



ŌģĀ. Introduction
Oral mucocele is a common exophytic lesion caused by the accumulation of saliva due to pathological changes in minor salivary glands[1]. It is typically asymptomatic and painless and characterized by the presence of a semipermeable fluctuant nodule[2]. Oral mucocele is frequently observed in teenagers and commonly occurs on the lower lip[3-5].
Oral mucoceles are histologically classified into two types: extravasation and retention[6,7]. Extravasation-type mucoceles are caused by traumatic damage to the excretory duct of the minor salivary glands those results in the extravasation of saliva into the surrounding connective tissue[6,7]. It is prevalent in the minor salivary glands of the lower lip[6,7]. On the other hand, retention-type mucoceles are caused by the obstruction of the salivary gland ducts, such as due to the presence of a sialolith[6,7].
The treatment method does not differ according to the type of mucocele and generally includes surgical excision, marsupialization, cryosurgery, and laser ablation[1]. Surgical resection, one of the traditional treatment methods, involves removing the surrounding mucosa and muscle layer below the salivary gland tissue[8]. This method requires special care to prevent the rupture of the mucosa during treatment, and recurrence may occur if the affected minor salivary gland is incompletely removed[8]. Invasive treatment methods are generally associated with bleeding, pain, and local anesthesia and are difficult to perform in infants and uncooperative young children[8].
Micro-marsupialization and tying have been introduced as alternative methods that can be used once a diagnosis of mucocele is made from the clinical examinations[9,10]. Micro-marsupialization, introduced by Morton and Barley[9] in 1995, involves the suturing of the oral mucosa, draining of the saliva inside the ranula between the suture and mucosa, and creation of a new epithelized tract along the path of the suture. Morton and Barley[9] reported the successful treatment of patients with oral ranulas and mucoceles using this method. The tying method, introduced by Itro et al.[10] in 1999, involves the removal of the lesion by tying its base with a surgical suture to block the blood supply, thereby resulting in necrosis. Using this method, the authors reported no recurrence 6 months after the removal of a ranula on the floor of the mouth[10].
The disadvantage of micro-marsupialization and the tying method is that it is impossible to reach a final diagnosis through histological examinations[11]. The main advantages of these methods are ease of performance, particularly in very young children, and the short duration of the treatment[12,13]. Several case reports have been published on the use of noninvasive treatment methods for oral mucoceles, but there is a lack of studies on the general method of application.
This case report presents the favorable results of four pediatric patients who received oral mucocele treatment using micro-marsupialization and tying method as part of minimally invasive techniques.
ŌģĪ. Case Reports
This study was conducted under the approval of the Biomedical Research Ethics Review Committee of Kyungpook National University Dental Hospital(IRB No: KNUDH-2021-07-05-00).
1. Case 1
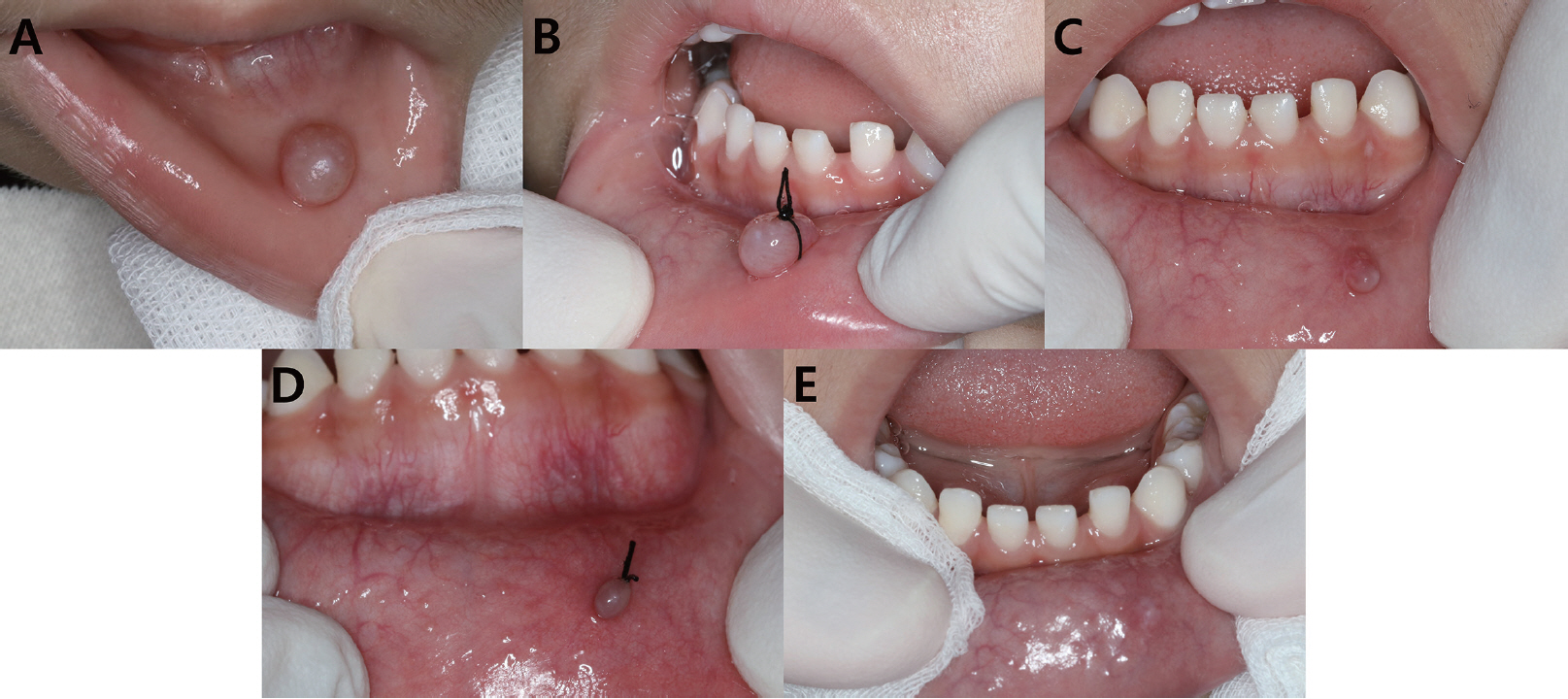
