



Ⅰ. Introduction
Resin-modified glass ionomer cement (RMGIC) is a dental restorative material composed of conventional glass ionomer cement (GIC), a photo-activated methacrylate and 2-HEMA or Bis-GMA[1]. RMGIC has a lower bonding strength than composite resin. RMGIC is one of the restorative materials of choice for dental caries in pediatric patients in the precooperative stage. RMGIC exhibits an excellent microbiological environment at subgingival margin compared to composite resin[2].
For successful adhesion of restorative materials, hemostatic agents are used to prevent blood contamination. Aluminum chloride (AlCl₃) is one of the most frequently used for bleeding control in the oral cavity[3,4]. The occurrence of systemic side effects with aluminum chloride hemostatic agent is less common[5]. Aluminum chloride hemostatic agent is often used in dental clinics at a concentration of are in 5 - 25% a pH of 0.7 - 3.0[4,6,7]. Aluminum chloride forms a barrier by reacting with blood proteins and arrests the bleeding from the vessels[8,9].
Several studies have reported that aluminum chloride hemostatic agents have an additional effect on dentin by removing the smear layer present on the dentinal walls following instrumentation and by changing the composition of the dentinal surface[6,10]. Previous studies conducted to investigate the bonding strength of resin restorative material contaminated by aluminum chloride hemostatic agent showed different results according to the use of acid etching and classification of adhesives. One of the studies reported that identified a significantly decreased bonding strength of resin in a group wherein the self-etching adhesive had acted as a hemostatic agent[11]. Another study confirmed the recovery of bonding strength after using self-etching adhesives followed by acid etching treatment with phosphoric acid[12]. The document regarding the effect on shear bond strength of dentin of primary teeth by aluminum chloride hemostatic agent is limited.
The purpose of this study was to analyze the effect of aluminum chloride hemostatic agent on the shear bond strength by of RMGIC to dentin of primary molar. Scanning electron microscopy (SEM) based image analysis and energy-dispersive X-ray spectroscopy (EDS) analysis were performed.
Ⅱ. Materials and Methods
This study was approved by the Institutional Review Board (IRB) of the Dankook University Dental Hospital (IRB NO: DKUDH IRB 2020-05-004).
1. Materials
Altogether, 36 non-carious primary molars were used in this study. The teeth were extracted within 4 months from pediatric patients who visited the Dankook University Dental Hospital. After extraction, the primary molars were immediately rinsed under running tap water and cleaned with a ultrasonic scaler. Primary molars were immersed in 1.23% thymol solution and stored in a refrigerator at 4.0℃ until used for the experiment. The specimens were randomly divided into 4 groups, with 15 specimens allocated to each group.
Ketac™ conditioner (ESPE, USA) containing polyacrylic acid (PAA) was used to remove the dentinal smear layer (Table 1). Hemodent® (Premier Product Co., Germany) was used as an aluminum chloride hemostatic agent. Fuji™ II LC capsule (A2 shade, GC Dental Co., Japan) was used as the restorative material, and it was light-cured with B&Lite S (B&L BIOTECH Inc., South Korea).
2. Methods
1) Fabrication of specimens
A mold was fabricated with a 3D printer using polylactic acid filament. The teeth were subsequently embedded in the mold and filled with self-curing acrylic resin. After 24 hours, the teeth were sectioned into the buccal and the lingual portions with a highly accurate cut-off machine (Accutom-50: Struers, Denmark, Fig. 1). To create homogeneous smear layer, the exposed dentin surface was thoroughly polished for 60 seconds with a polishing machine (J-POS2: JISICO, South Korea) and a 600 grit silicon carbide sandpaper under water coolant.
2) Dentin surface treatment and RMGIC restoration
In group I, the surface of each specimen was air-dried for 5 seconds. Onto the dried surface of the dentin, a Teflon mold with an internal diameter of 3.0 mm, the height of 2.0 mm was placed. The mold was restored with RMGIC, and light-cured for 20 seconds.
In group II, the surface of each specimen was air-dried for 5 seconds, and PAA was applied for 10 seconds. After washing with water for 5 seconds, the surface was air-dried for 10 seconds. Subsequently, RMGIC was applied and cured using the same method used for group I.
In group III, aluminum chloride hemostatic agent was applied for 1 minute. The application time of 1 minute was according to the manufacturer’s instructions. The surface was then washed for 10 seconds and air-dried for 5 seconds. RMGIC was cured with the same method used for group I.
Similarly, an aluminum chloride hemostatic agent was also used in group IV. Subsequently, PAA was applied for 10 seconds, washed with water for 10 seconds, and the surface was air-dried for 5 seconds. RMGIC was cured in the same method used for group I.
In all groups, PAA and hemostatic agent were applied onto all the surfaces of the teeth using a cotton pellet.
3) Thermocycling
All of the cured RMGIC specimens were subjected to thermocycling process between temperature of 5.0℃ and 55.0℃ for 5000 cycles with dwelling time of 30 seconds and transfer time of 5 seconds (Fig. 2).
