영유아기 과잉치의 임상적 처치 및 micro-computed tomography 분석: 증례 보고
Clinical Management and Micro-Computed Tomography Analysis of Supernumerary Teeth in Infancy: A Case Report
Article information

Abstract
과잉치는 치판의 과도한 성장과 분화에 의해서 발생된다. 이로 인해 이소맹출, 맹출지연, 인접치의 치근 흡수, 그리고 치간이개 등의 문제가 발생할 수 있다. 영유아기에서의 과잉치는 드물며 국내에서는 거의 보고되지 않았다. 이 증례에서는 3개의 매복된 과잉치가 있는 생후 2일된 신생아에 대해 보고하고 있으며, 환자는 21개월간 추적 관찰되었다. 유치열기에 맹출된 하나의 과잉치는 14개월이 되었을 때 중등도 진정 하에 발치되었다. 발치된 과잉치에 대해 micro-computed tomography (CT) 분석을 진행하여 치근단 부위의 미세한 형태 이상을 확인하였다. 과잉치 발치 후 치간이개는 감소하였고 구강위생도 개선되었다. 조기 진단 및 치료를 통해 과잉치로 인한 합병증을 예방할 수 있다.
Trans Abstract
Supernumerary teeth develop from excessive proliferation and development of the dental lamina. Supernumerary teeth can cause several problems, including ectopic eruption, delayed eruption, root resorption of adjacent teeth, and diastema. Supernumerary teeth in infancy are rare and have rarely been reported. Case of a 2-day-old infant with 3 supernumerary teeth is presented here and the patient was followed up for 21 months. The erupted supernumerary tooth in the primary dentition was extracted under moderate sedation at the age of 14 months. Microcomputed tomography analysis of the extracted tooth confirmed microscopic root malformation. After extraction, the midline diastema was reduced and oral hygiene improved. Early diagnosis and prompt treatment can prevent complications of supernumerary teeth.
Introduction
Teeth that grow in addition to normal dentition are termed supernumerary teeth [1]. Although the etiology of supernumerary teeth is unclear, it is thought to occur owing to hyperactivity of the dental lamina at the onset of tooth formation [2,3]. Supernumerary teeth occur twice as often in men than in women with permanent dentition. In primary dentition, no significant difference between the sexes is observed [4]. Supernumerary teeth occur more commonly in the maxilla than in the mandible [5]. In primary and permanent dentitions, the prevalence of supernumerary teeth is 0.03 - 1.9% and 0.1 - 3.8%, respectively [6]. The reason for the low prevalence of supernumerary teeth in primary dentition may be that most children visit the dental clinic for the first time in the early stages of mixed dentition; therefore, impacted supernumerary teeth commonly go unrecognized [7].
Most supernumerary teeth are impacted and have no symptoms; therefore, radiography is essential for diagnosis [8]. Since children may not cooperate with radiographic examinations, most of the published cases were observed in mixed or permanent dentition [9]. Supernumerary teeth detected in the early stages of childhood development, such as the neonatal period or infancy, are extremely rare, except for erupted natal and neonatal teeth [10]. This case report describes the differential diagnosis of supernumerary teeth during the neonatal period and infancy when a developmental cyst is often suspected. This report also presents the clinical management of an erupted supernumerary tooth in the maxillary anterior region of the primary dentition, with succedaneous supernumerary teeth during the neonatal period, infancy, and early childhood. Furthermore, observation of a supplemental supernumerary tooth with root anomalies in the primary dentition using microcomputed tomography (CT) analysis is also presented.
Case Report
A 2-day-old male infant was referred from the pediatrics department of Wonju Severance Christian Hospital owing to swelling and a gum nodule-like lesion at the middle of the anterior maxillary alveolus (Fig. 1A). Clinically, the lesion was swollen and white. On the anteroposterior skull (AP skull) radiograph taken in advance at the pediatrics department, radiopaque masses were observed in the anterior maxilla area (Fig. 2). The patient had no relevant medical or family history, and results of newborn screening test was also normal. As the patient was too young to differentiate supernumerary teeth from normal dentition, a follow-up of the lesion was planned at the department of pediatric dentistry.