A 5-year-and-5-month-old boy visited the hospital with a blister on the lower lip that had occurred 1 year previously. Clinical examination revealed an exophytic lesion with a narrow peduncle (diameter 7.0 mm ├Ś 5.0 mm) and pink hue(Fig. 1A). The patient had no history of trauma to the oral cavity but had a habit of biting the lips. The patientŌĆÖs guardian confirmed that the size of the lesion continued to grow larger than that at the onset via a cycle of rupture, collapse, and refilling.
The lesion was tentatively diagnosed as an extravasation-type mucocele. Accordingly, various treatment methods, including surgical removal, were explained to the guardian, and consent was obtained to implement the tying method.
20% benzocaine topical anaesthetic gel (Ultracare®, Ultradent, South Jordan, USA) was applied, and the base of the lesion was tied using a 3-0 suture(Fig. 1B). Except for a slight agitation in the patient, there was no difficulty in the treatment when tying the base of the lesion. At the 1-week follow-up, the lesion site was spontaneously eliminated, and no remaining lesions or scar tissues were visible(Fig. 1C). The lesion healed favorably without surgical scars and was well maintained without recurrence until now, 3 years after the operation.
2. Case 2
A 3-year-and-1-month-old boy visited the hospital with a blister on the lower lip. The patientŌĆÖs guardian confirmed that the lesion had occurred 3 months prior, and the size had recently increased significantly because of the rupture-refilling cycle. Clinical examination revealed a wide base with a diameter of about 7.0 mm ├Ś 7.0 mm with an undercut, which is unlike the general shape of the round, semicircle mucocele(Fig. 2A). The patient had no history of trauma to the oral cavity but had a habit of sucking the fingers during sleep.
Based on the characteristics of the lesion and the childŌĆÖs oral habits, a tentative diagnosis was reached as an extravasation-type mucocele. Informed consent was obtained to treat the patient using a minimally invasive method based on the patientŌĆÖs age and behavioral problems. Because the lesion was large and had a wide base, micro-marsupialization was planned to reduce the size and followed by the tying method.
Topical anesthesia was applied and a 3-0 suture was passed through the most abundant central part of the lesion to form a discharge passage(Fig. 2B). During ligation, the lesion was compressed to confirm that the releasing pathway of saliva was properly formed. At the 1-week follow-up, the size of the lesion was considerably smaller and its base was exposed(Fig. 2C). The ligation was removed and the tying method was performed(Fig. 2D).
One week later, the lesion site was healed without any surgical scars, and no recurrence was observed until now, 6 months after the operation(Fig. 2E).
3. Case 3
A 5-year-and-6-month-old girl visited the hospital with a cyst on the right lower lip. On clinical examination, we observed a lesion with a wide base of approximately 4.0 mm ├Ś 4.0 mm in diameter(Fig. 3A). Using a questionnaire, we confirmed that the patient did not have any history of trauma and had a sucking habit at the time of eating.
The patient was tentatively diagnosed as an extravasation mucocele caused by continuous irritation. Considering the guardianŌĆÖs request for the use of nonsurgical methods and the type of mucocele, the micro-marsupialization method was selected.
