성장기 II급 부정교합 환아의 기능성 악교정 장치의 치료 효과에 관한 연구
Study of Functional Appliance for Treatments of Children and Adolescents with Class II Malocclusion
Article information

Abstract
이 연구의 목적은 소아청소년에서의 2급 부정교합 치료에 사용되는 기능성 악교정 장치의 효과 및 치료 시기에 따른 효과를 평가하고자 하였다. 경희대학교 소아치과에 내원한 2급 부정교합환자 30명을 대상으로 하였으며 치료에 사용된 기능성 악교정 장치에 따라 군을 나누었다. 치료 시기에 따른 비교를 위하여 경추골 성숙도 방법을 이용하여 2개의 군으로 나누어졌다. 각 실험군은 치료 전(T0)과 치료 후(T1)의 측모두부방사선사진을 비교 분석하였다.
기능성 악교정 장치 중, Twin block과 Activator는 하악골의 길이(Co-Gn)와 하안모의 길이(ANS to Me)의 유의한 증가를 보였으며, overjet과 overbite의 유의한 감소를 보였다. 반면 Fränkel appliance를 이용한 환자에서는 상하악 간의 관계 및 overjet의 유의한 개선을 보였다. 최대성장기에 기능성 악교정 장치를 사용하였을 때 최대성장기 전에 사용한 것에 비하여 유의한 하악 길이의 증가, 상악과 하악간의 관계 개선, overjet의 감소, 하악 중절치의 순측 경사의 증가를 보였다. 이 연구를 통하여 2급 부정교합을 가진 소아청소년에서 기능성 악교정 장치의 효과를 검증하였으며, 최대성장기에 치료를 시행하는 것이 더 효과적인 것을 확인하였다.
Trans Abstract
The purpose of this study was to evaluate the skeletal and dentoalveolar effects and optimal timing for treatment of class II malocclusion with functional appliances in children and adolescents.
A group of 30 patients with class II malocclusion were divided into 3 groups according to their use of functional appliance: Twin block, Activator, Fränkel appliance. The group was also divided into 2 groups according to the cervical vertebrae maturation method. Lateral cephalometric radiographs were analyzed pretreatment (T0) and posttreatment (T1). Among the functional appliances, treatment with Twin block and Activator showed significant increase in the length of the mandible (Co-Gn) and the lower anterior facial height (ANS to Me), whereas the overjet and overbite were significantly reduced. Treatment with Fränkel appliance showed significant improvement in the relationship of maxilla and mandible. In addition, if the functional appliance was used during the period of pubertal growth peak, there was a significant increase in mandibular length, improvement in the relationship of maxilla and mandible, labial inclination of lower incisors and decrease in overjet compared to the treatment before pubertal growth peak. Therefore, this study indicates that using functional appliances for patients with class II malocclusion is effective and the optimal timing for using functional appliances is during pubertal growth peak.
Ⅰ. 서 론
골격성 2급 부정교합은 하악의 위치가 상악의 위치에 비해 상대적으로 후방에 위치한 골격성 부조화를 뜻하며 일반적으로 치열의 부조화를 동반하게 된다[1]. 그 원인은 주로 상하악의 비정상적인 성장에 의하여 치성문제, 연조직의 비정상적인 힘 및 잘못된 습관에 의해서 상악골의 과성장이나 하악골의 저성장이 나타나게 된다. 그 중 가장 많이 언급되는 것은 하악골의 저성장이다[2].
하악골의 저성장을 보이는 2급 부정교합 환자에서 기능성 악교정 장치를 이용한 치료를 통하여 하악골을 전방으로 위치시킴으로 상하악골의 수평적인 길이 차이를 효과적으로 치료할 수 있다[3]. 기능성 악교정 장치는 하악을 지속적으로 전방에 위치시켜 주변 근육이 새로운 위치에 적응하게 하며, 외측익돌근이 retrodiscal pad의 활성을 증가시켜 하악 과두의 성장을 촉진시킨다[4]. 대표적인 기능성 악교정 장치에는 Twin block, Activator, Fränkel appliance, Bionator, Herbst appliance 등이 있다. 이 장치들은 장치의 지지 방식에 따라 조직지지 장치와 치아지지 장치로 분류된다. 이 장치들은 모두 하악을 전방위로 위치시키며, 동물 실험을 통하여 하악의 인위적인 전방위가 골격적 변화를 일으킬 수 있다는 것을 증명하였다[5,6], 이에 대하여 Clark[7]은 하악 열성장 치료를 위해서는 하악 과두 연골의 생물학적 성장을 이용하여야 한다고 주장하였다.
이전의 많은 연구에서 하악의 최대성장기를 찾고자 측모두부 방사선사진을 이용하여 유년기와 청소년기의 하악 성장률의 차이를 조사하였다[8-10]. 이러한 연구 결과를 바탕으로 하악의 최대성장기인 사춘기 성장 곡선의 상승기에 기능성 악교정 장치를 사용하였을 때 가장 바람직한 치료 효과를 얻을 수 있었다[11-15]. 한편 최대성장기 이전의 조기치료를 통하여 치아치조 및 골격의 효율적인 변화 및 사회심리학적인 효과를 얻어 2급 부정교합의 성공적인 치료를 하였다는 연구도 있으나[16,17], 최대성장기 이전 치료에서 골격적 변화를 얻을 수 있으나 최대성장기 치료에 비하여 결과적으로 큰 차이는 없다는 연구도 있다[18].
사춘기의 하악 성장률과 하악의 최대성장기는 몇 가지 골성숙도 평가를 통하여 유추할 수 있다. 이러한 생물학적 지표에는 신장[19], 수완부의 골격적 성숙도[20], 치아의 발달과 맹출[21], 2차 성징[22], 경추골 성숙도[23]등이 있다. 이 중 경추골 성숙도를 통한 하악의 성장 평가는 측모두부방사선사진 촬영만으로 얻을 수 있다. O’Reilly 등[23]은 하악의 성장변화와 경추의 성숙도의 연관성을 평가하기 위해 매년 측모두부방사선사진을 촬영하여 특정한 경추의 성숙 단계와 하악골의 길이, 하악지의 높이, 하악체의 길이의 유의한 증가가 연관이 있다는 사실을 보고하였다.
