



Ⅰ. Introduction
Amelogenesis imperfecta (AI) is a genetically and clinically heterogeneous group of inherited enamel defects[1]. It primarily affects the formation and/or calcification of enamel[1]. Hypoplastic enamel features reduced enamel thickness with normal hardness, whereas hypocalcified or hypomaturation enamel features reduced hardness and discoloration with normal thickness[2]. AI occurs either in isolation or in association with other dental abnormalities[1,2]. Dental anomalies previously described in association with AI include taurodontism, congenitally missing teeth, eruption failure, crown and root resorption, pulp calcification, and hypercementosis[1,2]. Eruption failure as well as crown and root resorption have been reported in patients with autosomal recessive hypoplastic AI[2-4]. AI may occur concomitantly with systemic disorder or in association with syndromes, such as Jalili syndrome[5], Raine syndrome[6], epidermolysis bullosa[7], tricho-dento-osseous syndrome[8], and AI and gingival fibromatosis syndrome (AIGFS, OMIM#614253)[9]. A rare syndrome associating AI with nephrocalcinosis, which was first described by MacGibbon[10] in 1972, was named as Enamel Renal Syndrome (ERS, OMIM#204690)[11]. ERS shows pathognomotic oral characteristics easily detectable at an early age, which proceeds the onset of renal involvement. Therefore, pediatric dentists are likely to become the first health practitioners to recognize this syndrome and refer to a nephrologist for prevention of possible renal failure. The purpose of this study is to describe the oral phenotypes of a patient with ERS, which is the first case report in South Korea.
Ⅱ. Case Report
A 6-year-old girl was referred to the Department of Pediatric Dentistry, Ajou University Dental Hospital from a local dental clinic with a presumptive diagnosis of Amelogenesis imperfecta (AI). According to her mother, none of her family members had dental anomalies like her. Her medical history and general physical condition were unremarkable during her first visit.
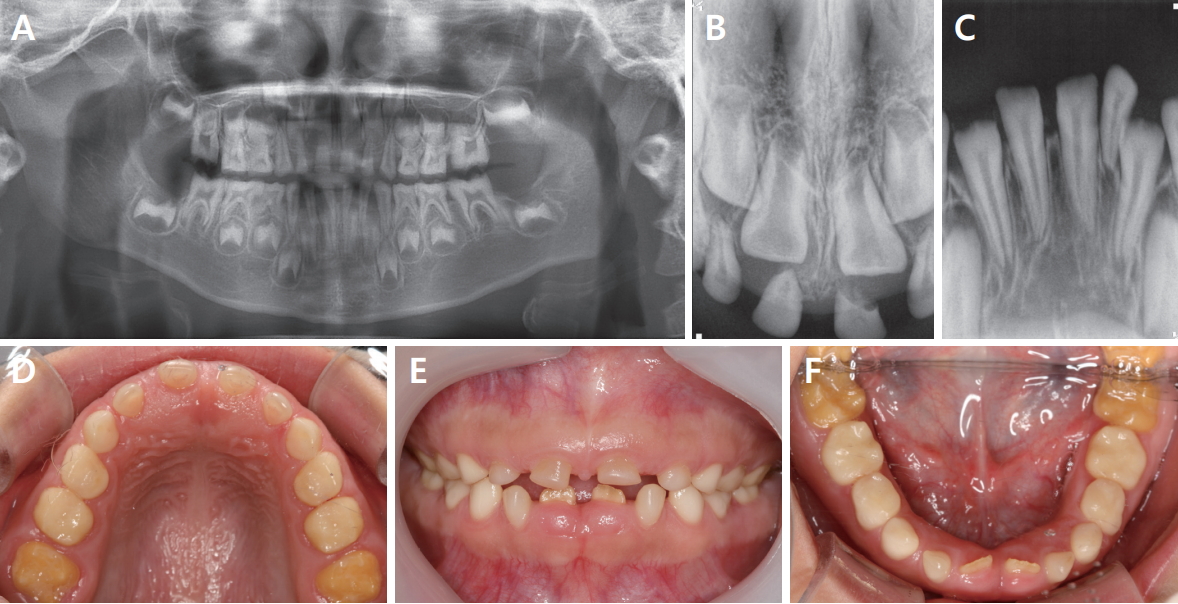
The intraoral examination revealed a thin enamel layer on all erupted primary and permanent teeth. The teeth were small-sized and yellow discoloration was observed on the erupted permanent teeth (Fig. 1). Panoramic radiograph taken at age 7 showed no sign of taurodontism, congenital missing, pulpal calcification, or eruption disturbance. The roots of permanent tooth germs were developing well. However, there was no density difference between the enamel and dentin layer throughout all primary or permanent dentition whether erupted or unerupted (Fig. 1A-C). Based on clinical and radiographic examination, hypoplastic enamel type IF “rough hypoplastic” or hypoplastic enamel type IG “thin/agenesis enamel” were suspected[12]. We referred her to the pediatric geneticist at Ajou university medical center for genetic evaluation of associated congenital systemic disease or skeletal dystrophy, and no association was found. For dental treatment, it was planned to give her restoration with preformed stainless steel crowns on her permanent first molars after the full eruption.