4) Measurement of shear bond strength
A universal testing machine (Kyung-Sung Testing Machine Co., South Korea) was used to measure the shear bond strength (Fig. 3). Each specimen was tested in the machine under the condition of a 50.0 KgF load cell with a crosshead speed of 1.0 mm/min. The maximum value at the time when the RMGIC restoration detaches from the specimen was measured. Each measurement was divided by the base area of the restoration and converted into MPa.
5) SEM/EDS Analysis
Three specimens were used for SEM/EDS study of each group. Dentin was pre-treated in the same manner as described previously. The exposed dentinal surface was observed in SEM (Sigma 500 VP: Zeiss, Germany) at 5000 magnification. The surface of the specimen was analyzed using EDS (NORAN System 7: Thermo Fisher Scientific, USA) attached to SEM. Elements such as carbon, oxygen, aluminum, phosphorous, chlorine, and calcium were measured with EDS.
Ⅲ. Results
1. Shear bond strength
The mean and standard deviation of the shear bond strength of each group are presented (Table 2, 3). Group I that restored RMGIC without using hemostatic agent and PAA showed 4.04 ± 0.88 MPa of shear bond strength. Group II, which used only PAA without hemostatic agent showed 8.29 ± 1.40 MPa of shear bond strength, a higher value than group I. Group III, wherein only the hemostatic agent was used, a shear bond strength of 1.39 ± 0.47 MPa. This value was lower than that observed in group I. In group IV, where a hemostatic agent was used prior to applying PAA, the value of 6.24 ± 2.76 MPa appeared, which was a higher than group I but lower than group II. Significant differences were observed among the shear bond strengths of all groups.
2. SEM/EDS analysis
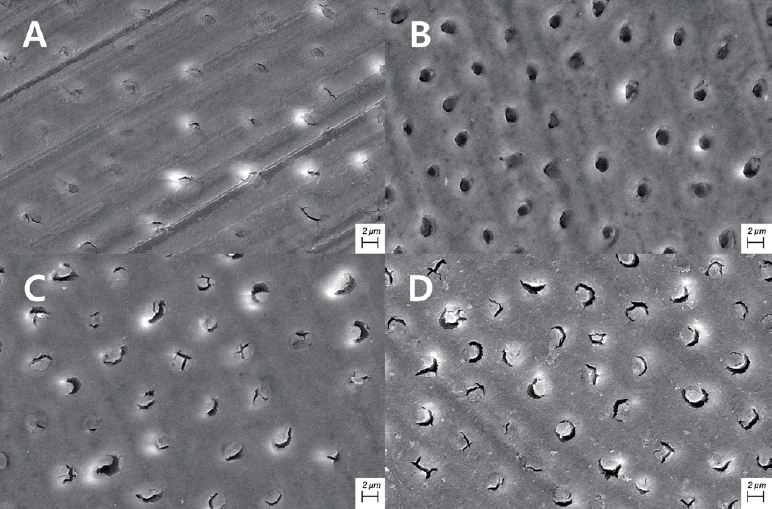
When the dentinal surface was examined using SEM, it was impossible to identify the shape of the dentinal tubules in group I, since the smear layer covered the dentinal surface (Fig 4). On the other hand, the round shape of the dentinal tubule was observable in group II, since the smear layer has been removed by the PAA. In group III, which used the aluminum chloride hemostatic agent, the opening of dentinal tubules was wider than group I, but the shape of the opening was not circular. Group IV is observed to have some smear layer removed from the surface compared to group I, and this pattern was similar to group III.
In the EDS analysis, aluminum was observed in groups III and IV that used the hemostatic agent (Table 4). It was not observed in groups I and II which did not use the hemostatic agent. The weight percentage of chlorine was higher in group III than in groups I, II and IV. The weight percentage of calcium was lower in groups III and IV than in group I.
Ⅳ. Discussion
The purpose of this study was to investigate the effect of contamination from aluminum chloride hemostatic agent on the shear bond strength of RMGIC to primary tooth dentin.
Many carious lesions are located near the subgingival margin. Contamination with blood and gingival crevicular fluid takes place near the subgingival margin. To prevent such deterioration, practitioners use the hemostatic agent during the restoration process to reduce the amount of gingival crevicular fluid and to control gingival bleeding[4]. Pediatric dentistry clinics use various hemostatic agents, including aluminum chloride, ferric sulfate, and epinephrine. Each hemostatic agents has a difference in mechanisms for hemostasis. Therefore, the appropriate hemostatic agent is selected for the location and situation of bleeding. The present experiment was performed using an aluminum chloride that acts by precipitating proteins on the superficial layer of mucosa and make it mechanically stronger.
RMGIC is a restorative material composed of GIC with resin components[1]. The mechanical properties such as tensile strength and compressive strength of RMGIC is equal to those of bond strength GIC. The bonding intensity of RMGIC depends on the ionic bond between hydroxyapatite (HA) of the tooth and restorative material[13]. Ionic bonding between tooth and material takes place by the acid-base reaction of calcium ions from HA present on the surface of the tooth and carboxyl ion from polyacids present in RMGIC components.