Treatment was performed by placing a 3-0 silk suture through the center of the lesion under topical anesthesia(Fig. 3B). Binding included part of normal tissue and mucocele lesion for the retention of the suture. The silk thread fell out once, but 10 days after religation of the suture, saliva was discharged from the lesion, and the size of the lesion was reduced. One month later, a small amount of residue was observed around the suture. The saliva was completely discharged, and the lesion had regressed completely(Fig. 3C). The ligation removal was performed. No recurrence was reported at the 3-month follow-up(Fig. 3D).
4. Case 4
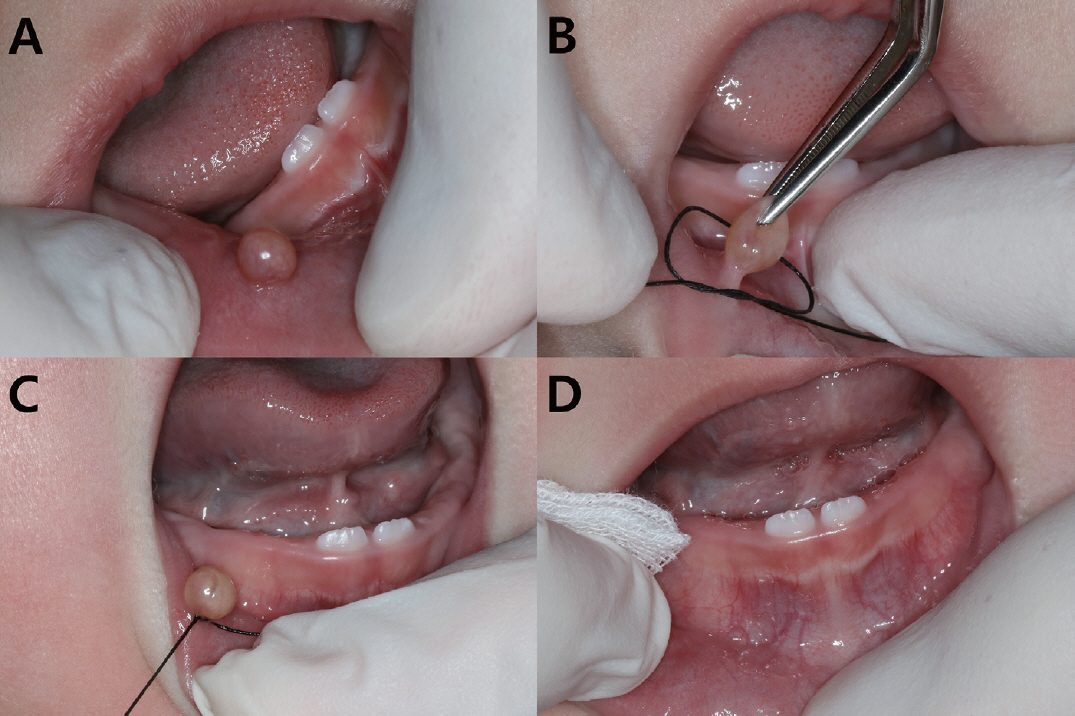
A 9-month-old girl visited the hospital with a blister on her right lower lip. On clinical examination, we observed a mucocele in the form of a round lesion (diameter 5.0 mm ├Ś 5.0 mm) with a narrow nodular base on the right side of the lower lip(Fig. 4A). The patient had no history of trauma, and it was confirmed that the child had a habit of sucking the thumb.
The patient was tentatively diagnosed with an extravasation-type mucocele. After explaining the various treatment methods, including surgical treatment, to the guardian, consent was obtained to implement the tying method.
After topical anesthesia application, the base of the lesion was tied using a 3-0 silk suture(Fig. 4B, 4C). The base of the mucocele lesion was exposed by an assistant lifting the lesion with a pincette(Fig. 4B). The guardian was cautioned not to allow the patient to touch the treatment site. The lesion had regressed by the 1-week follow-up(Fig. 4D). The guardian confirmed that the spontaneous removal occurred approximately 4 to 5 days after the treatment. There were no remaining lesions or scar tissues. There was no recurrence until 1 year after the treatment.
Ōģó. Discussion
A mucocele is the most common benign minor salivary gland disease and the second most common benign soft-tissue lesion in the oral cavity, second to traumatic fibroma[8,14]. It commonly presents as a painless, blue-toned, fluctuant lesion[15]. The initial lesion exhibits bullous edema and gradually increases in size until it bursts on its own; the mucus is discharged, and the mucocele is refilled with mucous fluid[15]. As this rupture-refilling cycle is repeated, the lesion continues to grow larger due to fibrosis and becomes nodular[15].
