


Ⅰ. Introduction
In 1962, Jacqueline Noonan, a pediatric cardiologist, reported 9 children who had distinctive facial features, short stature, chest deformities, and congenital heart disease. Since she showed that this disease affects both females and males, Noonan syndrome (NS) was named after Dr. Noonan. NS is a common congenital genetic disorder with an estimated incidence of between 1 per 1,000 and 1 per 2,500 live births. This disease undergoes autosomal dominant hereditary transmission, but the phenotype expression varies[1]. Other characteristics of NS include hearing impairment, visual disturbance, bleeding tendencies, malignant hyperthermia by certain general anesthetics (which is rare), and delayed motor development and speech. Oral and dental issues of NS include a high arched palate, dental malocclusion, ectopically positioned teeth, micrognathia, articulation difficulties, delayed tooth eruption, dental erosion, and multiple dental caries[1-4].
There is the American Academy of Pediatrics guideline for NS. While this guideline is mainly focused on the medical area, the information of the dental area is insufficient. Only limited descriptions of the oral features and management are available. NS is a common congenital genetic disorder with relatively high incidence and causes multiple problems such as heart disease, renal disease, and hemostasis issue. Therefore, dentists should be aware of the NS on clinical features, oral characteristics, and considerations for treatment. Thus, this case report describes the oral features and management of NS.
Ⅱ. Case Report
An 11-year-old boy with NS visited the hospital with an ectopically positioned maxillary right canine.
The information was obtained from medical records. The patient had a cardiac murmur at birth and was diagnosed as congenital pulmonary valve stenosis (PVS) without cyanosis.
Genetic testing was conducted in 2014, which revealed a mutation in p.Met504Val on PTPN11 exon 13. PTPN11 is expressed in most tissues and controls various cell signaling pathways that are important for numerous cell functions, such as mitogenic activation, metabolic control, transcriptional regulation, and cell migration[5]. Mutations in PTPN11 typically interrupt the binding interface between the N-SH2 domain and catalytic core required for the enzyme to maintain its auto-inhibitory conformation. Therefore, these mutations result in gain-of-function changes and the pathogenesis of Noonan syndrome arises from excessive SHP-2 activity[6]. The phenotypes of NS with PTPN11 mutations have been associated with a pectus deformity, the characteristic facial appearance, short stature, pulmonary valve stenosis, and atrial septal defects[1]. Mutations in PTPN11 are also associated with genetic diseases and cancer, such as Leopard syndrome, juvenile myelomonocytic leukemias, neuroblastoma, melanoma, acute myeloid leukemia, breast cancer, and lung cancer[7,8].
In addition, growth and development was delayed, so the patient was treated with growth hormone. He also had a hearing impairment and wore a hearing aid. In many cases, there are issues with hemostasis, which our patient did not experience.
His height was 140 cm at the 1st visit, which was below the 50th percentile of the standard growth curve of Korean children and adolescents. His weight was 32.4 kg, which was around the 25th percentile of the standard growth curve of Korean children and adolescents.
His facial appearance showed characteristic features of NS (Fig. 1). The forehead was broad and arch-shaped, the eyelids were drooping, the nose was broad with a depressed root, the ears were low-set, posteriorly rotated, and had an oval shape, and the neck was the webbed with a wide shape. Another feature included his hoarse voice.
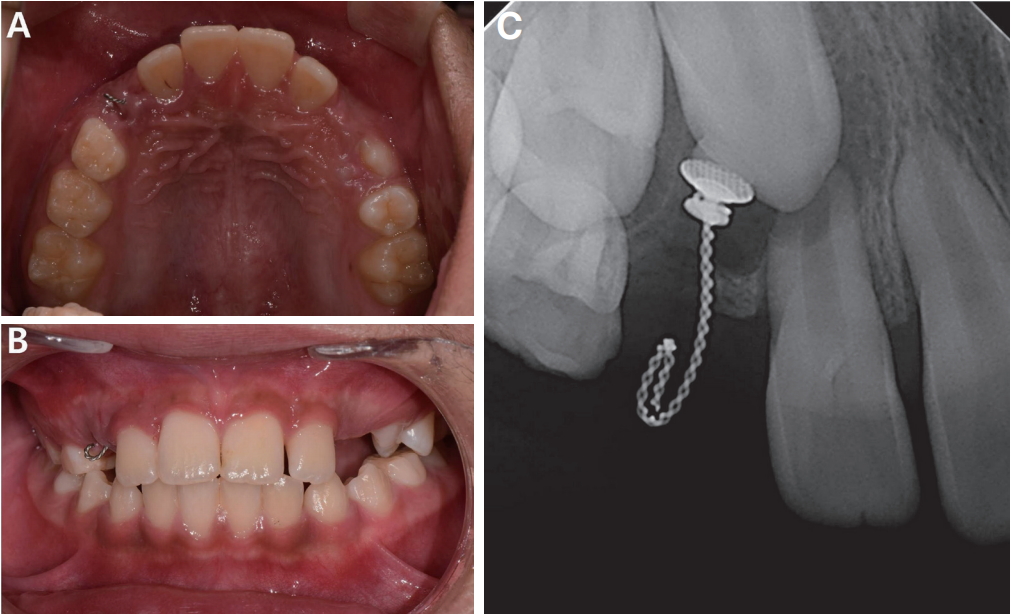
Based on intraoral examination, the patient showed a dental class II relationship, protrusion of the upper anterior teeth, and a shallow overbite. The left lateral incisors showed an edge to edge bite, but his palatal arch shape was normal (Fig. 2).
