



Introduction
There has been an increasing demand for orthodontic treatment with a decrease in the age of patients receiving treatment due to a growing interest in oral health along with the increased need for aesthetic improvement[1,2].
The orthodontic treatment methods that can be used during the mixed-dentition stage include the use of removable orthodontic appliances and the use of fixed orthodontic appliances. Removable appliances can reduce chair time for patients since they can be fabricated in a dental laboratory rather than inside the patientŌĆÖs oral cavity and can be beneficial for oral hygiene management as the appliance can be easily removed in socially sensitive situations. However, since the appliance can only be effective when it is being used by the patient, its therapeutic effect is heavily dependent on the patientŌĆÖs treatment cooperation. One drawback is that complex orthodontic tooth movements are difficult to achieve with the use of removable appliances alone[3].
Treatment with fixed appliances can exert continuous force regardless of the patientŌĆÖs cooperation, but it is considered to be unesthetic, painful, expensive, and have a long treatment period[4,5]. Fixed appliances that use mini tubes to remedy the drawbacks of traditional brackets have been recently introduced. Orthodontic treatment using mini tubes involves the application of round wires with thin mini tubes of low volume for exerting light forces due to reduced friction. The use of these mini tubes is a less visible and less painful treatment method capable of providing rapid local treatment to areas requiring attention. However, it can be challenging to insert and remove the wire in cases of torque adjustments and severe crowding because of insufficient space for attaching the appliance.
Insufficient space for the eruption of permanent anterior teeth and locking of molar teeth are situations that are commonly encountered with patients in their mixeddentition stage. Open coil springs or loops are often applied as a method of using fixed appliances. However, for patients with severely impacted teeth, application is sometimes difficult for both the patient and the dentist because there is not enough space for attachment. Recently, methods that use thin NiTi wires of high elasticity without the use of even the most minimal attachments such as brackets or tubes have been introduced. Using