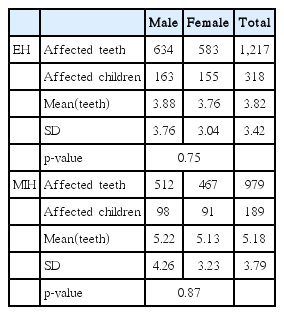
Number of teeth affected by enamel hypomineralization and molar incisor hypomineralization
2. Distribution of defects according to tooth type
Among all teeth that exhibited enamel hypomineralization, mandibular first permanent molars were the most commonly affected, followed by maxillary central incisors, maxillary first permanent molars, and mandibular second permanent molars, in that order (Table 5).

Distribution of affected teeth by tooth type
Analysis of correlation between first permanent molars and the rest of the permanent teeth with regard to enamel hypomineralization defects revealed that presence of defects in first permanent molars indicated the possibility of defects in the rest of the permanent teeth. This correlation was the highest among central incisors, followed by second permanent molars (p < 0.05; Table 6).

The correlation between first permanent molars and the rest of permanent teeth in regards to enamel hypomineralization defects
3. Condition of affected teeth
Incisors and first and second permanent molars exhibited high morbidity rates; Table 7 presents the results of analysis of lesion patterns in these teeth according to the EAPD criteria. In incisors, demarcated opacity was the most prevalent type of defect at 99.7%, while the prevalence of enamel breakdown was only 0.3%. In first permanent molars, demarcated opacity was the most prevalent defect pattern at 49.6%, followed by atypical restoration at 46.1%, and even extraction at 1.8%. Similarly, in second permanent molars, demarcated opacity was the most prevalent defect pattern at 85.8%, followed by atypical restoration at 13.0%. The differences in defect patterns according to tooth type were significant (p < 0.05).

Status of affected incisors and molars
4. Range of defects and need for treatment of labial surfaces of incisors and canines
Fig. 1 presents the range and distribution of defects among the nine compartments on the labial surfaces of central and lateral incisors and canines. Defects were deemed present when they met at least one of the four criteria shown in Table 2. Based on the number of teeth with lesions in each compartment, six grades of defects were defined, ranging from < 10 to > 50, represented by a change in color. When teeth were divided into three equal parts from top to bottom, the most frequently affected regions were the edge and middle portion of maxillary central incisors, in that order.
Surface-related distribution in anterior teeth.
Subsequently, depending on the number of affected teeth, a total of 12 teeth and 108 blocks were classified into 6 subject groups for evaluation of esthetic satisfaction and need for treatment, as indicated by subject response to the questionnaire survey. Subjective esthetic satisfaction was evaluated on a scale of 1 to 5. Esthetic satisfaction scores for presence of enamel hypomineralization in incisors or canines were lower (p < 0.05; Table 8). The need for esthetic treatment, although not in proportion with the increase in number of affected blocks, varied significantly depending on the presence or absence of defects (p < 0.05; Table 9).
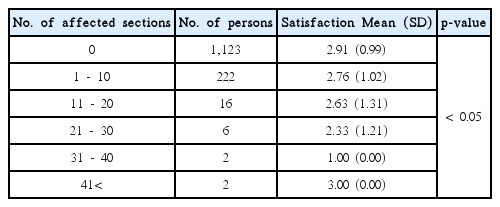
The correlation between range of defects and esthetic satisfaction