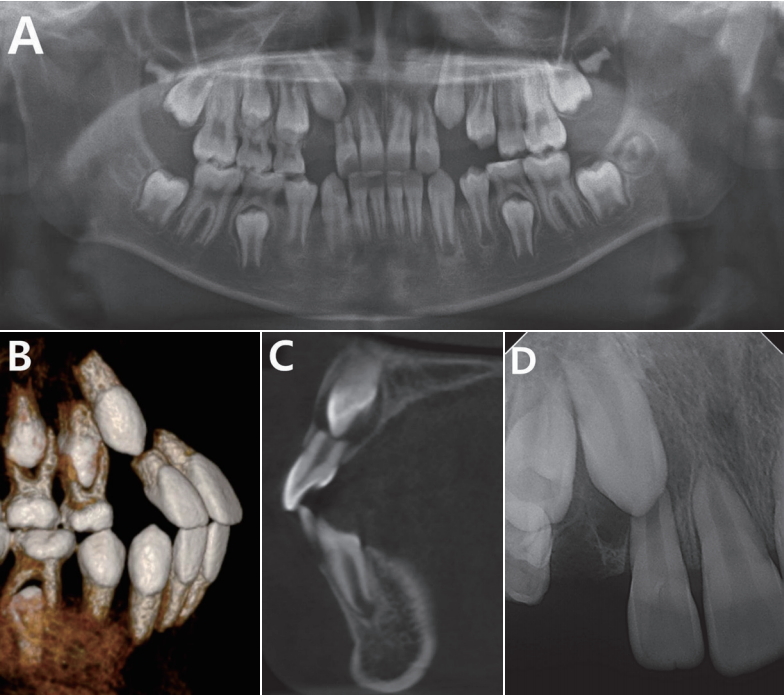
Radiographic examination revealed that the upper right canine was ectopically positioned, which led to root resorption of the upper right lateral incisor (Fig. 3). A lateral cephalometric film showed a craniofacial pattern that was within normal limits. Dental patterns of maxilla and mandibular teeth were protrusive and the soft tissue profile was convex (Fig. 4).
Surgical opening and round button (Lingual button 001-05, Tomy Incorporated, Japan) with wire attachment on the impacted upper right canine was performed and traction was applied. Before surgery, prophylactic antibiotics were prescribed. A wire for tooth traction was exposed to gingiva (Fig. 5).