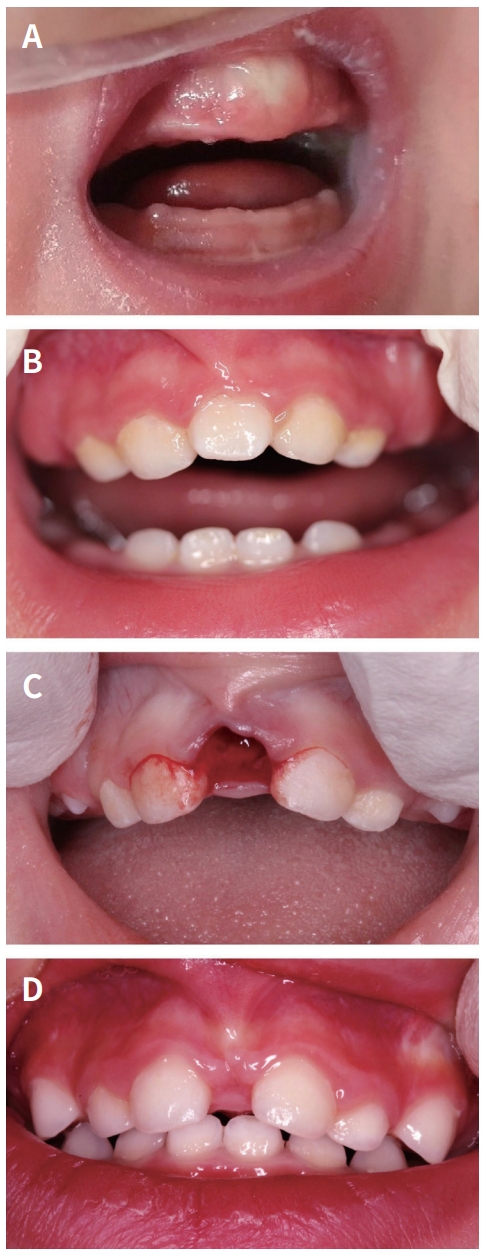
Clinical intra-oral photographs of patient. (A) Maxillary alveolar swelling at the age of 2 days, (B) An eruption of a supplemental supernumerary tooth at the age of 13 months, (C) After extraction of supernumerary tooth at the age of 14 months, (D) Normal healing 4 months post-operatively.

Anteroposterior skull radiograph taken at the pediatric department showing radiopaque masses in the maxillary anterior region.
At 8 months of age, he revisited our hospital with the chief complaint of delayed eruption of the maxillary central deciduous incisors. A periapical radiograph revealed three impacted supernumerary teeth (Fig. 3A), one of which was vertically impacted between the impacted maxillary central deciduous incisors. The remaining two were impacted above the maxillary central deciduous incisors, and the one on the left was inverted. Considering the tooth location, development of adjacent teeth, patient’s age, and ability to cooperate, the supernumerary tooth between the maxillary central deciduous incisors was decided to extract under moderate sedation following tooth eruption.