소아청소년치과에서 2급 부정교합의 성장기 교정을 시행함에 있어서 기능성악교정 장치에 의하여 일어나는 효과에 대해 인지하여야 하며, 또한 성장 시기를 분석하여 올바른 시기의 장치 적용을 통하여 최상의 효과를 얻어야 한다. 이에 이 연구의 목적은 경희대학교 치과병원 소아치과에 소아청소년의 2급 부정교합의 치료를 목적으로 내원한 환자들을 대상으로 본원 소아치과에서 많이 사용되는 기능성 악교정 장치에 의하여 일어나는 골격적, 치아 치조적인 변화를 비교 평가하고자 하였으며, 경추골 성숙도 평가에 기반하여 골격적 성숙도가 다른 단계에 있는 두 군에서의 치료 효과의 차이를 비교하여 기능성 악교정 장치를 이용한 최적의 치료 시기를 조사하고자 하였다.
Ⅱ. 연구 대상 및 방법
1. 연구 대상
2012년 1월부터 2016년 12월까지 본원 소아치과에 내원하여 교정치료를 위한 분석을 시행한 811명의 환자 중 2급 부정교합으로 진단된 환자를 대상으로 하였다. 치료를 시행하여 1차 치료를 종료한 환자를 대상으로 진행하였으며, 치료 중에 기능성 악교정 장치를 사용하지 않은 환자, 1차 치료 후 측모두부방사선사진을 촬영하지 않은 환자들은 제외하였다. 다양한 장치를 통하여 치료가 진행되지만 대상자의 수가 유의성을 확인할 수 있을 정도가 되는 장치인 Twin block, Activator, Fränkel appliance를 사용한 환자를 대상으로 하였다. 이 중 치료 전후의 측모두부방사선사진을 모두 가지고 있는 환자만을 대상으로 하였으며 경추골 성숙도가 최대성장기 이후인 경우를 배제하였다. 이 기준을 만족시키는 30명의 환자를 대상으로 연구를 진행하였다.
2. 연구 방법
1) 골격적 성숙도의 평가
한 명의 조사자가 대상자의 측모두부방사선사진을 모두 관찰한 후 Lamparski가 고안한 평가 방법을 통해 경추골의 6개의 다른 성숙 단계에 따라 사춘기 성장 단계를 유추하였다[24]. 경추골의 6개의 성숙 단계는 2번에서 6번 경추골의 특징지어지는 형태적인 변화에 따라 정하였다(Fig. 1). 기능성 악교정 장치를 사용 시작시의 골격적 성숙도를 경추골 성숙도 방법에 따라서 평가하여 성장기 전 치료군(CVMpre), 성장기 치료군(CVMpeak)의 2개의 군으로 나누어 비교하였다. 성장기 전 성장 가속단계(경추골 1단계에서 2단계)인 환자를 CVMpre에 포함하였고, 최대성장기(경추골 3단계에서 4단계)인 환자를 CVMpeak에 포함하였다.

Cervical vertebrae maturation indicators by Lamparski.
Stage 1: All inferior borders of the bodies are flat. The superior borders are strongly tapered from posterior to anterior. Stage 2: A concavity has developed in the inferior border of the second vertebrae. The anterior vertical heights of the bodies have increased. Stage 3: A concavity has developed in the inferior border of the third vertebra. The other inferior borders are still flat. Stage 4: All bodies are now rectangular in shape. The concavity of the third vertebra has increased, and a distinct concavity has developed on the fourth vertebra. Concavities on 5 and 6 are just beginning to form. Stage 5: The bodies have become nearly square in shape and the space between the bodies are visibly smaller. Concavities are well defined on all six bodies. Stage 6: All bodies have increased in vertical height and are higher than they are wide. All concavities have deepened.
2) 치료 과정
교정분석을 통하여 2급 부정교합을 진단받아 기능성 악교정장치의 사용이 결정되었다면, 장치를 위한 환자의 인상을 채득하였고, 구성교합은 상악, 하악의 중절치를 edge-to-edge 상태로 교합이 3 - 4 mm 정도 열리게 하여 채득하였다. 모든 장치는 같은 기공소에서 만들어졌으며, 만들어진 장치를 하루에 최소 12시간 이상을 착용하도록 하였고, 보호자에게 착용을 확인 및 장려하도록 하였다. 기능성 악교정 장치는 1급 구치 관계를 얻을 때까지 사용되었고 그 후에는 필요하다면 고정성 장치를 이용하여 치아 배열을 완료하였다.
3) 두부계측 분석
모든 측모두부방사선사진은 한 명의 조사자에 의해서 계측되었으며, 계측 프로그램(V-Ceph, version 7.0, CyberMed, Inc., Seoul, Korea)을 사용하여 계측 및 분석되었다. 계측에 필요한 측모두부방사선사진은 교정치료를 위하여 처음 내원한 시기(Time 0, T0)와 기능성 악교정 장치를 이용한 교정치료가 끝난 시기(Time 1, T1)에 촬영되었다. 분석에 필요한 변수들을 모아서 제작된 두부계측분석이 사용되었다. 두부계측분석을 위하여 14개의 기준점을 측정하였으며, 각 계측당 12개의 길이, 7개의 각도를 나타내는 총 19개의 변수들이 생성되었다. 각 변수는 악골의 수평적인 성장을 측정하기 위하여 Pt to Nasion perp (mm), CO-A (mm), Pg to Nasion perp (mm), Co-Gn (mm), Wits (mm), Max.-mand. Differential (mm)을, 수직적인 성장을 위하여 FH to palatal plane (deg), FH to mandibular plane (deg), Palatal pl. to mandibular pl. (deg), ANS to Me (mm), Co-Go (mm), CoGoMe (deg)을, 치아치조적인 성장을 비교하기 위하여 Incisor overjet (mm), Incisor overbite (mm), Interincisal angle (deg), U1 to Pt A vertical (mm), U1 to FH (deg), L1 to Pt A - pogonion (mm), L1 to mandibular plane (deg)을 계측하여 비교하였다(Fig. 2, Table 1).