a method that attaches a single-segmented wire, bent in an active state, directly onto the teeth with flowable resin, it becomes unnecessary to deploy the procedures of insertion and removal or the replacement of wires. Due to the application of light force, these thin NiTi wires have fewer side effects and can be used easily and immediately without procedures in the dental laboratory. However, they have rarely been used in pediatric dentistry[6-10].
This report presents three cases of molar uprighting and space regaining using straight 0.012 inch NiTi wire with flowable resin, without the use of even the minimal attachments such as brackets or tubes.
Case Reports
1. Case ŌģĀ
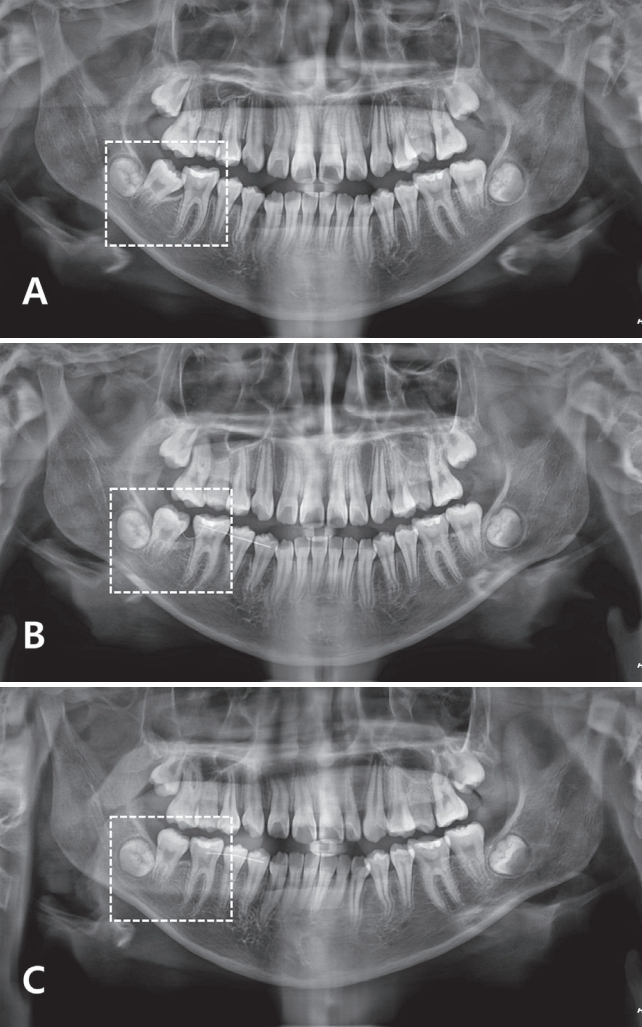
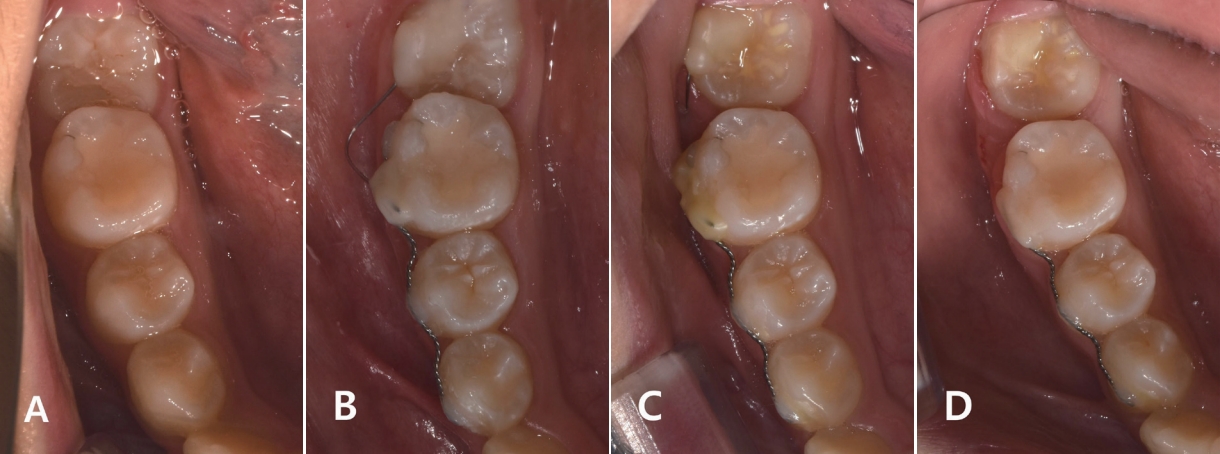
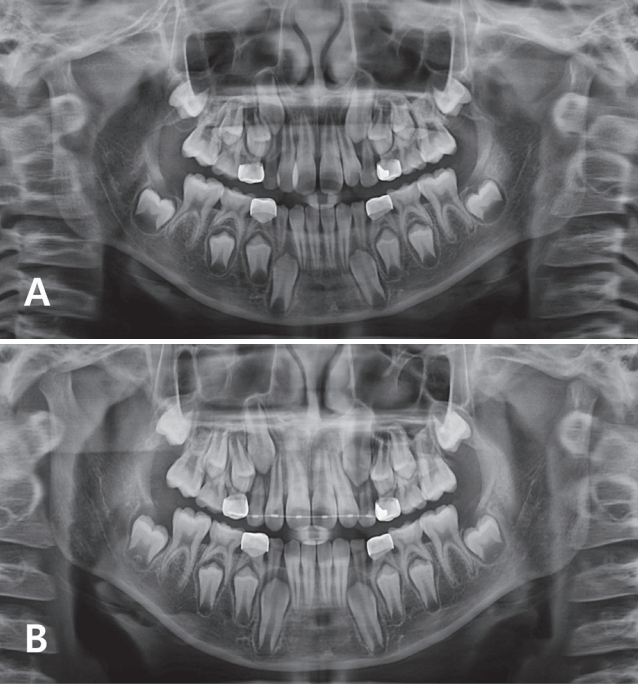
A 10-year-old girl visited the hospital with an impacted mandibular right second molar. The patient had an intellectual disability level II. The results of the oral examination and radiography indicated that the mandibular right second molar revealed mesially angulated impaction, with most of the crown being exposed within the oral cavity. Factors that would hinder orthodontic upright treatment, such as soft tissue growth or the extrusion of opposite teeth, were not observed (Fig. 1A, 2A). To apply distalizing force to the second molar, a straight 0.012 inch NiTi wire (G&H Wire Co, Greenwood, IN, USA) was prepared to be twice the length of the first molar and attached to the mesiobuccal center of the second molar using only flowable resin. The straight wire was then bent until it reached the center of the first molar and fixed in place using flowable resin. To reinforce the anchorage, 0.0175 inch multistranded wire was passively attached to the first, second premolar, and first molar (Fig. 2B). After 1 month of the treatment, the bent NiTi wire straightened and moved the second molar distally, alleviating the locking (Fig. 2C). Two months after the treatment, when 1 mm of space was secured between the first and second molars, the wire was removed and the second molar was allowed to erupt spontaneously (Fig. 1B, 2D). Six months after the treatment, the second molar fully erupted and was level with the adjacent first molar(Fig. 1C). Oral hygiene was good, and there was no wire detachment. Soft tissue impingement occurred, but there was no pain and discomfort during treatment.