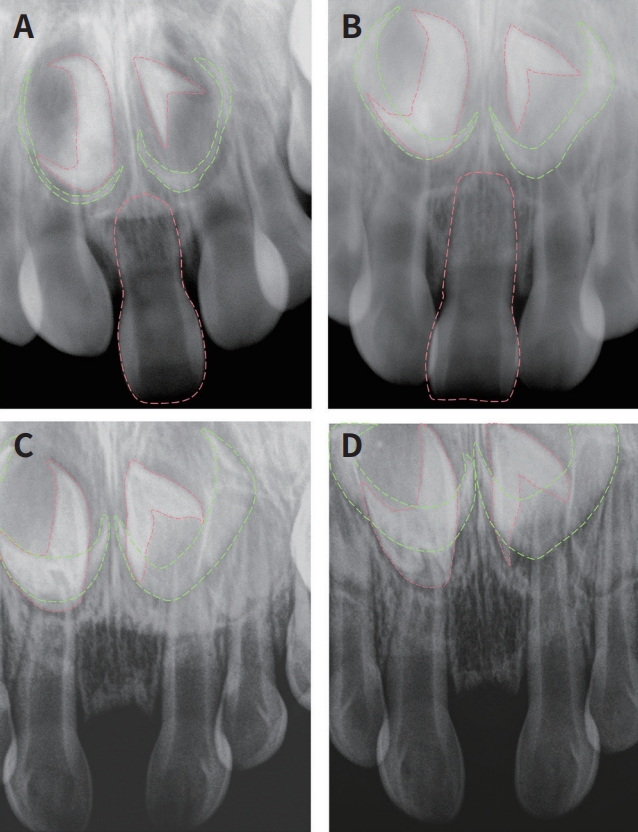
Periapical radiographs of patient. (A) The deciduous supernumerary tooth, two succedaneous supernumerary tooth buds (red dot line) and two tooth buds of the permanent incisor (green dot line) in the maxillary anterior region at the ages of 8 months, (B) At the ages of 13 months, (C) At the ages of 16 months (1 month post-operation), (D) At the ages of 20 months (4 months post-operation).
The parents confirmed the eruption of the supernumerary tooth and two maxillary central incisors at 10 months of age. The erupted supernumerary tooth was morphologically similar to the normal maxillary central deciduous incisors at the age of 13 months (Fig. 1B). At 14 months of age, simple extraction of the erupted supernumerary tooth was performed under moderate sedation and local anesthesia (Fig. 1C). The extracted tooth was 16 mm long, and its shape was very similar to that of the normal maxillary central deciduous incisor (Fig. 4). Four months after the extraction, the midline diastema was reduced but not completely resolved (Fig. 1D). As the parents did not opt to treat the diastema, observation without further treatment was planned. Surgical extraction of the impacted supernumerary teeth was planned as appropriate during the follow-up.

Photographs of the extracted supernumerary tooth. The morphology is similar to a normal deciduous central incisor.
The root shape anomaly of the extracted supernumerary tooth was detected using a high-resolution micro-CT scanner (SkyScan 1176, Bruker-microCT, Kontich, Belgium) with an X-ray source of 90 kV, 278 μA, 780 ms/frame exposure, and a 0.5 mm thick aluminum filter (Fig. 5A - 5C). The voxel size of the resulting image was 8.84 μm, and the mean scanning time was 40 min. The NRecon software (ver.1.6.9.3, Brucker micro-CT) was used to reconstruct 2-dimensional cross-sectional grayscale image slices (1804 pixels × 1452 pixels). Sectional images of the sagittal, axial, and coronal planes were acquired by aligning the reconstructed images using Data Viewer software (ver.1.5.1.2, Brucker micro-CT). Pseudo-color images of the targeted sectional images were obtained using CT-analyzer software (ver.1.14.4.1, Brucker micro-CT) according to the grayscale intensity (Fig. 5D).