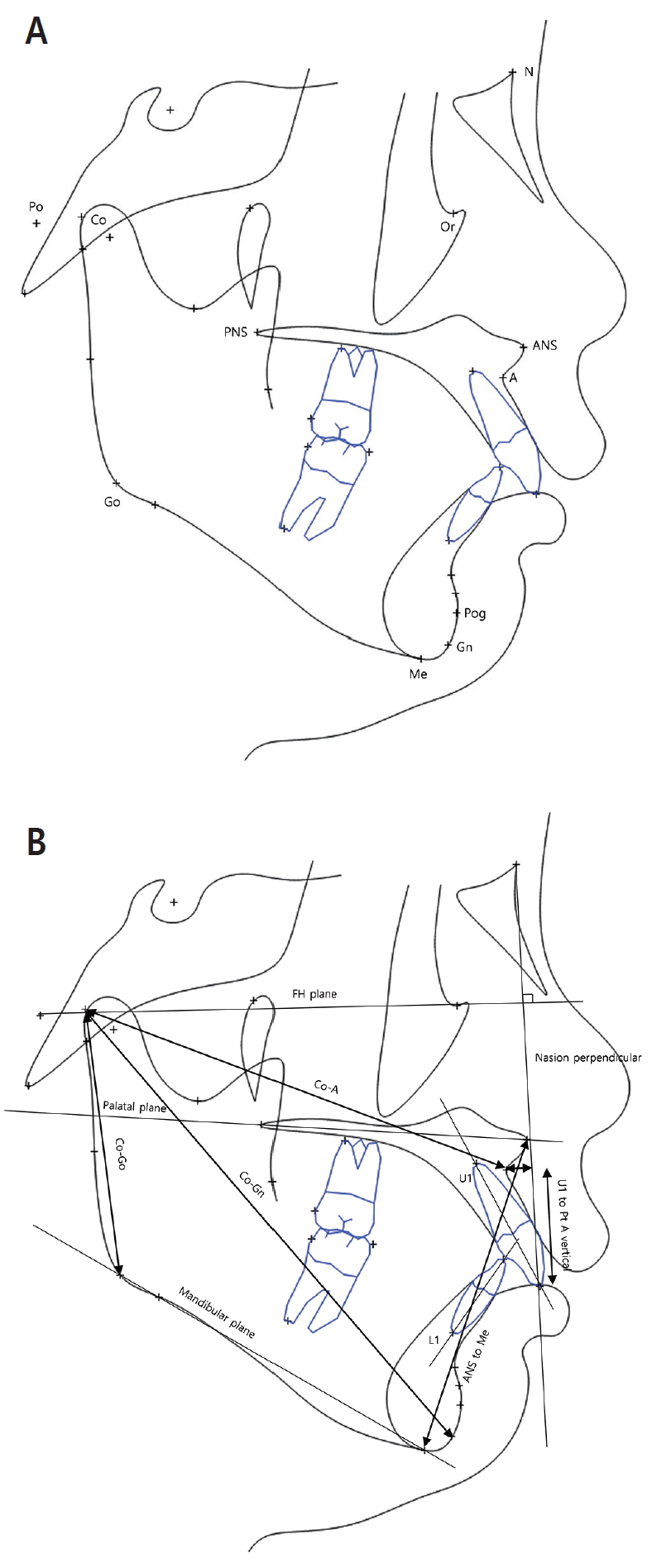
Cephalometric landmarks and measurements (A) landmarks (B) Angles, lines and measurements.

Cephalometric landmarks and measurements
3. 관찰자 내 신뢰도
관찰자 내 신뢰도를 평가하기 위해 총 20명의 측모두부방사선사진을 무작위로 선정하여 8개월 간격으로 2번에 걸쳐 측정하였다. 급내 상관계수(Intra-class correlation coefficient)를 이용하여 관찰자 내 신뢰도를 평가한 결과, 0.74로 중증도 이상의 신뢰도를 보였다.
4. 통계적 분석
Shapiro-Wilk test를 통하여 두부계측분석에 사용된 변수들이 정규분포를 나타내지 않음을 확인하였다. 각 장치들의 효과를 비교하기 위해 장치 사용 전과 사용 후의 변수들이 비교되었다. 또한, 치료 시작 시기가 다른 두 군(CVMpre, CVMpeak)의 T0와 T1사이의 변수들의 차이가 비교되었다. 모든 통계적인 비교는 각 군의 표본수가 부족했기 때문에 비모수 검정을 통해 이루어졌다(Mann-Whitney U-test, p < .05). 모든 통계적인 계산은 통계 프로그램(SPSS for Windows, version 25.0; IBM Inc., Chicago, USA)을 이용하였다.
Ⅲ. 연구 결과
1. 피험자 분포
전체 조사대상은 30명이었으며, 이 중 Twin block을 사용한 환자는 14명(남자 8명, 여자 6명), Activator를 사용한 환자는 10명(남자 6명, 여자 4명), Fränkel appliance(남자 2명, 여자 4명)를 사용한 환자는 6명이었다. Twin block군의 평균나이는 10.8세, Activator군의 평균나이는 11.3세 그리고 Fränkel appliance군의 평균나이는 10.3세였다.