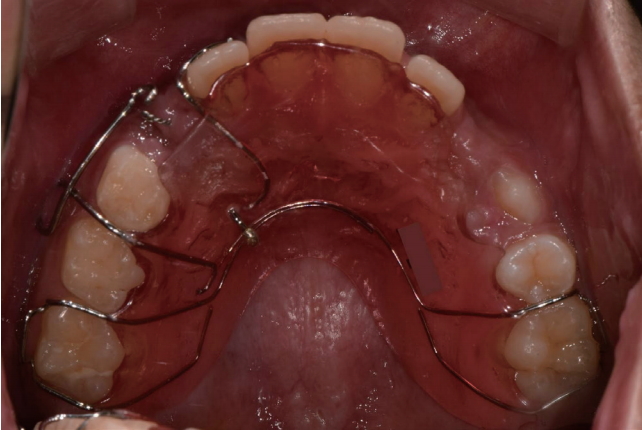
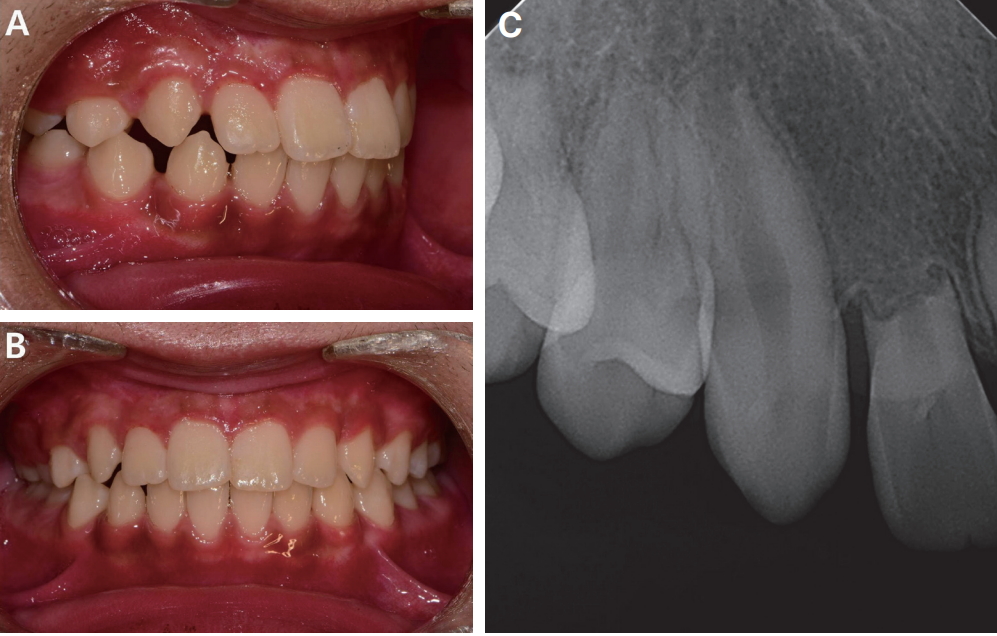
Traction of the ectopic positioned tooth was applied using a removable appliance (Fig. 6) and elastic rings. For patient compliance, it started to hang the elastic ring after 1 week since the appliance was delivered. For the 1st month, 3/16 “ 3.5 oz. elastic rings (Energy PakTM elastics, RMO, USA) were used and after that 1/8 “ 3.5 oz. elastic rings were used. The patient showed poor compliance with treatment, such as not wearing the removable device properly or having issues with hanging the elastic ring. Following a removable appliance was used for 10 months, brackets were attached to the upper right central incisor, lateral incisor, primary 1st molar. Power chains were used to pull the impacted tooth labial direction. During the traction, the upper right lateral incisor root resorption was increased. The treatment period was longer than that of other children until the impacted canine erupted (Fig. 7). Although the patient showed low treatment compliance, low comprehension, and was lacking in patience, his behavior was controlled by verbal management during treatment.
Ⅲ. Discussion
It is difficult to accurately diagnose NS since it has characteristics similar to other diseases. Turner syndrome, cardiofaciocutaneous (CFC) syndrome, and Costello syndrome resemble the NS phenotype. Thus, genetic testing is useful for a differential diagnosis. In 2001, it was shown that NS could be caused by missense mutations in the protein tyrosine phosphatase nonreceptor type 11 gene (PTPN11 )[1]. This represents a protein tyrosine phosphatase that plays a role in the RAS-mitogen activated protein kinase (MAPK) signal transduction pathway; thus, NS is a disorder of the RAS-MAPK pathway[9]. NS could also be identified based on mutations in genes including RAS, SOS1, RAF1, BRAF, SHOC2 , and NRAS [1]. Although it remains unclear, the RAS-MAPK pathway is believed to regulate bone homeostasis and a mutation in PTPN11 could affect osteoblast and osteoclast activity. Children with NS showed a significantly lower total bone mineral content and bone mineral density compared to same age, gender, and height children without NS[9]. Bone resorption is increased in NS associated with increased Ras/MAPK pathway[10]. The bone remodeling can affected the rate of tooth movement; in other words, tooth movement is reduced when the bone remodeling is low[11]. The velocity of impacted tooth movement in this patient with NS during the traction was slower than normal children, suggesting that it may be influenced by subtle variations in bone remodeling as a result of mutations in PTPN11 . This patient also showed poor compliance with treatment, such as not wearing the removable device properly or having issues with hanging the elastic ring. Furthermore, these factors influenced the length of the treatment period and the slow tooth movement rate.
