



Ⅰ. Introduction
An impacted tooth is one that fails to erupt due to a certain physical barrier in the eruption path, leading to no emergence at ½ to ¾ of root formation[1]. It can be caused by systemic or local factors. Systemic factors include endocrine diseases and certain syndromes. Local factors include a mucosal barrier, lack of space, odontogenic tumors, odontoma, supernumerary teeth, and ectopic eruption[1].
A thorough evaluation including a detailed medical history, dental history, familial history, clinical inspection and radiographic examinations is essential to detect and treat impacted teeth[2,3]. A clinical examination should be carried out to determine the presence of a palatal or buccal bulge and availability of space for an unerupted tooth[4,5]. Diagnosis of impacted tooth and a determination of its location is performed through radiographic evaluation including panoramic radiograph and Cone-Beam Computed Tomography(CBCT)[4,5].
Treatment options for impacted teeth include periodic observation, removal of obstacles on eruption pathway, surgical exposure, orthodontic traction, and extraction depending on root development, the direction of eruption, depth of teeth, and position of the teeth[6]. If the eruption direction of the tooth is severely deviated from normal or if eruption is no longer expected after periodic observation, orthodontic traction can be performed[7].
Impacted teeth not only cause esthetic problems but also lead to functional problems. Orthodontic intervention to bring these impacted teeth to the line of occlusion is important for long-term function and stability.
Various methods have been used to guide the eruption of impacted teeth. Despite the use of removable appliances has been suggested in previous studies[8,9], it has several disadvantages including the need for patient cooperation and limited control of tooth movement[10].
This case report presents treatment procedures for impacted teeth using modified Nance appliance. It is a new type of fixed orthodontic appliance that facilitates convenient exchange of traction wires by attaching a bracket on the resin button of the Nance holding arch. An indication of the appliance is an impacted tooth in the maxillary arch. It is especially useful when a change of direction is required during traction. The traction wire for delivering force to impacted teeth can be changed without removal of the entire appliance[10].
Orthodontic traction using modified Nance appliance offers high advantages in terms of anchorage control and good periodontal results. Modified Nance appliance is an easy appliance for practitioners to use and highly tolerable by young patients. It is applicable to different areas within the maxillary arch.
This report presents three cases of impacted teeth that were treated with modified Nance appliance as well as a review of previous studies.
Ⅱ. Case Reports
1. Case Ⅰ
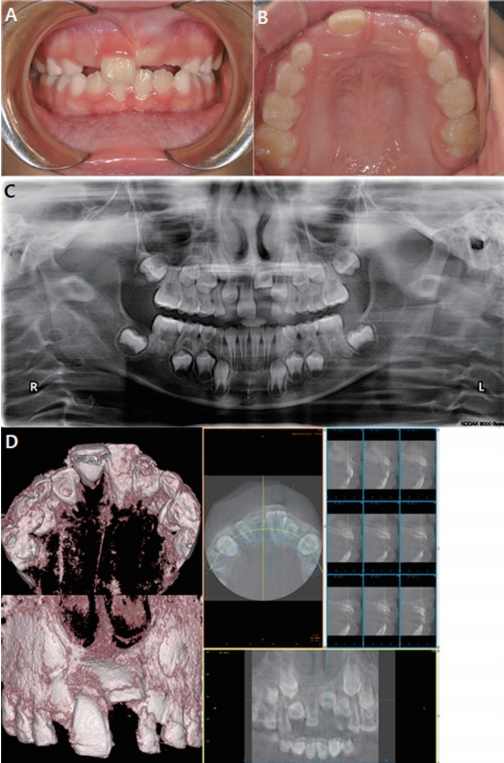
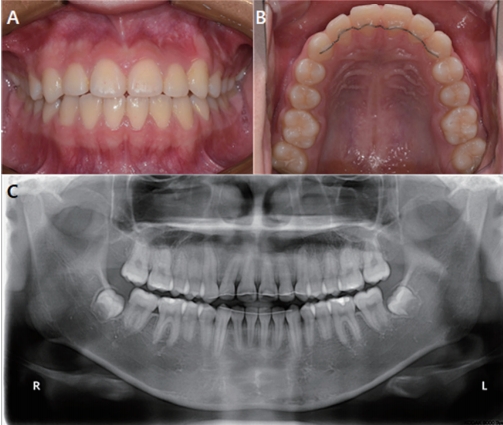
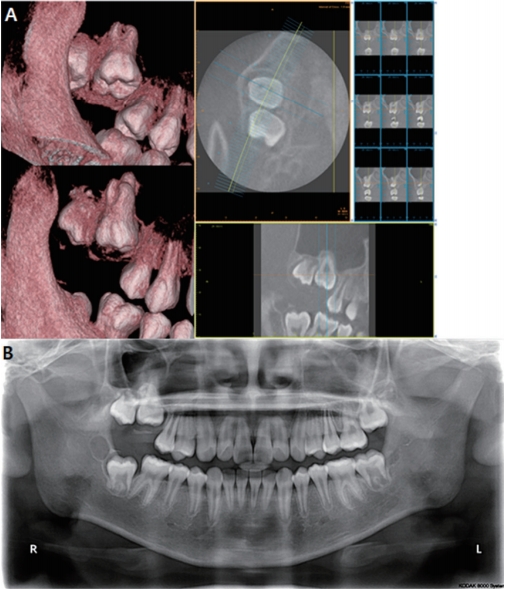
A 7-year-old girl was referred from a local clinic with chief complaint of a missing maxillary anterior tooth. The patient had no significant medical history. On intraoral examination, the maxillary left central incisor was detected on buccal mucosa above mucogingival junction(Fig. 1A, 1B). She presented Class I molar relationship bilaterally with normal overjet and overbite. On the panoramic radiograph(Fig. 1C) and CBCT images(Fig. 1D), horizontally impacted maxillary left central incisor was observed.