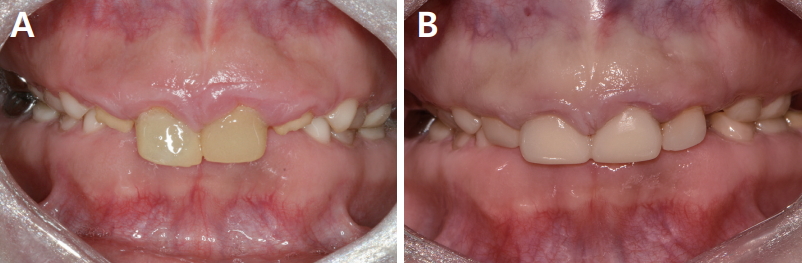
For prevention of enamel fracture, preformed crown restoration was performed on the first permanent primary molar size E4 at age 9. The lower lateral incisors were also restored with composite resin for the same purpose. At age 10, the upper central incisors were restored with Polymethyl methacrylate (PMMA)-based provisional crowns following minimal preparation at age 10 (Fig. 2A). However, the provisional crowns and composite resin filling kept falling out, possibly on account of a deep bite and weak bond strength between enamel and resin. Provisional crowns were remade by shortening the crown length at age 13, and finally they showed favorable retention (Fig. 2B).
At age 10, hematuria was accidently found while she was hospitalized for enteritis at the same institute. A renal ultrasound revealed bilateral nephrocalcinosis. Plasma calcium and phosphate alkaline level appeared normal while the phosphate level was slightly low. It was planned for her to receive a periodic renal examination, but she stopped visiting the nephrologist.
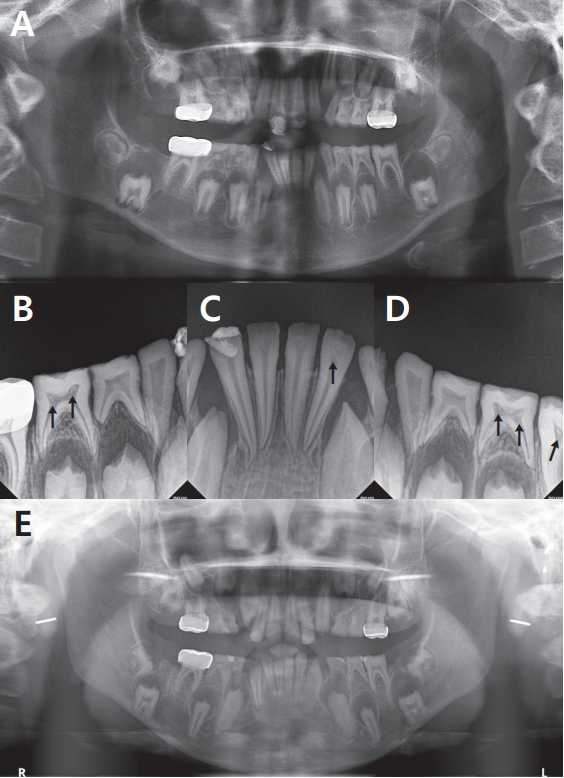
At age 10, enlarged follicles and ectopic impaction of the second permanent molars were obvious in the panoramic radiograph (Fig. 3A). Intrapulpal calcification was present in both lower incisors and lower primary molars in the periapical radiographs taken at age 10 (Fig. 3B-D). We referred her to the Department of Oromaxillofacial Surgery (OMFS) at the same institute for proper treatment of the cystic change in the lower second permanent molars. At OMFS, it was planned for her to be under observation. At age 12, primary canines were extracted to promote eruption of the upper and lower canines. Slow but continuous eruption was observed (Fig. 3E). A panoramic radiograph taken at age 14 showed continued eruption failure and multiple follicular enlargement in premolars despite continued root formation (Fig. 3E). The enlarged follicles were well defined, unilocular, and delineated by a sclerotic border. The lower second permanent molars were inferiorly displaced near the mandibular border while the lower premolars were inferiorly displaced further compared to age 10. The upper second premolars were displaced into the sinus area. Root dilaceration was suspected in the impacted second premolars and molars. The occlusal plane of the impacted second permanent molars were flat to concave without typical cusp morphology (Fig. 3E).
