


Ⅰ. Introduction
Parenting styles were known to influence the well-being of children[1]. Three types of parenting styles, authoritative, authoritarian, and permissive, had been described by Baumrind[1]. Authoritative parents were controlling, but were also warm and receptive to the child. Authoritarian parents were less friendly and more controlling in their interactions with their child[1]. Permissive parents were non-controlling and nonresponsive toward their child and made few demands. The parenting style of caregiver could influence disease outcomes. The environment that they created for the child could change oral hygiene, dietary practices, and dental attendance patterns[2]. Since the parent was responsible for nearly all aspects of the child’s oral health, it could be assumed that the parenting style of the caregiver could influence early childhood caries (ECC)[2].
Evidence supported a potential relationship between parenting styles, child behavior, and dental caries[3], but limited research has been performed on this topic. The most relevant and closely related publication was by Kumar et al.[4], who showed a correlation between parenting practices and children’s dental caries experience. Children exhibited a higher dental caries experience when they were raised with more power assertion parenting practices[4]. Howenstein et al.[5] suggested that authoritative parenting styles were associated with few caries. This publication also indicated an association between authoritarian parenting practices and increased caries. On the other hand, Dabawala et al.[1] concluded that the association of parenting styles with ECC could not be confirmed. The conclusions about the relationship between parenting styles and dental caries had yet to be concluded and were mixed and controversial.
Biological and environmental factors related to early childhood caries have been well-established[6,7]. However, the relationship between parenting styles and ECC has not been clearly elucidated yet[7], and research on this topic has not been conducted in Korea. This study aimed to evaluate the association between parenting styles and childhood dental caries using a sample of Korean children 3 - 6 years of age.
Ⅱ. Materials and Methods
1. Subjects
A total of 353 children between 3 to 6 years of age from four kindergarten institutions in Korea were surveyed. Before samples were selected, Institutional Review Board (IRB) was received and informed consent from each subject was written (IRB approval number 2018-08-041). Among the kindergarteners, questionnaires were given in advance to the parents at each of the four institutions. The following situations resulted in subject exclusion from the sample size: if the PSDQ questionnaire was partially filled/unreturned, if the parents did not give informed consent for participation in the study, or if the child was absent on the day of the oral examination.