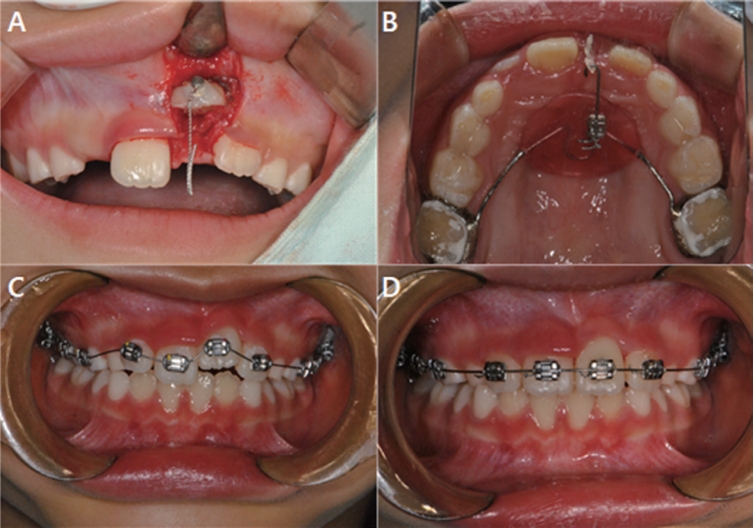
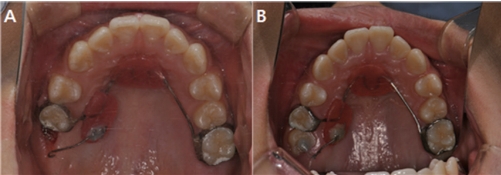
Closed eruption technique was performed. The crown of #21 was exposed and a button with ligature wire chain was bonded on the labial surface of the tooth(Fig. 2A). The flap was sutured back. A week later, the suture was removed and pickup impression for an orthodontic appliance was taken with alginate. A modified Nance appliance with bracket on its resin button was delivered in a week. A traction wire was fabricated with TMA wire and ligated to a bracket on the appliance(Fig. 2B). The ligature chain was placed on the terminal hook of traction wire for application of traction forces. Approximately 60 gm of force was applied. The patient was checked at monthly intervals to monitor the traction force and adjust the appliance. After 3 months, #21 emerged into the oral cavity.
The modified Nance appliance was removed and fixed orthodontic appliances were bonded on the maxillary arch for further alignment(Fig. 2C). Typical leveling and finishing procedures were continued(Fig. 2D). After 8 months, the brackets and bands were removed.
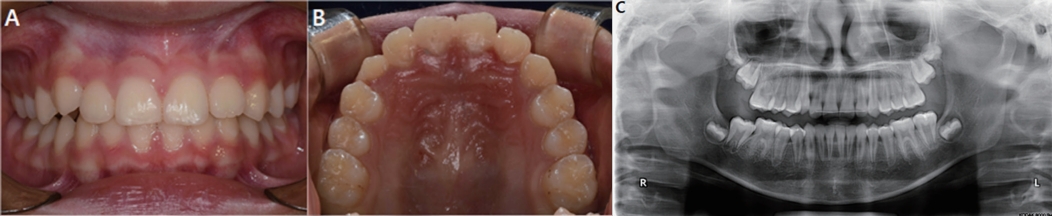
After 3 months of traction using the modified Nance appliance followed by 8 months of additional orthodontic procedures on the maxillary arch, the left maxillary incisor was positioned adequately in the dental arch(Fig. 3). A fixed retainer was bonded on the lingual side of the maxillary incisors.