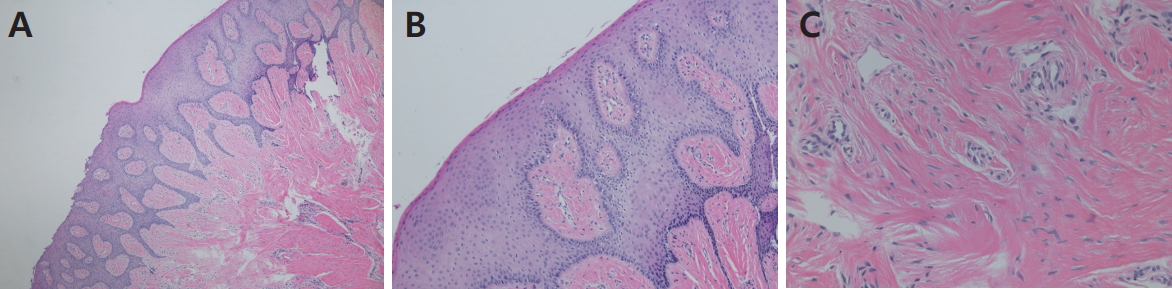
Mild gingival hyperplasia was observed in the anterior of the teeth at age 10 (Fig. 2A). At age 13, gingiva above the impacted lower right canine was removed to promote its eruption, and the excised gingiva was sent for biopsy. The tissue removed during gingivectomy was fixed in formalin and embedded in paraffin. Sections were subjected to hematoxylin and eosin (H&E). The epithelium consisted of an elongated rete peg inserted into underlying fibrous connective tissue. The connective tissue was dense with collagen fiber bundles running without orientation. The histologic characteristics were consistent with gingival fibromatosis (Fig. 4). However, dystrophic calcification, a pathognomonic feature of ERS, was not observed in the connective tissue (Fig. 4C).
The patient was referred to the Department of Orthodontics at the same institute due to the uperupted teeth. A combination of surgical and orthodontic approach was considered to bring the unerupted teeth into alignment despite suspected ankylosis and the limited vertical anchorage that may contra-indicate this orthodontic approach. A high possibility of failure was explained to the patient and her parents. The first target of the orthodontic traction is the first premolars. The orthodontic treatment plan will be modified depending on how the impacted premolars respond to the orthodontic traction force. If this is not feasible, a surgical and prosthodontic approach remains as a theoretical possibility for the future.
The authors conducted an electronic literature search of the keywords ‘amelogenesis imperfecta, eruption failure, follicular cyst’, and found case reports showing similar oral phenotypes. A possibility of ERS was suspected, and it was confirmed while reviewing her past medical records at Ajou Univeristy Medical Center, which revealed bilateral nephrocalcinosis at age 10.
Ⅲ. Discussion
AI can occur in isolation or concomitantly with other dental or systemic disorders. In this case, the patient had hypoplastic enamel in both primary and secondary dentition, suggestive of AI. Bilateral nephrocalcinosis was accidentally detected at the age of 10. She presented other pathognomonic dental features indicating ERS, such as eruption failure and follicular enlargement of multiple posterior permanent teeth, gingival hyperplasia, and intral-pulpal calcification. ERS was diagnosed in patient and a multidisciplinary approach was considered for an eruption failure.
Enamel hypoplasia, tooth shape abnormalities, intrapulpal calcification, eruption failure, and follicular enlargement were observed in this case, which were pathognomonic dental features of ERS[9-11]. AI in this case was classified as hypoplastic enamel type IF “rough hypoplastic” or IG “thin/agenesis enamel”[12]. In panoramic and periapical radiographs, there was no radio-density difference between the dentin and enamel layer, indicating less mineral contents (Fig. 1A-C). The flattened cusps of the first permanent molars may have been caused by attrition (Fig. 1D). However, the concave occlusal surface of the unerupted second molars may have occurred during the developmental process (Fig. 3A,E). In a previous histologic study, progressive resorption and replacement by bone were suspected in impacted permanent molars, possibly leading to an abnormal flat or concave crown morphology[13].
While most AI patients suffer from dental pain and hypersensitivity when eating and drinking, this patient did not express any such discomfort. It is in accordance with the previous report that dental pain or hypersensitivity are not prominent features in patients with hypoplastic enamel type IF “rough hypoplastic” and type IG “thin/agenesis enamel”[14]. However, provisional crown restoration and composite resin filling were performed to prevent further destruction of enamel as well as for esthetic purposes.