2. Methods
1) Parenting Styles Assessment Tool
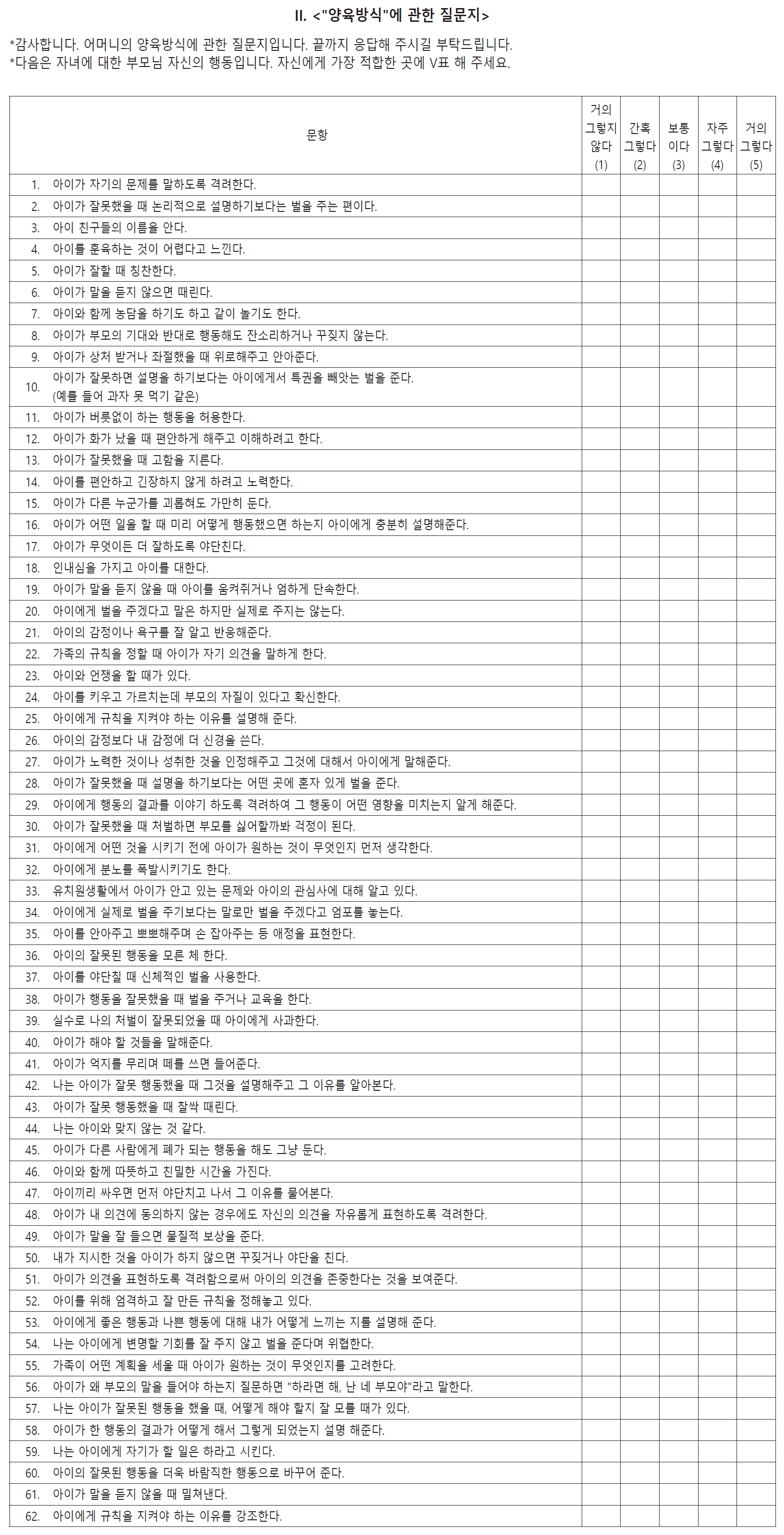
The PSDQ contained 62 statements regarding different parent reactions to child behavior[8]. Translated version which was used in a study conducted in the department of education in Korea[9] was used in this study (Fig. 1). The questionnaire assessed the parenting style based on Baumrind’s parenting types: authoritative, authoritarian, and permissive[5]. Each parent was asked to rank each statement on a Likert scale from 1 to 5 (1 equals never, 2 equals once in a while, 3 equals half the time, 4 equals very often, and 5 equals always) as to how regularly they and their spouse/significant other (if applicable) exhibited each behavior[5]. The scoring key of the PSDQ was used to classify the parents into one of the three specific parenting styles. Depending on the previous study[8], there were 27 items for the authoritative parenting style. The authoritarian style included 20 questions, while the permissive manner included 15 questions (Table 1). An overall mean score in each parenting style category was calculated, and this score determined the parent’s particular style with the highest mean score placing the parent in the proper parenting category[5].
2) Demographic factors
The questionnaire as a second part involved individual data including gender, parent’s educational level, and order of birth.
3) Oral examinations
A dentist performed oral examinations using dental mirrors and explorers with hand lights in the kindergarten classes. Before the oral examinations, the dentist was trained and calibrated on the WHO criteria of dental caries. Ten new patients who visited our hospital were examined at the time of initial visit and first visit for treatment without radiography. The intraclass correlation coefficient was 0.80 and demonstrated good to excellent correlation.
4) Analysis of data
The criteria for the diagnosis of dental caries was based on the requirements from the World Health Organization (WHO). The experience of dental caries was distinguished as dt (decayed primary tooth), ft (filled primary tooth), and mt (missing primary tooth). The dft index was the sum of decayed and filled primary teeth. As the primary tooth were not missing early physiologically, missing tooth especially posterior primary tooth contained to decayed or filled teeth under 5 years old.