There are previous studies on the negative effects of hemostatic agents on the adhesion of composite resin. It has been reported that ferric sulfate hemostatic agents reduce the bonding strength of composite resin[12,14-17]. Prabhakar and Bedi[18] suggested that the reduction in shear bond strength may be associated with coagulation of plasma proteins in the dentinal fluid. Another previous studies report that aluminum chloride hemostatic agents have a negative effect on bonding strength of composite resin[10,12,14,15]. It was postulated that insoluble complex was responsible for the decrease in bonding strength on the composite resin which contaminated with aluminum chloride[19]. In the case of two hemostatic agents, some researchers report that the reduced bonding strength was recovered when using the total etching adhesive system[10-12,20]. In primary tooth, it also showed a tendency to decrease bonding strength due to hemostatic agents[16,18]. Our findings, using RMGIC, were in line with those of the previous studies which report the decrease in bonding strength after the application of hemostatic agents.
The micromechanical bonding of polymers that penetrate the dentinal tubules is important[21,22]. The polymer penetrating the dentinal tubules exposed after elimination of the smear layer enhances the micromechanical bonding strength by increasing the surface area. Elimination of the smear layer observed in the SEM after the use of aluminum chloride hemostatic agent was consistent with the previous study[6,23,24]. Land et al.[6] reported that the smear layers partially eliminated within 30 seconds to 5 minutes after the application of aluminum chloride hemostatic agent. The amount of smear layer elimination was increased by time. However, the openings of dentinal tubules were not fully exposed, and debris remained within the dentinal tubules.
In the present study, the shear bond strength of group III was significantly lower than that of group I. Hemostatic agent use may have contributed to the reduction in the bond strength between dentin and RMGIC. If the aluminum ion contained in the aluminum chloride hemostatic agent reacts with HA of the tooth surface, it is replaced by calcium ions of HA to form an insoluble complex, Al(OH)₂H₂PO₄[19]. Accordingly, it reduces the reactivity of the dentin surface and leads to decreased ionic bond with RMGIC.
According to Saad et al.[14], there was no significant difference in bond strength between a group involving RMGIC restoration wherein PAA was applied after contamination with an aluminum chloride hemostatic agent and a group involving RMGIC restoration wherein PAA was applied without the use of a hemostatic agent. However, it was significantly lower than the group that only applied PAA without hemostatic agent. Such difference in results seems to be due to the differences in constituents of the material and type of the teeth used in the study.
As a result of EDS analysis, aluminum was identified in groups III and IV which was not present in groups I and II. Groups III and IV showed the similar weight percentage of aluminum. Weight percentage of chlorine in group III was higher than in groups I, II and III. This indicates that the application of PAA has reduced the weight percentage of chlorine on the tooth surface, whereas the effect was minimal in the case of aluminum. This result is consistent with those of the previous studies. This was associated with reduced calcium after using a hemostatic agent and is assumed to be the result of complex formation.
Application of 37% phosphoric acid following the use of aluminum chloride hemostatic agent can effectively eliminate some of the remaining smear layers due to acid corrosion. And the openings of the dentinal tubules were observed more clearly following its application[11,24]. In addition, one study using ethylene diamine tetraacetic acid reports that the bonding strength was restored[10]. But, many studies that used PAA following the use of aluminum chloride hemostatic agent reported that this protocol was inadequate to effectively remove the debris remaining within the dentinal tubules[14,23]. The findings from the previous studies are consistent with the SEM results from the present study.
In this study, the experiment was conducted to verify alterations in tooth surface and reduction in the bond strength by a hemostatic agent. One previous study on this reduction suggests cutting off the portion of surface dentin that was exposed to the hemostatic agent[25]. Additional studies need to be conducted to explore ways to recover the bond strength of dentin contaminated with aluminum chloride as much as that of the uncontaminated surface during the process of bonding RMGIC.
The present study examined the influence of aluminum chloride. In addition to aluminum chlorides, a variety of hemostatic agents such as ferric sulfate are used in pediatric dental clinics. Further studies are required to compare and analyze the effects of those various hemostatic agents on bonding strength between RMGIC and dentin of primary teeth.
Since there are restoration cases using RMGIC for permanent tooth in the department of pediatric dentistry such as amelogenesis imperfecta cases and erupting tooth, a study investigating the effect of aluminum chloride hemostatic agent on permanent dentin is also required.
Ⅴ. Conclusion
The shear bond strength of RMGIC significantly decreased when aluminum chloride hemostatic agent was applied for 1 minute regardless of the use of PAA in dentin of primary molar. The findings of SEM imaging showed that some of the smear layers were removed when aluminum chloride hemostatic agent was applied to dentin. Also, when the aluminum chloride hemostatic agent was applied, the increased weight percentage of chlorine declined with PAA application, while the measurement of aluminum did not. The calcium measurement dropped after applying the aluminum chloride hemostatic agent. The application of an aluminum chloride hemostatic agent to the exposed surface of dentin should be avoided to prevent the reduction of shear bonding strength during the restoration of RMGIC on dentin of primary molar.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