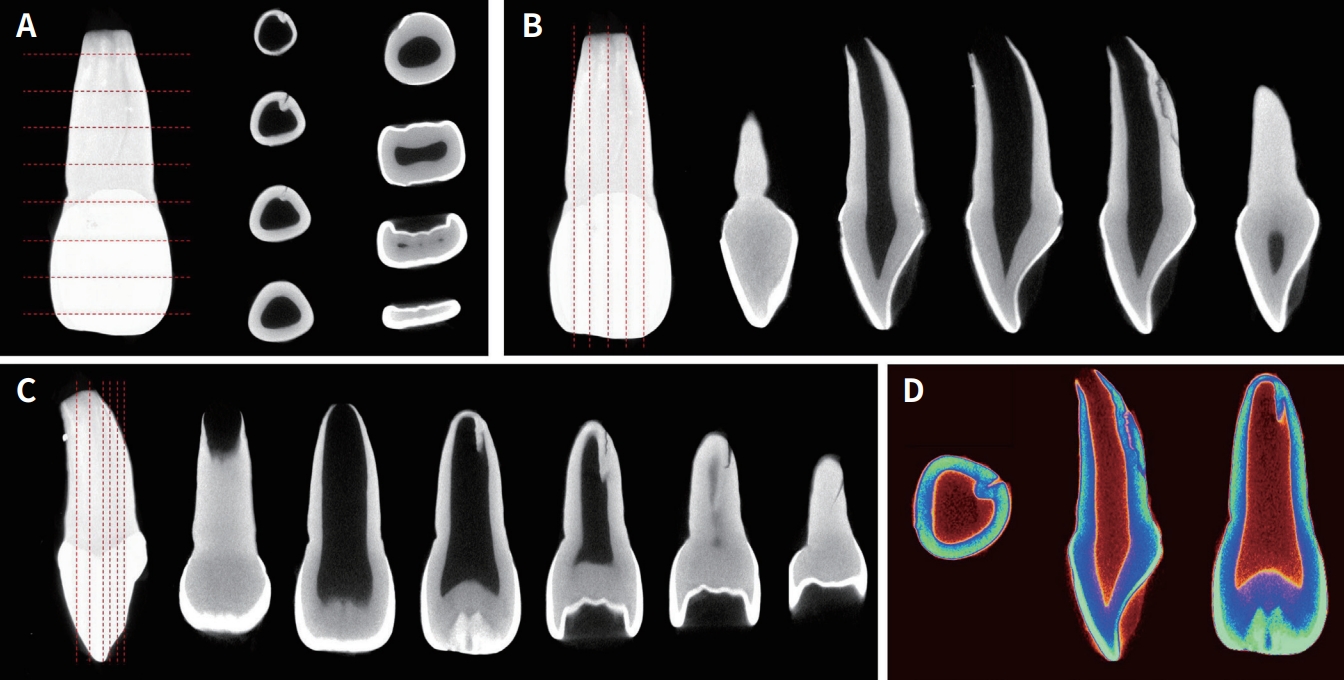
Micro-computed tomography of the extracted supernumerary tooth. (A) Horizontal sectional image, (B) Sagittal sectional images, (C) Coronal sectional images, (D) Pseudo-color images.
Discussion
The growth and development stages of a child can be classified based on the period showing relatively distinct characteristics. This is classified as a neonatal period of up to the ages of 4 weeks, 1 month - 1 year for infancy, 1 - 6 years for early childhood, 6 - 12 years for late childhood, and 12 - 18 years for adolescence [11]. Natal teeth that have already erupted at birth or neonatal teeth erupting within a neonatal period are easy to check because they can be seen with the naked eye. Unlike natal or neonatal teeth, the early detection of impacted supernumerary teeth is not simple without radiography. In this case, a supernumerary tooth was suspected on an AP skull radiograph taken at the pediatric department immediately after birth. Over-exposure parameters or inadequate movement of child patient during skull radiography may increase the risk of cancer and affect cognitive abilities in adulthood [12,13]. In pediatric dentistry, considering the radiation dose and cooperation of the patient, it is recommended to use a size 0 intraoral film for patients under 3 years of age with the help of their parents [14]. Considering the cooperation level of the patient and to minimize the radiation dose, additional radiography was not immediately performed. A periapical radiograph was obtained at 8 months of age to check for the development of a supernumerary tooth, and two impacted supernumerary teeth were additionally confirmed.