CVMpre군은 경추골 성숙도 1, 2단계의 각 18명의 환자로 기능성 악교정 장치의 첫 사용 시기가 사춘기 최대성장기 전인 환자들로 구성되었다. T0의 평균나이는 10.1세였으며, T1에서의 평균나이는 12.3세였다. 치료 종료시의 경추골 성숙도 단계는 모두 3 단계 이하로, 사춘기 최대성장기 전이었다. 기능성 악교정 장치의 실제 사용기간은 평균 1.0년이었으며, T0와 T1사이의 간격의 평균은 2.3년이었다. CVMpeak군은 경추골 성숙도 3, 4단계의 12명의 환자로 기능성 악교정 장치의 첫 사용 시기가 사춘기 최대성장기인 환자들로 구성되었다. T0의 평균나이는 11.4세 였으며, T1에서의 평균나이는 15.1세였다. 기능성 악교정 장치의 실제 사용기간은 평균 0.7년이었으며, T0와 T1사이의 간격의 평균은 2.6년이었다(Table 2).
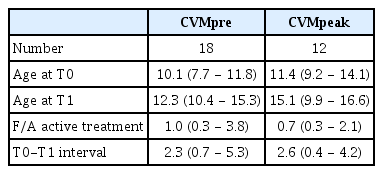
Characteristics of samples Unit: Average year of age (range)
2. Twin block의 치료 효과
Twin block을 사용한 치료에서 하악의 수평적 크기 변화를 나타내는 변수 Co-Gn의 유의한 증가를 보였다. 수직적인 크기 변화 측면에서는 하안모의 길이 변화를 나타내는 변수 ANS to Me의 값과 하악각의 크기 변화를 나타내는 CoGoMe의 값이 유의하게 증가하였다. 치아치조 변화를 나타내는 변수 중에는 Incisor overjet과 Incisor overbite값이 유의한 감소를 보였다(Table 3).
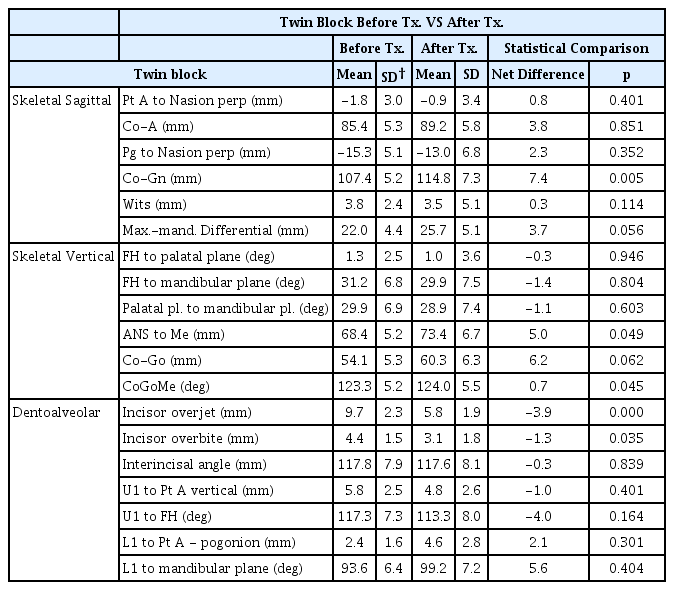
Changes in cephalometric variables by Twin block (n=14)
3. Activator의 치료 효과
Activator를 사용한 치료에서도 하악의 수평적 크기 변화를 나타내는 변수 Co-Gn의 유의한 증가를 보였다. 수직적인 크기 변화 측면에서는 하안모의 길이 변화를 나타내는 변수 ANS to Me의 값이 유의하게 증가하였다. 치아치조 변화를 나타내는 변수 중에는 Incisor overjet과 Incisor overbite값의 유의한 감소를 보였다(Table 4).
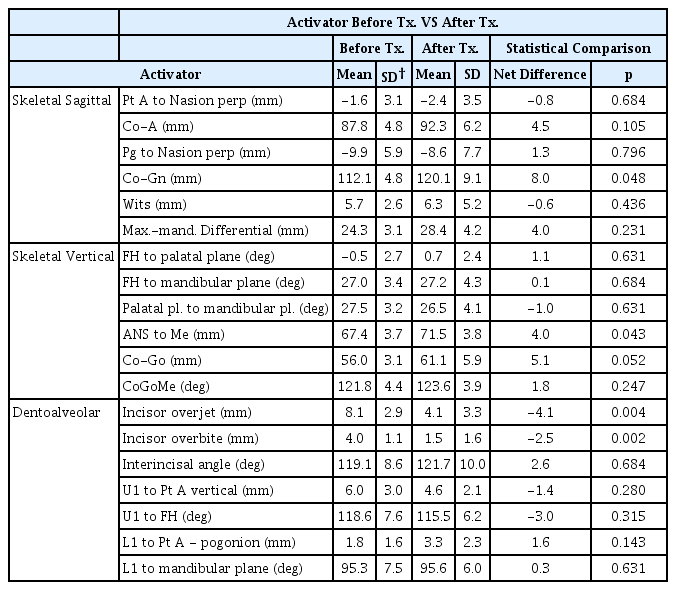
Changes in cephalometric variables by Activator (n=10)
4. Fränkel appliance의 치료 효과
Fränkel appliance를 사용한 치료에서는 상악과 하악의 길이의 차를 나타내는 변수 Max.-mand. Differential 값과 치아치조 변화를 나타내는 변수 중에는 Incisor overjet 값의 유의한 감소를 보였다(Table 5).