To compare the dft index according to the parenting styles, the parenting styles were analyzed in two ways. The first method was to classify the parenting styles as previously described[5] and compare the dft index. The second method compared the dft index according to the subdomains of each parenting style. All subjects were summed and averaged the scores of the questionnaire items for each parenting style (Table 1). By this method, all subjects had three average values (authoritative domain, authoritarian domain, and permissive domain). Each parenting style subdomain was grouped into five groups according to the Likert scale. The higher the group number, the more the parent showed the characteristics of each parenting style. The dft index was compared between groups by each parenting domain.
5) Statistical Analysis
R language version 3.3.3 (R Foundation for Statistical Computing, Vienna, Austria) and T&F program ver. 1.0 (YooJin Bio-Soft, Korea) were used for all statistical analyses. Mean values of demographic characteristics were calculated and analyzed using Mann-Whitney analysis and Kruskal-Wallis test. Association between parenting styles and dft index were analyzed by Mann-Whitney analysis. Kruskal-Wallis test was conducted to compare the dft index according to each subdomain. Post-Hoc analysis was performed using Bonferroni algorithm.
Ⅲ. Results
The questionnaire was distributed to 353 children and their parents. A total of 158 questionnaires were returned (response rate of 44.7 percent), and these children underwent clinical examinations. Ninety boys made up 52.9 percent of the total subjects, while 80 girls made up 47.1 percent of the total number of subjects. Based on age, 23 children (3 years old) accounted for 14.6 percent of the study population, while 43 children (27.2 percent) were four years old. Fifty-four children (34.2 percent) were five years old, and 38 children (24.0 percent) were six years old (Table 2). Approximately, one half (55 percent) of the subjects had one or more decayed teeth with a mean dft index of 3.6.
The results of the survey on the demographic factors were as follows (Table 3). Differences according to gender were found in girls with an average dft index of 2.92 and boys with 2.84 with no statistically significant difference (p = 0.981). According to the parents’ educational level, the dft index decreased as the educational level increased, but was statistically insignificant (p = 0.502). In the dft index difference, according to the birth order, the dft index increased as the birth order increased (p = 0.020).
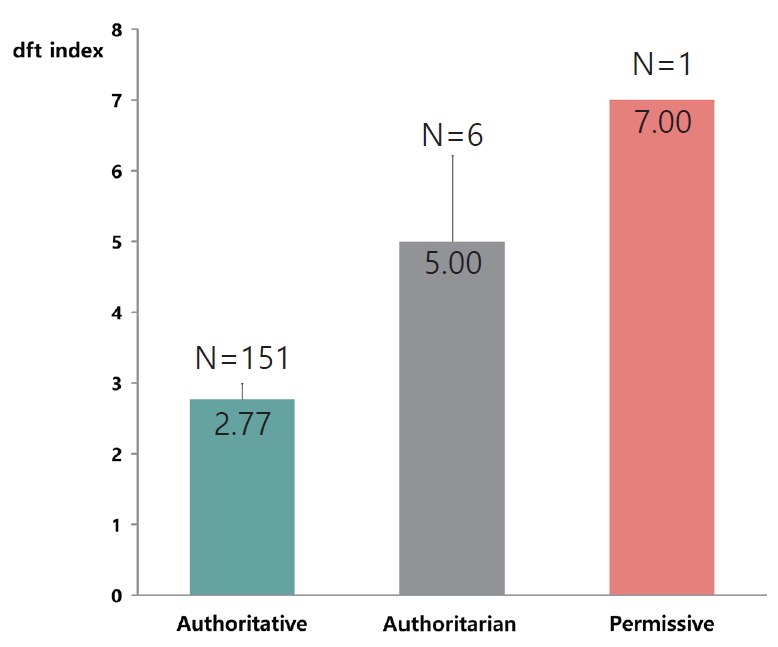
Among the 158 parents/child dyads who completed both questionnaires and oral examinations, the results of the PSDQ were as follows: 151 parents (95.6 percent) exhibited authoritative parenting, 6 (3.8 percent) exhibited authoritarian parenting, and only 1 (0.6 percent) exhibited permissive parenting. The authoritative parenting style was dominant. The difference between the dft index, according to the three groups, was shown in Fig. 2, and the p value was not statistically significant at 0.068. The mean dft index in the authoritative group was 2.77 and the lowest dft index among all the groups. In the authoritarian group, the dft index was 5.00, the second highest. In the permissive group, the dft index was 7.00, the highest value among the three groups.