Oral mucocele is most common in teenagers[3-5] and is related to the parafunctional oral habits in children and adolescents[16]. According to previous studies, cheek- and lip-biting habits in children and adolescents were the most frequent causes of mucoceles in the United States[16]. Lesions occurred with the highest frequency in the lower lip. The lower lip is the most vulnerable to trauma, both functionally and nonfunctionally, because it is a part of the oral cavity that moves actively during masticating and speaking[17]. One study using magnetic resonance imaging showed that both men and women have a wider distribution of minor salivary glands in the lower lip than in the upper lip[18]. The presence of a large number of minor salivary glands in the lower lip might be associated with the high frequency of mucoceles that occurs in this region[19].
Histologically, oral mucoceles are classified into two types: the relatively more common extravasation type and retention type[6,7]. An extravasation-type mucocele which is relatively common in children is primarily caused by oral habits, such as lip biting, and occurs mostly in the minor salivary glands of the lower lip[6,7]. On the other hand, a retention-type mucocele is caused by the obstruction of the salivary glands, and the major salivary glands are often involved[6,7]. It is primarily found in adults[6,7]. Mucoceles can be classified into three categories based on the depth of distribution[20]. If the lesion is located directly below the mucosa, it is classified as a superficial mucocele; if it is located in the upper submucosa, it is classified as a classic mucocele; and if it is located on the lower dermis, it is classified as a deep mucocele[20].
In the case of the four patients in this study, after considering various factors such as the clinical features of the lesion, oral habits of the patient, and site of the mucocele, the lesions were tentatively diagnosed with extravasation-type mucocele caused by the damage to the minor salivary gland duct. The general treatment methods for mucocele include surgical excision, marsupialization, cryosurgery, and laser ablation[1]. Considering the ages of the patients in this study, it would have been difficult to use the surgical approach. Minimally invasive methods, such as micro-marsupialization and the tying method were selected. There was no difficulty in controlling the behavior of the children during treatment except for a slight agitation. Antibiotics were not prescribed because there was no possibility of bleeding or secondary infection. The mucoceles were successfully removed, and favorable results were obtained, without recurrence.
Micro-marsupialization involves the formation of a surgical ligation using surgical sutures after topical anesthesia is applied to the area[9]. The lesion is removed by inducing the formation of an epithelial tube between the superficial and salivary gland tissues below[12,13]. Ligation may become loose after 2 or 3 days and in such case, the treatment should be repeated[9]. Silk sutures may cause inflammation after 7 days due to surgical stimulation and accumulation of debris around the ligature[21,22]. Sandrini et al.[23] suggested that ligation should be maintained for 30 days. Further studies have shown that maintaining sutures for a long period in children can lead to discomfort and infection, which may cause recurrence due to incomplete epithelization of the suture tracts[24].
According to a study conducted by Sagari et al.[25], a success rate of 87.5% was observed in eight patients treated by micro-marsupialization. In the study by Delbem et al.[12], 14 pediatric patients were treated with a success rate of 85%. Itro et al.[10] introduced the tying method to remove a ranula on the floor of the mouth and reported no recurrence at the 6-month follow-up. Similarly, Lee et al.[26] also reported that following the successful removal of an oral mucocele on the lower lip of a 1-year-old girl using the tying method, recurrence was not observed at the 6-month follow-up.
As described above, micro-marsupialization and the tying method can be performed using topical anesthesia[12]. In addition, there is no bleeding during the procedure, no tissue damage, and no inflammatory reaction, and the healing period is short[12]. Children who have difficulty adjusting to long and invasive procedures will be more likely to accept and cooperate with these minimally invasive methods[12,13].
After surgical resection of the mucocele, it is desirable to perform histological examination. Minimally invasive treatments can be performed in uncooperative patients and in cases in whom it is possible to diagnose the mucocele based on its clinical presentation. In addition, when selecting a minimally invasive treatment method, micro-marsupialization using sutures is recommended in the case of large-sized or dome-shaped mucoceles with wide bases and decreased heights that are located deep in the mucosa. The use of the tying method is recommended cases of superficial and pedunculated mucoceles with narrow bases and increased heights.
Despite the various advantages of a minimally invasive method, one disadvantage is that it is impossible to accurately diagnose the lesion with a biopsy after treatment[11]. In this case, fine-needle aspiration cytology, one of the pathological diagnostic methods for exophytic lesions in the oral cavity, can be used[27]. Because of the minimally invasive nature of this method, it is possible to histologically diagnose the lesion with the cooperation of the child patient[27]. Because of the lack of information on the use of minimally invasive treatment methods with sutures, a comparison of the recurrence rates is not yet feasible. More studies are needed to further understand and compare the benefits of this method.
ŌģŻ. Summary
It is difficult to treat young infants and children with behavioral problems with mucoceles using traditional methods. In such instances, micro-marsupialization or the tying method might prove to be more advantageous because of their ease of performance and patient acceptance. Within the limit of this study, this case report provides a possibility that micro-marsupialization and the tying method may be considered as alternative methods for the treatment of oral mucoceles in pediatric patients, particularly those with behavioral problems.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