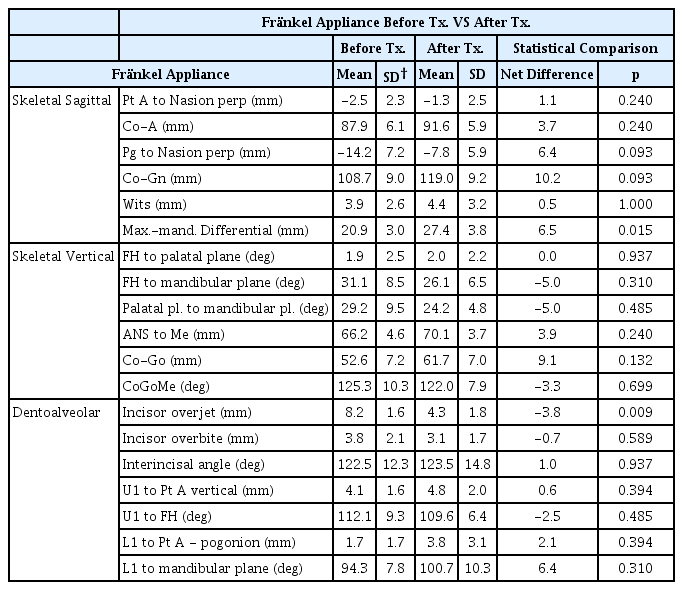
Changes in cephalometric variables by Fränkel appliance (n=6)
5. 치료 전 CVMpre군과 CVMpeak군의 비교
치료 전의 CVMpre군과 CVMpeak군 사이의 변수들의 비교에서는 통계적으로 유의한 차이를 발견할 수 없었다. 두 군은 모두 6 mm 이상의 overjet과 2급 교합관계를 가지고 있었다(Table 6).
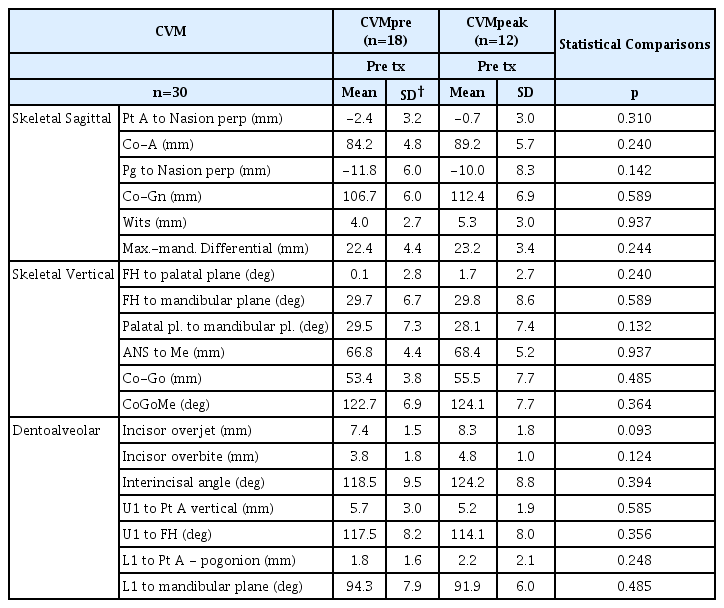
Comparison of cephalometric variables between CVMpre group and CVMpeak group before treatment
6. 치료 전후 CVMpre군과 CVMpeak군의 비교
CVMpre군과 CVMpeak군의 치료 전후 변수들의 비교에서는 CVMpeak군의 하악골의 수평적인 전방 위치를 나타내는 변수 Pg to Nasion perp, 하악골의 크기를 나타내는 변수 Co-Gn, 상악골과 하악골의 크기 차이를 나타내는 변수 Max.-mand. Differential, Incisal overjet의 변화가 CVMpre군에 비해 유의하게 크게 나타났다(Table 7).
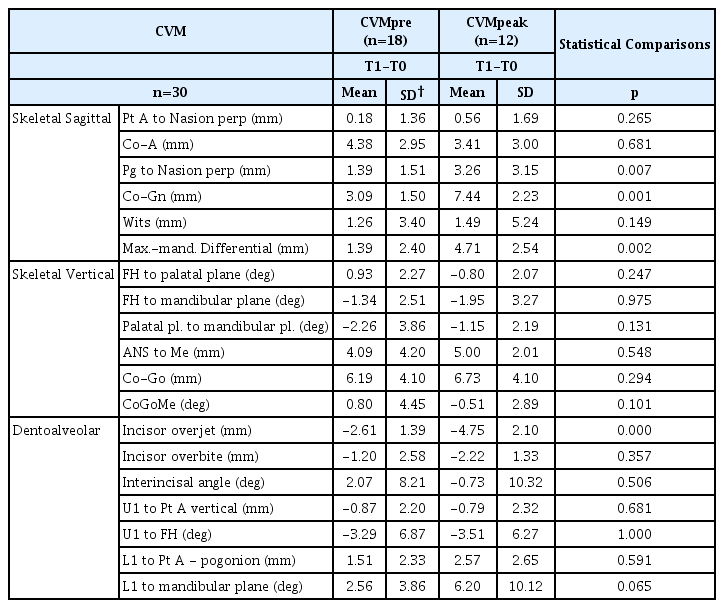
Comparison of cephalometric variables between CVMpre group and CVMpeak group after treatment
Ⅳ. 총괄 및 고찰
2급 부정교합의 치료는 사춘기 최대성장기에 시행하는 것이 효과적이다. 그러나 사회적인 놀림이나 정서적인 문제점을 가지는 경우, 깊은 과교합에 의하여 악골 저성장이 예상되는 경우에 조기 치료를 시행하고 있다[1]. 치료 시기에 관한 논쟁과 치료 결과에 대한 비교 분석은 꾸준하게 이루어지고 있다[3,4,13-15]. 이는 2급 부정교합의 치료 효과가 다양한 인종의 성장 양상과 치료를 시행하거나 받는 사람들의 사회문화적인 원인에 의한 것이라고 생각한다.