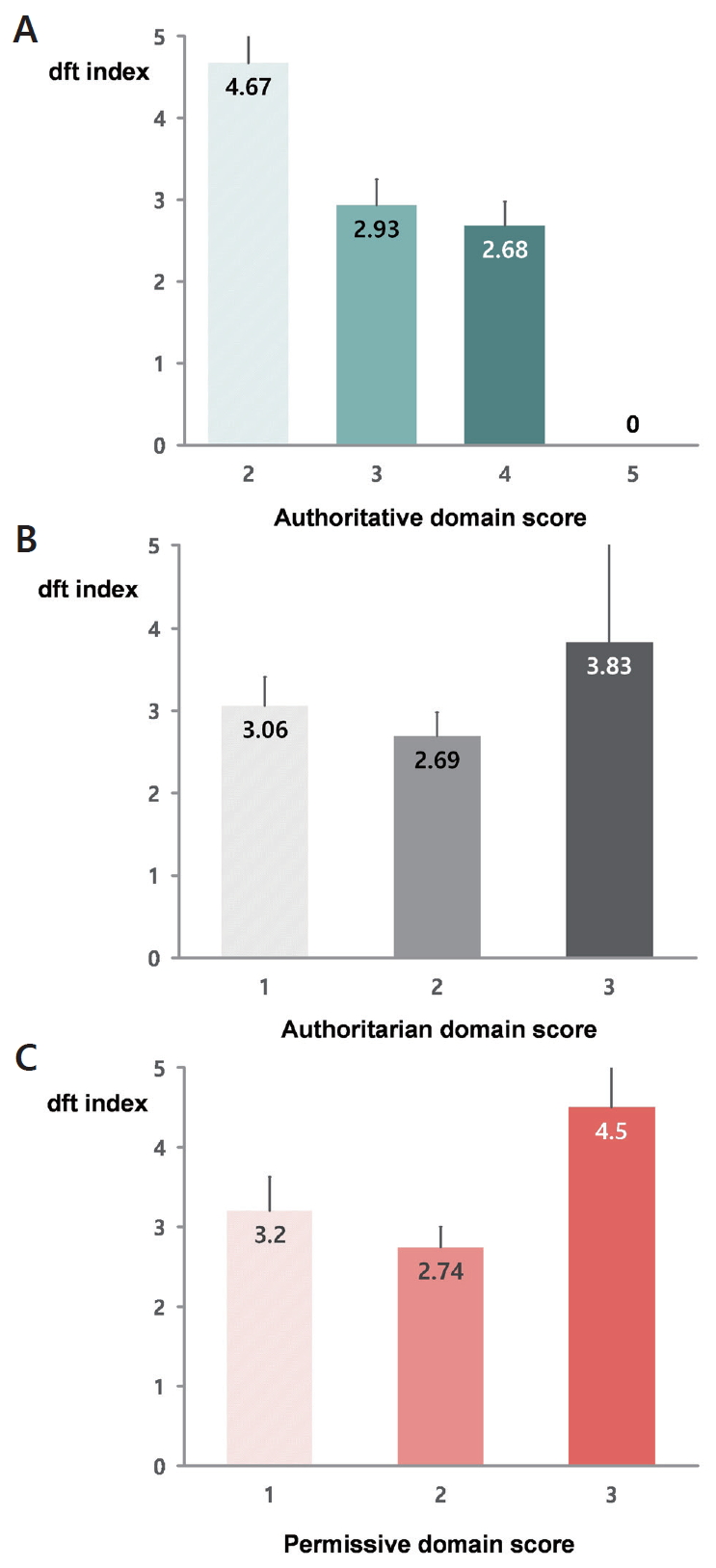
According to each subdomain, the dft index was compared. The distribution of mean scores in each subdomain of the parenting styles was 1 to 5, so it was divided into five sections. In the authoritative domain, the higher the authoritative tendency, the lower the dft index (Fig. 3A). Unlike the trend of the authoritative domain, the dft index increased as the authoritarian tendency became stronger (Fig. 3B). As parental tolerance increased, the child’s dft index also increased (Fig. 3C).