22 months after debonding, the fixed retainer was removed. During 22 months of clinical and radiographic follow up, apical closure, bone level and attachment level were similar to those of the adjacent teeth(Fig. 4).
2. Case Ⅱ
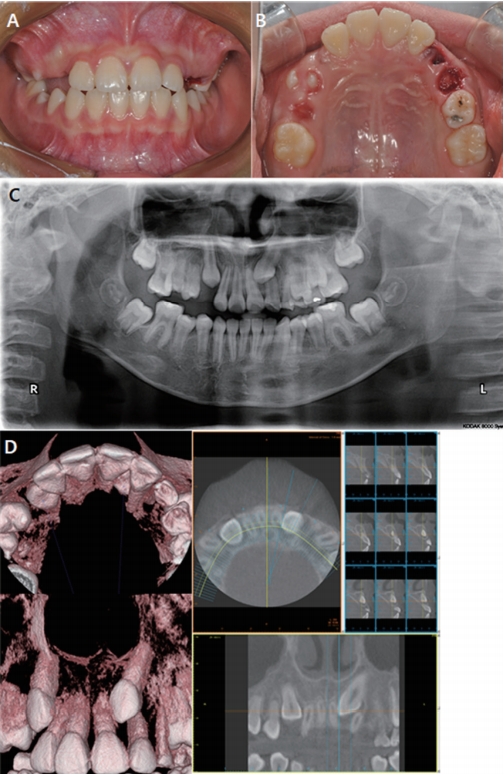
A 9-year-old girl was referred from a local clinic with chief complaint of an impacted permanent maxillary left canine. The patient had no significant medical history. An intraoral examination revealed retained deciduous maxillary left canine and a Class I molar relationship on both sides(Fig. 5A, 5B). A panoramic radiograph showed impaction of the permanent maxillary left canine which was superimposed with the root of the left lateral incisor(Fig. 5C). CBCT images revealed mesiobuccally impacted maxillary left canine and the crown of the tooth located between #21 and #22(Fig. 5D).
Surgical exposure and button attachment were performed with the same procedures as described above for Case 1(Fig. 6A). After 7 days, the suture was removed and pick-up impression was taken to fabricate an appliance.
A modified Nance appliance was delivered in a week. A traction wire to move the tooth to the distobuccal direction was made with TMA wire and ligated to the bracket on the appliance(Fig. 6B). Approximately 100 gm of force was applied to the tooth. The patient was admitted at monthly intervals to check the traction force and adjust the appliance. For the first 5 months of traction using modified Nance appliance, the tooth moved to distobuccal side.
An apically positioned flap was then performed so as to provide enough attached gingiva to the tooth(Fig. 6C). The modified Nance appliance was removed and fixed orthodontic appliances were bonded to the upper arch(Fig. 6D). Flexible NiTi wire was engaged to the upper arch. When #23 reached to occlusal level, fixed appliances were bonded and NiTi wire was engaged to the lower arch. As the treatment progressed, the NiTi wire was replaced with rectangular stainless steel wire(Fig. 6E). After 20 months, the brackets and bands were removed.
After 5 months of traction using modified Nance appliance followed by 20 months of second phase orthodontic procedures, treatment was completed. The left maxillary canine was positioned adequately in the dental arch with enough width of attached gingiva(Fig. 7). Fixed and removable retainers for upper and lower arch were delivered to the patient.
Over 8 months of clinical and radiographic follow up, its bone level and attachment level were similar to those of the adjacent teeth(Fig. 8).
3. Case Ⅲ
An 11-year-old boy was referred from a local clinic with chief complaint of an unerupted molar. The patient had no significant medical history. On the panoramic radiograph and CBCT images, the maxillary right first molar had not erupted(Fig. 9A, 9B).
The patient and his parents were fully informed and aware of the possibility of ankylosis and traction failure. Since they did not agree with the overall orthodontic treatment, the treatment objective was limited to traction of the impacted tooth.
Surgical exposure was performed with electrosurgery. The occlusal surface of #16 was uncovered and a button with a ligature wire chain was bonded on the surface. A modified Nance appliance was delivered in a week. Additional resin part was made on the right palate so that the bracket could be located close to the tooth while the resin button could be an additional anchorage(Fig. 10A). Approximately 60 gm of force was applied to the impacted tooth to occlusal direction.