2급 부정교합치료를 위한 하악의 전방 견인력이 하악 과두 연골 성장을 자극하여 하악의 형태적 크기 변화와 교합의 변화를 일으킬 수 있다는 것은 동물실험을 통하여 증명한 바 있다[25-27]. 그러나 실험동물인 쥐는 이상적인 장치 사용기간과 빠른 성장률로 인하여 성장 수정을 몇 주 만에 얻을 수 있으나 사람의 경우 최적의 장치 사용기간을 얻는 것이 제한적이며, 비슷한 성장 수정을 얻기 위해서는 몇 달이나 몇 년의 시간이 필요하다. 또한 Creekmore와 Rodney[28], Mills[29]에 따르면 기능성 악교정 장치에 의한 하악의 성장 또한 수평적인 방향이 아닌 수직적인 방향으로 일어날 수 있고, 이에 따라 안모에 악영향을 끼칠 수 있다고 하였다. 이에 이 연구는 우리나라 학령기 환자에서 2급 부정교합에 널리 사용되는 기능성 악교정 장치의 효과에 대해 확인하고자 진행하였다.
Twin block과 Activator는 하악을 전방위 시키고 여러 구강 주위근의 활성을 변화시키는 방법으로 하악의 성장을 유도하는 장치라는 점에서 유사하다. 다만 Activator는 하나의 큰 아크릴릭 레진 판이 구강 내에 들어가게 되고, Twin block은 두개의 분리된 상악, 하악용 아크릴릭 레진이 구강 내에 들어가서 발음과 저작을 가능하게 하여 상대적으로 긴 착용시간을 얻을 수 있다[30]. 이전의 두 장치의 효과에 대한 비교연구[31]에서 두 장치의 연조직 및 경조직에 대한 효과는 유사하였으나 가장 큰 차이는 하악의 전방 이동량이었다. 이 연구에서도 Twin block과 Activator를 사용한 군의 상악에 대한 유의한 변화는 찾을 수 없었다. 이전 연구들에서 주장되었던 장치에 의해 하악이 전방위로 이동하면서 그 반대의 힘이 상악을 후방으로 미는 힘이 상악의 성장을 억제한다는 “헤드기어 효과”는 보이지 않았다[32,33]. 하악에서는 Twin block을 이용한 이전 연구[34,35]와 Activator[36]를 이용한 이전 연구에서 확인하였던 것처럼 이 연구에서도 하악골 길이의 유의한 증가를 보였다(Co-Gn). 그러나 하악골의 길이 증가에 따른 Pogonion의 전방 이동은 유의한 차이를 보이지 않았다(Pg to Nasion perp). 또한 상하악간 관계의 변화를 나타내는 변수인 Wits appraisal과 Max.-mand. Differential의 유의한 변화는 확인할 수 없었다. 수직적인 변화에서는 구개 평면이 Frankfort horizontal 평면과 이루는 각도나 하악 평면이 Frankfort horizontal 평면이나 구개 평면과 이루는 각도는 유의한 차이가 없었다. 그러나 하안모의 길이(ANS to Me)는 유의하게 증가하였다. 이러한 의도하지 않았던 하안모의 길이 증가는 기능성 악교정 장치에 의해 하악의 성장이 수직적인 방향으로 일어날 수 있다는 이전의 연구결과[28,29]와 유사하였으며 이에 대한 주의가 요구된다. 또한 다른 기능성 악교정 장치를 사용한 Malta 등[37]에 의한 연구에서도 이와 유사한 악영향이 나타나는 것으로 보고되고 있다.
치아치조관계에 대하여 이 장치들은 Incisor overjet과 Incisor overbite의 유의한 감소를 보였는데, 이는 치료 전후의 상악 중 절치와 하악 중절치의 기울기와 위치의 유의한 변화와 장치사용에 따른 구치부의 맹출로 인한 효과인 것으로 해석할 수 있다. 이는 Twin block과 Activator가 필연적으로 상악 절치의 구개측 경사와 하악 절치의 순측 경사를 일으킨다는 이전 연구[38,39]와 유사한 결과를 보였으며, 이는 악정형 장치를 이용하여 골격적인 변화만이 아니라 치아치조 관계에도 영향을 준다는 결과를 보여주었다.
Fränkel appliance는 조직지지 장치로 하악을 전방위로 위치시키는 기능 외에 근육의 비정상적인 기능을 차단하기 위한 전정 차폐판과 하악 순측 패드, 그리고 하악 설측 차폐판이 주된 부분을 구성하며, 구강 내 힘의 불균형을 개선하고 근신경계에 작용하여 개선된 상태를 훈련시킨다[40]. 이 연구에서 Fränkel appliance를 사용한 군에서는 상하악간 관계의 변화를 나타내는 변수인 Max.-mand. Differential의 증가와 overjet의 감소 외에 다른 변수들의 유의한 차이는 확인할 수 없었다. Fränkel appliance를 이용한 이전 연구에서도 하악골의 골격적 변화는 없었으며 상하악간 관계의 유의한 개선을 보였다[40]. 상악골과 하악골의 유의한 크기 변화를 보이지 못하였는데 상하악간 관계의 유의한 개선을 보인 이유에 대해서는 경우에 따라 상악골의 수평적 성장 억제와 하악골의 수평적 성장 유도가 다른 정도로 일어났을 것으로 생각할 수 있고 실험군의 크기가 늘어난다면 보다 확실한 결론에 도달할 수 있을 것이다.