Ⅳ. Discussion
The association of parenting style with ECC would not be determined, as all the three types of parenting styles could not be differentiated in the sample. In a study of ECC risk factors in children aged below four years, Seow et al.[10] reported a tendency for increased laxness, verbosity, and the over-reaction type of parenting behavior among the parents of children with ECC compared to caries-free control children, but the difference was not statistically significant. In an earlier study carried out in children between the age group of 2 - 14 years by Seran et al.[11], no relationship could be established between oral health status and parenting style assessed with PSDQ. However, race/ethnicity, level of parents’ education, and socioeconomic status were associated with oral health status[11]. Howenstein et al.[5] reported that the prevalence of dental caries was statistically significantly lower in authoritative parental children. In the present study, compared to the other groups in the children of authoritative parents, the dft index was lower although not statistically significant. Besides, there was a tendency for the dft index to be lowered as the parenting style exhibited an authoritative trend.
In general, an authoritarian group with a strong dictatorial tendency might be considered to have a lower dft index. However, in this study, the dft index was lower in the authoritative group compared to the authoritarian group. Kumar et al.[4] showed that the more authoritative the parents were, the lower the risk of caries. They also demonstrated that parents who were coercive and authoritarian did not help improve their children’s oral health[4]. Previous studies described that the authoritarian parenting style was generally oppressive, but oral hygiene was not the primary concern and resulted in a higher incidence of dental caries[5].
A systematic review by Hooley et al.[6] revealed that children with higher birth order and belonging to large size families are more prone to caries[12]. Wyne et al.[13] also reported that birth order was related to caries, with the first-born child presenting a higher experience of caries. This could be attributed to the relative lack of knowledge on the part of new parents in managing a child’s behavior and lack of dental health education and dietary counseling[13]. In this study, multi-child families showed a higher dft index when compared to one-child families. However, unlike previous studies, the lower the birth order, the more likely caries were to occur (p = 0.020). This was because it might be related to show a tendency of twoincome parents in recent years. The number for two-income parents had increased, the amount of time and resources invested in their children had decreased. Furthermore, as the number of children in a family increases, the time and effort of each child would be reduced, so they would not pay much attention to oral health care.
The following limitations existed in this study. Firstly, the PSDQ questionnaire had a limit on reliability as an assessment tool, especially for Korean parents. The reason why the PSDQ questionnaire was selected as an assessment tool of parenting style was that a lot of previous related studies used the PSDQ questionnaire, and review studies about the reliability and validity of PSDQ suggested that PSDQ exhibited high reliability and validity[14]. Although defining the parenting style as one tendency itself was limited, it was considered meaningful to typify the parenting style, so PSDQ was chosen. Nevertheless, in our study, the reasons why the results of PSDQ were biased towards one side were that Korean parents tended to be unfaithful to external research that must be submitted to the kindergarten class or school. Moreover, the parents tended to provide false statements in self-reported questionnaires.
Secondly, as a result of the survey, there was a possibility that the permissive parenting style appeared as one person and resulted in errors in statistical analysis. Therefore, the dft index according to the overall tendency of each subdomain of each parenting style was analyzed. To complement these points in future studies, they should be used to supplement and evaluate future research using other advanced parenting methods such as clustering to assess parenting styles[15].
Although the biological and environmental factors associated with early childhood caries were well established, the importance of parenting styles of preschoolers was undervalued compared to these factors. Therefore, the dentist must play a role in identifying and guiding the parenting style in the dental office. In fact, to prevent dental caries in children, a patient-centered approach is required in addition to the existing population-based approach.
Ⅴ. Conclusions
There were no statistically significant differences between dental caries and parenting styles. Authoritative parenting styles resulted in children having low rates of dental caries (low dft index). The stronger the authoritative tendency of the parents, the lower the experience of dental caries in the children. The lower the birth order, the more likely caries were to be induced (p = 0.020). The dentist must recognize the parenting styles and their importance, and be aware of the importance of parent education.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