The correlation between range of defect and need for treatment
IV. Discussion
Enamel breakdown can occur on occlusal force impact, and enamel hypomineralization appears in a variety of colors, including yellow, tan, brown, and milky white [23]. The aprismatic enamel layer, thick prism sheath, and coarse crystals observed in hypomineralized enamel are responsible for the decreased hardness of hypomineralized teeth [24]. In particular, when bacteria penetrate porous enamel, the pulp enters into a state of chronic inflammation, which causes hypersensitivity and failure of local anesthesia [24,25]. Because of the resultant constant pain, young and adolescent patients affected by MIH often exhibit behavior management issues during dental treatment.
In addition, enamel hypomineralization typically occurs at locations other than those of dental caries, and when lesions affect the cusp, appropriate restoration becomes very difficult [26]. Consequently, maintaining restorations is challenging, and several claims are being raised that it is best to extract teeth with poor prognosis in a timely manner [27]. Traditionally, the ideal age for extraction of first permanent molars is 9 - 11 years [28]. However, recent studies are conflicted over the appropriate age for extraction; some studies have proposed that extraction should be performed at a younger age, whereas others have stated that early extraction could increase the risk of hypomineralization in second permanent molars [29].
Anterior teeth defects are treated with emphasis on esthetic improvement. However, because microabrasion, resin restoration, and whitening agents such as hydrogen peroxide usually cause mineral loss [30], casein phosphopeptide-amorphous calcium phosphate is now being used for active remineralization treatment [31].
In general, the ideal age for MIH epidemiological studies is 7 - 8 years, during which the first four permanent molars will have erupted and enamel loss due to dental caries or other diseases would not have started yet. In addition, at this age, children still possess a residual part of the second molar, which makes it possible to evaluate the correlation between MIH and second-molar hypomineralization. Elfrink et al. recently suggested that primary molar hypomineralization and MIH are correlated and that the former could be a predictor of MIH [32]. In the present study, although the entire permanent dentition was evaluated, hypomineralization of second permanent molars was the focus of evaluation. Therefore, subjects with complete dentition, between the ages of 14 and 16 years, were enrolled as study subjects.
The most active research on prevalence of MIH is conducted in Europe, where prevalence levels ranging from 3.6% to 37% have been reported [10]. In Asian countries, prevalence of MIH has been reported to be 2.8% in Hong Kong [33], 25.5% in China [34], 20% in Thailand [35], and 6.0% in South Korea [20]. This variation in prevalence might be attributable to environmental or genetic factors or even differences in research methodology and criteria among various studies [10]. In the present study, the prevalence of MIH was 13.8%, which increased to 23.2% upon expanding the study sample to include subjects in the stage prior to permanent dentition. This value is slightly higher compared to that reported in a nationwide survey in 2010, probably because the previous study included children in Pusan and larger cities as test subjects, while the present study only included subjects from a provincial area in Yangsan. Because the residents of this province have lower socio-economic status and limited access to health services in comparison with residents of bigger cities, the risks of development and progression of oral diseases among the former are known to be high. Epidemiological studies on MIH have also reported that children living in provincial areas exhibit higher prevalence of MIH than those living in cities [36].
In the present study, the average number of teeth with lesions in the EH and MH groups were 3.88 and 5.18, respectively, with no significant differences according to sex. These values were higher compared to those reported in 6 to 12-year-old children in Brazil at 3.3 [37], 12-year-old children in Hong Kong at 2.6 [33], and 8-year-old children in Spain at 3.5 [38].
In the EH group, mandibular first permanent molars were the most commonly affected teeth, followed by maxillary central incisors, maxillary first permanent molars, and mandibular second permanent molars, in that order. These results indicating high prevalence of MIH in first permanent molars and maxillary central incisors are consistent with those of previous studies [36]. It is noteworthy that the proportion of affected second permanent molars, which are generally excluded from MIH diagnosis, was relatively high. It is, therefore, necessary to study hypomineralization in second permanent molars, which experience a relatively high proportion of occlusal forces. In the MIH group, where subjects exhibited defects in first permanent molars, the results of correlation analysis demonstrated that presence of defects in first permanent molars indicated a high possibility of presence of defects in the remaining permanent teeth, with the correlation being especially strong among central incisors and second permanent molars. Given the strong correlation between MIH in first and second permanent molars, extraction of MIH-affected first permanent molars-which is one of the treatment choices-should be planned carefully.
In the present study, the pattern of MIH defects varied according to tooth type. Demarcated opacity was the most commonly observed defect at 99.7% in anterior teeth, probably because the positional characteristics of anterior teeth renders them unaffected by bite forces and also decreases their chances of developing crown fractures from external factors. First permanent molars exhibited similar proportions of demarcated opacity at 49.6% and atypical restoration at 46.1%, which indicated a history of hemorrhoid damage. The highest prevalence of demarcated opacity was observed in second permanent molars at 85.8%. Since the present subjects had just experienced eruption of second permanent molars, we believe that they might not have yet suffered enamel loss due to occlusal forces or dental caries. In the absence of appropriate regulated treatment for demarcated opacity, there is a very high chance that the condition could progress into first permanent molars and atypical restorations.
Subjects with enamel hypomineralization in anterior teeth frequently experienced esthetic dissatisfaction. In this study, among the six anterior teeth, high prevalence of enamel hypomineralization was observed in in the middle and 1/3 of the incisal edge of maxillary central incisors. Hypomineralization in these teeth becomes evident during smiling, talking, and mastication, which might adversely affect esthetic perception. The present results of the questionnaire survey for subjective esthetic satisfaction revealed lower esthetic satisfaction and greater need for esthetic treatment in presence of defects in anterior teeth, which also reflected the effect of MIH on esthetic satisfaction among patients. Adolescence is a period of transition from childhood to adulthood, which involves physical and psychological changes. Therefore, it is necessary to consider the possibility of loss of self-esteem due to physical defects among adolescents.
V. Conclusion
The present study aimed to investigate the prevalence and distribution of enamel hypomineralization among adolescents. The results indicated a 13.8% prevalence of MIH, which increased to 23.2% upon inclusion of permanent teeth. Enamel hypomineralization in first permanent molars was significantly correlated with that in central incisors and second permanent molars. In anterior teeth, the middle and 1/3 of the incisal edge of maxillary central incisors were the most affected by hypomineralization. Patients with defects in anterior teeth exhibited low esthetic satisfaction and high demand for esthetic treatment.