Supernumerary teeth were classified according to their morphology, location, and number [15]. The morphology of supernumerary teeth in the primary dentition is usually conical or normal [16]. In contrast, this number can vary in permanent dentition [17]. Mitchell [18] classified supernumerary teeth according to morphology (supplemental, conical, tuberculate, and odontoma) and location (mesiodens, paramolar, and distomolar). The conical type is peg-shaped and most commonly found in permanent dentition. The tuberculate type has one or more cusps/tubercles and may be invaginated. The supplemental supernumerary teeth were similar to normal teeth. Odontoma is the fourth type of supernumerary tooth [17]. The mesiodens is located in the maxillary midline and is usually conical. The paramolars are usually located buccal/palatal to the maxillary molar and are often small and rudimentary [19]. The distomolars are located distal to the third molar [20].
Postulations regarding the reasons for the formation of supernumerary teeth include atavism, tooth germ dichotomy, dental lamina hyperactivity, and genetic and environmental factors. Atavism theory states that the trait of a multi-toothed species was lost during evolution but remains genetically re-emerging in some patients. The dichotomy theory states that a single-tooth germ is divided into two tooth germs, one of which becomes a supernumerary tooth. According to this theory, the divided tooth germ grows into a normal tooth if it has the same size as the other part and into a dysmorphic tooth if it has a different size [21]. The hyperactivity theory of the dental lamina is widely accepted [22]. This theory explains that the development of supernumerary teeth results from the localized, independent, and conditioned hyperactivity of the dental lamina. In the supplemental form, additional tooth buds extend to the lingual area to form supernumerary teeth. The rudimentary form, which includes conical and tuberculate forms, originates from the over-proliferation of the dental lamina epithelial cells [3,21,23]. Therefore, similar to the present case, supplemental supernumerary teeth develop concurrently with the adjacent normal dentition.
Individuals without syndromes rarely have multiple supernumerary teeth. Syndromes associated with multiple supernumerary teeth include Ehlers-Danlos syndrome, Fabry-Anderson syndrome, Gardner’s syndrome, and labial palatal cleft or cleidocranial dysplasia [24,25]. Non-syndrome multiple supernumerary teeth describe multiple supernumerary teeth without systemic disease or syndrome [22], the prevalence of which is < 1% [3,26]. In the present case, three supernumerary teeth were present, with the patient having normal newborn screening test results and no history of systemic illness or syndrome. Multiple non-syndromic supernumerary teeth usually occur in the premolar area of the mandible [27]. In contrast, in the present case, three supernumerary teeth were observed in the maxillary anterior area.
Succedaneous supernumerary teeth can occur below the primary supernumerary teeth [28,29]. The incidence of succedaneous supernumerary teeth in patients with primary supernumerary teeth is 30 - 63% [29]. Taylor [30] found 18 primary supernumerary teeth in 11 patients, 17 of which presented with succedaneous supernumerary teeth, of which 13 were of the supplemental type. He explained that the extra tooth germ arises directly from the dental lamina, developing a successional tooth in the lingual area of the primary supplemental enamel organ. In this case, two successive supernumerary teeth with a suspected talon cusp were impacted below the primary supernumerary tooth.
In the primary dentition, a conservative approach is recommended for erupted supernumerary teeth. Because the interdental space in the primary dentition accommodates an additional tooth without any crowding, supernumerary teeth of the primary dentition affect the adjacent teeth less than those of the permanent dentition [23]. In contrast, early intervention is recommended when supernumerary teeth in the primary dentition cause pathological changes or crowding, along with esthetic problems and difficulty in managing oral hygiene [31]. In the present case, the maxillary deciduous central and lateral incisors were displaced palatally, but the primate space in the maxilla decreased (Fig. 1B). Moreover, dental plaque accumulated between the maxillary anterior teeth, and the parents were dissatisfied with the esthetics of the erupted deciduous supernumerary tooth. In consideration of both esthetics and functionality, the middle tooth among the three maxillary central incisors was judged as a supplemental supernumerary tooth and was extracted under moderate sedation with chloral hydrate (45 mg/kg) and hydroxyzine (0.08 mg/kg).