한편 치아지지 장치와 조직지지 장치의 차이에서는 장치가 힘을 받는 부분을 생각해 볼 때, 치아를 통한 힘의 전달이 아닌 악골에 직접적인 힘을 주는 조직지지 장치가 치아지지 장치보다 치아치조변화를 더 적게 일으키면서 하악의 골격적 변화를 유도할 것이라고 생각할 수 있다. 그러나 이 연구에서는 치아지지 장치인 Twin block과 Activator에서 하악의 수평적인 성장 및 수직적인 성장을 확인하였으며, Fränkel Appliance에서는 하악의 유의한 성장을 관찰할 수 없었다. 이는 치아지지 장치가 조직지지 장치보다 치아로부터 확실한 장치의 유지력을 얻어 더 안정적인 하악의 전방위를 얻을 수 있다는 점과, Twin block과 Activator는 상대적으로 긴 시간을 착용할 수 있도록 설계되었지만, Fränkel Appliance는 장치의 부피가 크고 일상생활에서 착용하기가 어렵기 때문에 착용시간이 상대적으로 짧다는 점을 이유로 들 수 있다. Twin block과 Fränkel Appliance의 효과를 비교한 이전 연구에서도 이와 같은 결과를 확인할 수 있다[41]. 따라서 하악의 열성장에 의한 2급 부정교합의 치료에 하악의 수평적 성장 및 수직적 성장을 얻기 위한 장치로는 치아지지 장치인 Twin block 과 Activator를 사용하는 것이 조직지지 장치인 Fränkel Appliance를 사용하는 것보다 더 적절한 효과를 얻을 수 있다.
한편 2급 부정교합에 대한 기능성 악교정 장치의 효과적인 치료 시기에 대한 연구에서는 최대성장기를 포함한 시기에 장치를 사용하였을 때 수평적인 성장에서 효과적인 것을 알 수 있었다. 구체적으로 하악의 상대적인 위치를 나타내는 계측인 Pg to Nasion perp의 차이가 통계적으로 유의하였는데, CVMpre의 경우 평균 1.39 mm, CVMpeak의 경우 평균 3.26 mm로 나타났고 이는 최대성장기를 포함한 시기에 장치를 사용할 때 하악이 2급 부정교합의 치료에 도움이 되는 방향인 전방으로 더 많이 이동한다는 것을 의미한다. 하악의 수평적인 길이의 계측인 Co-Gn의 차이도 통계적으로 유의하였는데, CVMpre의 경우 평균 3.09 mm, CVMpeak의 경우 평균 7.44 mm로 나타났고 이는 최대성장기를 포함한 시기에 장치를 사용할 때 하악의 수평적 성장이 더 많이 일어난다는 것을 의미한다. 상하악간 수평적인 길이의 차를 의미하는 계측치인 Max.-Mand. Differential의 차이도 통계적으로 유의하였는데, CVMpre의 경우 평균 1.9 mm, CVMpeak의 경우 평균 3.26 mm로 나타났고 이는 앞의 계측 Co-Gn의 결과와 함께 해석하였을 때 최대성장기를 포함한 시기에 장치를 사용할 때 하악의 수평적인 길이 성장으로 하악과 상악의 차이가 더 커지므로 2급 부정교합이 해소되는 방향으로 더 많이 성장하는 것을 의미한다. 또한 치아치조 성장과 수직적인 성장 면에서는 치료 시기의 차이가 유의한 차이를 만들지 못한다는 것을 알 수 있었고, 이는 최대성장기 전이 아닌 최대성장기에 장치를 사용한다면 하악의 성장이 치아치조적인 성장이나 수직적인 골격적 성장이 아닌 수평적인 골격적 성장 면에서 더 많은 유의한 차이를 보인다는 것을 의미한다. 이 연구 결과는 최대성장기를 포함한 시기의 악교정 장치의 사용이 최대성장기 전의 장치의 사용보다 하악의 바람직한 골격 성장 수정을 유도한다는 이전의 연구 결과들과 같은 결론을 얻었다[11-15]. 이러한 계측 수치의 차이를 보이는 것은 모두 장치 사용에 의한 것보다는 장치를 사용할 때 하악의 성장 방향을 2급 부정교합 해소에 유리한 방향으로 유도하고, 하악의 성장은 최대성장기에 더 많이 일어나게 되므로 이 시기에 장치를 사용한다면 하악을 2급 부정교합을 해소하는 방향으로 더 많이 성장시킬 수 있기 때문이다. 이에 따라 2급 부정교합의 치료를 위해 하악의 수평적인 성장이 필요할 때, 경우에 따라서는 많은 양의 성장이 필요할 수 있으므로 최대성장기를 포함한 시기에 치료를 하는 것이 치료의 효율성을 높일 수 있을 것이다.
임상에서 기능성 악교정 장치를 사용하여 2급 소아청소년 환자를 치료할 때, 그 예후는 만족할 만한 경우도 있지만 실망스러운 경우도 있다. 이 때문에 임상가는 장치 사용에 대한 의문이 생기는 경우가 있다. 또한 우리나라의 학령기 아동들의 생활에서 기능성 악교정 장치의 이상적인 장착시간을 지키기는 것에 대한 부담 또한 2급 부정교합 치료의 걸림돌이 될 수 있다. 이 연구의 의의는 한국 소아청소년에서 장치 사용에 있어 과학적인 근거를 제공하여 하악 열성장인 2급 소아청소년 환자의 치료에 적극적인 기능성 악교정 장치의 사용이 하나의 치료 방법이 될 수 있음을 보였고, 교정치료를 목적으로 초진으로 내원하는 환자에서 대부분 촬영하게 되는 측모두부방사선사진을 통하여 얻을 수 있는 경추골 성숙 단계를 이용하여 최대성장기를 유추하여 치료를 시작하는 것이 적절한 장치 사용 시기임을 보였다.