Although the majority of individuals with NS have a short stature, some individuals with NS show normal growth and stature. Birth weight and length are normal, but their growth patterns decrease to the 3rd percentile or less[1]. In this case, the patient did not show a significant growth delay. This may be an effect of growth hormone treatment, but it is important to observe the final growth and development.
His facial appearance showed typical features of NS, which are generally most distinct in infancy. With age, these features become more subtle[1]. Thus, early diagnosis of NS by a pediatrician is important.
Oral features of NS include a high arched palate, dental malocclusion, ectopically positioned teeth, micrognathia, articulation difficulties, delayed tooth eruption, dental erosion, and multiple dental caries[1-4].
The mandibular cysts occasionally occur in patients with NS, which is similar to cherubism[1,12]. In the present case, the patient showed mild dental malocclusion (dental class II relationship, shallow overbite). The upper right canine was ectopically positioned, which led to root resorption of the upper right lateral incisor. However, his palatal arch shape was normal and his skeletal pattern was observed within normal limits.
The American Academy of Pediatrics (AAP) proposed management recommendations of NS in 2010. For dental management, dental services should be contacted between the ages of 1 and 2 years. In addition, patients require regular follow-up once a year[1].
Few studies have reported the oral characteristics and detailed dental management of Noonan syndrome despite its high incidence. Thus, we recommend the management of, and precautions for, NS patients. There are no elements that cause major problems during common dental treatments. NS patients have diverse dental problems such as malocclusion and abnormal tooth eruption patterns[1-3]. Thus, it is important to have regular check-ups. Through regular check-ups, orthodontic treatment can be obtained over time. In many cases, subjects with NS showed feeding difficulties in infancy, and the parents provided the children with soft diets[1]. However, these eating habits cause dental caries. Thus, it is important to protect against dental caries by applying topical fluoride, sealant, and through regular oral examination.
Patients with NS often have congenital heart disease and renal disease. PVS is the most common cardiac condition in NS, which is often mild and requires only periodic reevaluation[1]. Dental treatment should proceed with caution in preventing infective endocarditis according to the 2007 American Heart Association (AHA) guideline[13]. Thus prior to treatments that can lead to infections, prophylactic antibiotics and a consult with a pediatrician may be required.
If the patient had uncooperative behaviors, conscious sedation or general anesthesia may be considered for treatment and management. The problems that may occur during general anesthesia are as follows. It is difficult to intubate due to high arched palate, short webbed neck, and micrognathia. There is limited cardiovascular reserve associated with cardiovascular disease especially pulmonary stenosis and atrial septal defect. It may be difficult to access intravenous veins due to redundant skin and lymphedema. In addition, congenital renal disease may cause electrolyte imbalance[14,15]. Thus, it needs to consult a pediatrician prior to treatments and dentists should pay attention to maintain airway during treatment under conscious sedation.
Hemostatic abnormalities have been reported in 30% to 65% of subjects with NS. Platelet dysfunction, thrombocytopenia, and deficiencies in coagulation factors have been reported. Although disordered bleeding is often mild, bleeding with surgical procedures can be severe[1,16]. If the patient has a hemostasis issue, they should consult a pediatrician or receive vitamin K, hemostatic agents such as tranexamic acid, or desmopressin[16]. The patient in this case did not have a bleeding disorder. Although included in the normal range, there was a tendency to delay bleeding during the window opening surgery. Thus, a blood test should be performed before starting treatment, and the treatment should be performed gently to prevent excessive bleeding. Dentists should make sure hemostasis before the patient was discharged.
Most patients with NS have normal intelligence. Among those of normal intelligence, the IQ has been shown to be 10 points less than unaffected family members or 1 SD below that of the general population. The majority of children with NS manifest poor cooperation, obstinacy, and irritability[1]. This patient also showed low treatment compliance, low comprehension, and was lacking in patience. Thus, the dentist should repeatedly explain and encourage children with NS.
There are limitations in discussing the oral features of NS patients from the analysis of only 1 patient. To define the oral characteristics of NS and propose a management protocol for NS during dental treatment, more patients should be examined.
Ⅳ. Summary
The patient in this case was not strongly affected by NS and showed mild dental problems. However, few reports have discussed the oral characteristics of NS despite its high incidence. Therefore, this report described the oral features of NS such as dental malocclusion, ectopically positioned teeth, dental erosion, and multiple dental caries. In addition, dental management of NS from the early infant period is recommended.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