Gingival hyperplasia was noted in the upper and lower anterior area in this case, pathologically diagnosed as gingival fibromatosis. Though not observed in this study, focal ectopic calcification was reported in connective tissue near odontogenic epithelium cells in ERS[15]. Recent studies regarding periodontal pathogenesis regarding ERS suggested mutations of FAM20A may be related with AI, abnormal bone remodeling and calcified nodules in periodontal ligament[16]. In other studies, such calcified nodules were also revealed in the pericoronal follicles[13,17]. Histologic analysis of the pericoronal follicles showed hyperplastic odontogenic ectomesenchyme with several round dysplastic calcification, and they were termed pericoronal hamartomas[4,18]. Yonemochi et al .[19] suggested that hamartomatous lesions in the pericoronal areas may induce active tissue remodeling and result in fibrosis in their surroundings, which may impede tooth eruption.
Multiple eruption failure combined with AI presents clinical challenges to dentists. In this case, the large harmatomatous lesion coronal to the impacted teeth and distance of displacement impose difficulties in predicting prognosis of orthodontic traction. In addition, weak bonding strength between hypoplastic enamel surface and resin imposes a possibility of frequent detachment of button used for orthodontic traction. There have been a few case reports of orthodontic tractions in similar cases. As treatment modality for eruption failure related with pericoronal hamartomas, marsupialization is thought to be ineffective because of the lack of cystic fluid in the pericoronal space[20]. Cho et al .[20] have reported possibility of successful eruption of a second premolar after excision of the overlying pericoronal tissue and orthodontic traction. However, slow and inconsistent results of orthodontic traction have been also reported[21]. A long term follow-up revealed that the extraction of primary teeth does not facilitate the eruption of permanent teeth[22]. However, an excisional biopsy and possibility of orthodontic traction still need to be considered before extraction of impacted teeth. The patient in this case is planned to have orthodontic traction of the first premolars. The second premolars and molars are under observation.
Recessive mutation in FAM20A (family with sequence similarities 20 member A) has been identified as the causative mutation for this rare syndrome associating AI and nephrocalcinosis, now termed as ERS[9,23,24]. FAM20A is also identified as the cause of Amelogenesis Imperfecta and Gingival Fibromatosis Syndrome (AIGFS, OMIM #614253)[25]. ERS and AIGFS show similar dental phenotypes. Considering that kidney phenotype has not been investigated fully in AIGFS patients, AIGFS may be ERS where complication in kidney has not been expressed or investigated yet[22].
This rare syndrome of AI associated with nephrocalcinosis, named as ERS, can be diagnosed by clinical and radiographic features. Dure-Molla et al .[22] summarized orodental clinical features typical of ERS as generalized thin hypoplastic or absent enamel, primary and permanent teeth affected, flat cusps on posterior teeth, relative microdontia and spaced teeth, intra-pulpal calcifications, delayed tooth eruptions, impacted posterior teeth with hamartoma-like hyperplastic follicle and altered eruption pathway, root dilacerations of impacted teeth, gingival enlargement with variable severity, and gingival and dental follicle ectopic calcification on biopsies. Each feature is not specific to ERS, but they become pathognomonic features of ERS when they occur together in the absence of other developmental anomalies[22].
In this study, the patient was diagnosed with medullary nephrocalcinosis at age 10. In ERS patients, the renal involvement is often silent in childhood while oral phenotype is evident at an early age. Renal involvement is characterized by bilateral medullary nephrocalcinosis on radiographic or ultrasound examinations[11]. Nephrocalcinosis is a condition where calcium salts are deposited in renal tissue, and it may lead to critical kidney complications. In ERS patients, 2 patients were reported to have died before the age of 30 due to renal failure[10]. Acute or chronic pyelonephritis, urinary calculus, and chronic renal failure have been also reported. The medical management of renal disease depends on the stage of disease and clinical status of the patient. Management may include dietary modification or administration of sodium bicarbonate to reduce acidosis[26]. In this study, nephrocalcinosis was detected accidentally at age of 10. She was advised to increase daily fluid consumption and she is planned to have periodic renal examinations.
Pediatric dentists are the first oral health practitioners whom ERS patients will meet at early age. The role of pediatric dentists is critically important in early diagnosis and referral of patients to both nephrologists for renal assessment and geneticists for causative mutation. Early detection of renal involvement may provide chances to prevent further undesired renal complications.
Ⅳ. Summary
A 6-year-old girl was referred with a presumptive diagnosis of Amelogenesis imperfect (AI) and the process of growth, multiple unerupted teeth and nephrocalcinosis were detected.
Enamel Renal syndrome (ERS), a rare syndrome of AI associated with nephrocalcinosis, can be diagnosed based on multiple dental phenotypes in the absence of renal diagnosis, such as hypoplastic enamel, pathognomonic eruption failure of posterior teeth, hamartoma formation coronal to impacted teeth, gingival hyperplasia, intra-pulpal calcification, and calcification nodule in gingiva and follicle. When ERS is suspected, pediatric dentists should refer of patients to both nephrologists for renal assessment and geneticists for causative mutation.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