3 months after traction with the appliance, the wire had to be replaced to change the direction and extent of force. A new traction wire for distobuccal movement of the tooth was ligated to the bracket on the button instead of removing the entire appliance. After 9 months of traction, the tooth was exposed into the oral cavity(Fig. 10B). After 11 months of traction, the appliance was removed. Second phase orthodontic treatment was not carried out. To allow spontaneous eruption of the tooth, a retainer was not fabricated.
Ⅲ. Discussion
Management of impacted teeth is important in terms of esthetics and function[11,12]. Several techniques have been used in the management of impacted teeth. According to previous studies, surgical exposure followed by orthodontic traction is a common treatment modality for impacted teeth[13,14]. In these cases, surgical exposure was used in combination with orthodontic traction using modified Nance appliance.
Nance appliance is a fixed type space maintainer for upper dental arch. It can be utilized in either a unilateral or bilateral loss of maxillary second primary molars or multiple molars[5]. In this study, it was used for space maintenance and anchorage reinforcement. It consists of bands cemented on molars with a connecting palatal arch made of 0.9 mm stainless steel wire and palatal button made of acrylic resin. Modified Nance appliance has a bracket embedded on the resin button of the Nance appliance. The bracket facilitates easier change of traction wire for changing the direction of force.
A traction wire made of TMA wire is ligated to the bracket for traction of tooth. The traction wire has a small hook at the terminal end for attachment of ligature ties. It can be adjusted three-dimensionally base on CBCT to the direction of desired movement.
The usage of TMA wire as a traction wire is suitable because it has good formability and flexibility. A light force can be applied to the tooth by utilizing the wire[15]. Light orthodontic forces, as used in the present cases, are beneficial to periodontal health since they can minimize the loss of alveolar bone support and potential injury to the tooth during traction[16].
When the impacted tooth is in normal direction, a traction force of approximately 50 gm is required to prevent root resorption and loss of vitality. A relatively large traction force of 100-150 gm is required when the tooth needs to be rotated[15,17]. This can be seen in the cases discussed. Approximately 60 gm of traction force was used in case 1 and 3, a relatively large traction force of 100 gm was used in case 2.
Using a modified Nance appliance provides great advantages to practitioners. While removable appliances requires adequate cooperation from patients, modified Nance appliance requires little cooperation from patients[18]. Hence it is a useful appliance for young patients who are not expected to have a high level of cooperation.
Modified Nance appliance with a bracket attachment reduces the hassle of removing the entire appliance to change the direction and extent of force[8]. In a previous study, Nance appliance with an extension arm embedded on the resin button was used to move impacted teeth[19]. In that case, to change the direction of movement, complete removal and reproduction of the appliance was needed. On the other hand, a bracket attached on modified Nance appliance enables replacing the traction wire to change the direction and extent of force[8]. In case 3, a new traction wire fabricated at chair side was replaced so as to change the direction of the force applied.
It provides proper anchorage due to the use of a Nance button and transpalatal arch wire. This enables to eliminate reactionary intrusive forces on adjacent teeth[10]. This is important in children with mixed dentition as there are not enough permanent anterior teeth for anchorage.
As can been seen in the 3 cases, this appliance is applicable to impacted tooth in various parts within the maxillary arch. When extra anchorage is needed, a resin button can be added as observed in case 3. This appliance can be utilized as an interim device for diagnostic purposes to determine the possibility of ankylosis[19].
The use of modified Nance appliance has advantages to the patients. This appliance enables easier oral hygiene management. Since the entire appliance is located on lingual side, it is esthetically superior than others such as removable appliances[19].
The limitation of using modified Nance appliance is that proper alignment and detailing may not be achieved through its single use. When the teeth are not well aligned, a second phase of treatment using fixed orthodontic appliances is required as been done in case 1 and 2. Furthermore, if expansion of the arch or space regaining is needed, using other appliances should be considered.
In these 3 cases, modified Nance appliance was successfully used for the orthodontic traction of impacted teeth in various position on upper dental arch with little complications.
Ⅳ. Summary
Orthodontic traction of impacted teeth was successfully performed using modified Nance appliance, requiring little cooperation from patients. Usage of the appliance enabled application of a light force in the dental arch. When using a modified Nance appliance, the entire appliance does not usually need to be removed to change the direction and extent of force. This appliance is applicable to impacted tooth in various parts within the maxillary arch. This appliance enables practitioners to achieve desired levels of biomechanical control.





 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