그러나 이 연구에는 몇 가지 한계점이 있다. 우선 각 군에 포함된 환자 수가 적다는 점이다. 여러 가지 기준 및 조건을 충족해야 하는 2급 부정교합의 치료에 대한 논문에서 대상자의 수를 늘리기에는 한계가 있다고 해도 대상자 수는 다른 관련 논문과 다소 차이를 보이고 있고, 특히 세가지 기능성 악교정 장치를 비교한 부분에서 Fränkel appliance의 실험군의 수는 통계를 통하여 유의한 수치를 확인할 수 있었지만 장치 사용의 과학적 근거가 되기에는 수가 부족하다(Table 8). 5년간의 기간에도 대상자의 수가 부족했었던 이유로는 과거 치료 후에 측모두부방사선사진을 촬영하지 않은 환자가 다수 존재했기 때문으로, 치료 후에 반드시 측모두부방사선사진을 촬영하도록 해야 할 것이다. 더욱 의미 있는 결과를 위해서는 추후 연구에서는 관련 연구들의 결과를 수집하여 더 큰 결과를 만드는 것이 필요하다. 두 번째는 Table 2에서 보이듯이 T0, T1의 간격과 기능성 악교정 장치의 실제 사용시기의 차이를 보이는데, 이는 진단 시에 환자의 측모두부방사선사진을 촬영하게 되는데, 처음 진단을 하고 치료시기를 미루거나, 기능성 악교정 장치 사용 후 바로 측모두부방사선사진을 촬영없이 고정성 장치로 보정 치료를 하는 경우가 많다. 이 때문에 자연적인 성장에 의한 것인지 기능성 악교정 장치에 의한 실제 치료 효과를 보이는 것인지 판단하기에 모호해질 수 있다. 이러한 모호성을 줄이기 위해 이후 연구에서는 포함 기준에서는 진단 후 치료시기를 미룬 환자를 제외해야 할 것이며, 기능성 악교정 장치 치료 후 보정 치료 전에 측모두부방사선사진을 촬영하여 이를 연구에 포함하여야 할 것이다.
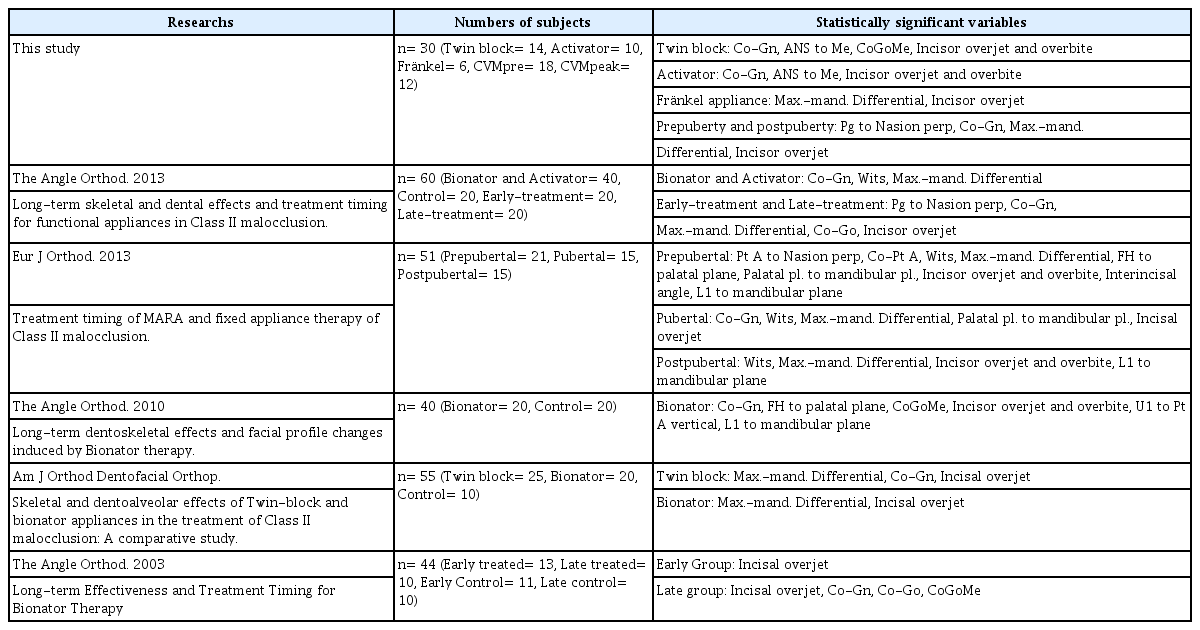
Numbers of subjects and statistically significant variables in other class II related researchs
세 번째는 대조군의 부재이다. 2급 부정교합 환자를 치료하지 않고 연구의 목적으로 관찰하는 것은 윤리적인 문제가 발생하기 때문에 대조군을 추가하는 것은 어려울 수 있으나, 기능성 악교정 장치의 효과에 대해 보다 정확한 연구를 위해서는 대조군이 필요하다. 네 번째는 대상을 후향적으로 관찰을 한 연구 설계 자체의 한계이다. 비록 교정학적인 연구에서 무작위 대조군 연구(Randomized Controlled Trials)는 윤리적 문제로 인하여 진행되기 힘들지만 이 주제에 대한 보다 나은 연구를 위해서는 이러한 한계를 극복한 연구가 필요할 것으로 보인다.
Ⅴ. 결 론
이 연구는 2급 부정교합을 보이는 30명의 환자를 대상으로 기능성 악교정 장치를 이용한 치료의 효과 및 치료시작 시기에 따른 효과의 차이를 알아보고자 하였다. 먼저 기능성 악교정 장치 중 Twin block 및 Activator를 사용한 치료에서는 하악골의 길이 증가, 하안모의 길이 증가, overjet 및 overbite의 감소 효과를 기대할 수 있으며, Fränkel appliance를 사용한 치료에서는 상하악 관계의 개선을 기대할 수 있다. 또한 기능성 악교정 장치를 사용한 2급 부정교합 치료를 최대성장기에 시행한다면 하악의 바람직한 골격적인 성장을 유도할 수 있으며, 이에 따라 3, 4번 경추골의 하연의 오목함이 관찰되는 CVM III, CVM IV 시기에 장치를 사용한다면 최대성장기 전의 치료와 비교하였을 때 하악골의 길이 증가와 턱 끝의 전방이동 및 overjet의 감소가 유의하게 일어난다.