Cone-beam computed tomography (CBCT) has been used to diagnose the shape and location of supernumerary teeth, root fractures of teeth, periapical lesions, and root canal morphology analysis in vivo [32-34]. Micro-CT is limited to in vitro applications and is currently unsuitable for clinical use because of its long imaging duration, high radiation exposure, and small scan area [35]. In contrast, micro-CT has a higher resolution than CBCT, it can more accurately identify the morphology and anomalies of teeth. Recently, cases of teeth in the primary dentition have been reported using micro-CT analysis. Morphological analysis of a supernumerary tooth with facial and palatal cusps with no pulp extension in the primary dentition was introduced [36]. The morphological characteristics of fused deciduous anterior teeth and the root canal morphology of primary molars were examined using micro-CT [37,38]. Micro-CT analysis of natal and neonatal teeth also has been introduced [39,40]. In this case report, micro-CT analysis confirmed root anomalies of the supplemental supernumerary tooth, which were unobserved through direct visual observation or on periapical radiographs. The morphology of normal root canals and the shape of roots in primary anterior teeth are similar [41]. The eruption rate of the supernumerary tooth was faster than that of the adjacent teeth, so root anomaly was suspected. The supernumerary tooth has an abnormal structure of root canal protruding to the inside of the pulp from the apical to the middle third of the root on the palatal surface and a crack-like anomaly inside it (Fig. 5). With the previous diagnostic method, it could be classified as a supplemental type very similar in shape to a normal tooth, but micro-CT analysis confirmed that it had internal anomalies that were clearly different from the normal tooth structure. These morphological anomalies might have weak resistance to external forces and could result in a poor prognosis compared to teeth with a normal structure.
There is a lack of consensus regarding the appropriate age for extracting impacted supernumerary teeth [42]. Considering various controversies, a method for determining whether to extract supernumerary teeth has been proposed based on the condition of supernumerary teeth and the surrounding conditions. Extraction should be performed for erupted supernumerary teeth, except in cases where supernumerary teeth need to be maintained because of the loss of adjacent teeth [43]. For unerupted supernumerary teeth, extraction can be performed at the time of detection or may be delayed. Impacted supernumerary teeth may cause complications such as cysts, intraoral infection, delayed eruption, impaction, displacement, rotation, crowding, diastema, and root resorption of adjacent teeth [44]. Surgical extraction should be considered when lesions are present or expected owing to supernumerary teeth or if esthetic or functional problems exist [45]. Immediate intervention may cause devitalization or root malformation in adjacent teeth. It can also cause dental phobias in young patients who are not yet familiar with dental treatment [23]. Asymptomatic impacted supernumerary teeth that may not affect dentition are sometimes best left in place with continuous follow-up [3]. Surgical removal can also be delayed when the supernumerary teeth or adjacent permanent teeth are in the early stages of tooth development. If the extraction of supernumerary teeth is delayed until the completion of adjacent tooth root development, loss of pulp vitality and abnormal root formation of adjacent teeth can be prevented [43]. Since the patient was too young and experienced no complications related to the impacted supernumerary teeth, it was decided to continue follow-up of the 2 impacted supernumerary teeth.
Summary
In this report, the treatment of a rare case of supernumerary teeth occurring in the early stages of childhood development was described. Clinical and radiological examinations can detect supernumerary teeth, whereas micro-CT can detect microscopic abnormalities in vitro. A male infant without systemic diseases or syndromes showed an erupted supernumerary tooth with root anomalies in the primary dentition and 2 impacted succedaneous supernumerary teeth. Early diagnosis and prompt treatment are crucial to minimizing complications in supernumerary teeth.
Notes
Conflict of Interest
The authors have no potential conflicts of interest to disclose.