2. Case ŌģĪ
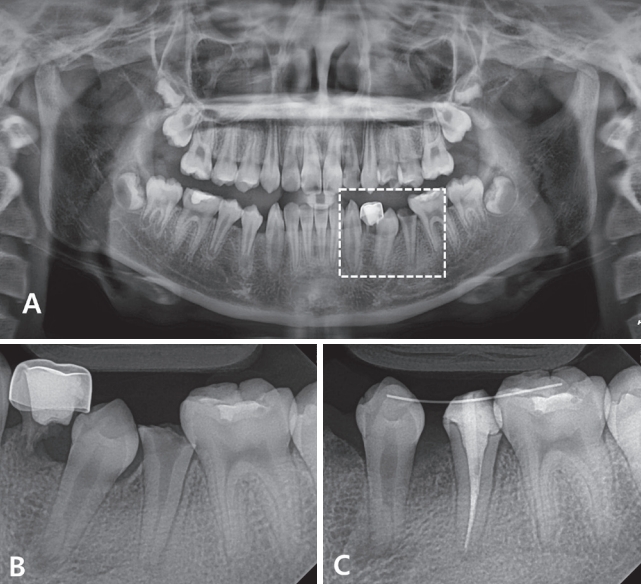
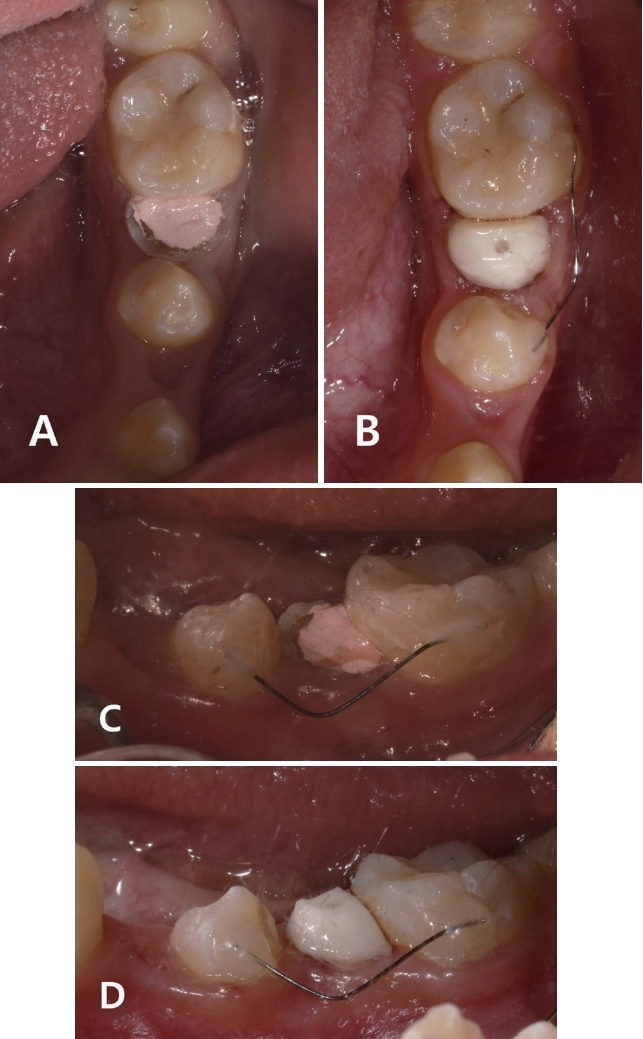
A 12-year-old girl visited the hospital with multiple dental caries. The results of the oral examination and radiography indicated multiple dental caries, ectopic eruption of the mandibular left first premolar, and crown fracture caused by caries in the second premolar (Fig. 3A, 3B, 4A). The initial plan was to place a post and restore the crown after extraction of the mandibular left first primary molar and root canal treatment of the mandibular left second premolar. However, due to the insufficient space for crown restoration caused by the ectopic eruption of the first premolar, orthodontic treatment was necessary to secure space. However, the patientŌĆÖs economic status was difficult, and it was necessary to secure space within a short period of time. Therefore, after the extraction of the mandibular left first primary molar, a straight 0.012 inch NiTi wire was prepared based on the distal distance from the center of the first premolar to the first molar. This wire was attached to the buccal center of the first molar using only flowable resin, and its other end was attached bent to the buccal center of the first premolar with flowable resin (Fig. 4C). As some space had been secured 1 month after treatment, the root canal treatment was finished, and the post and core were applied (Fig. 4B, 4D). As the wire straightened, sufficient space had been secured 2 months after the treatment. Therefore, the wire was removed, and the patient was referred to the prosthetics department for crown restoration (Fig. 3C).
3. Case Ōģó
An 8-year-old boy visited the hospital with maxillary right anterior crossbite. The results of the oral examination and radiography indicated crossbite of the maxillary right central incisor along with insufficient space. Cephalometric analysis revealed skeletal Class ŌģĀ malocclusion. The patient was instructed to use a fan-type appliance with a spring for 1 year to alleviate the crossbite and secure sufficient space. While the crossbite of the maxillary right central incisor was alleviated, not enough space had been secured for arranging the maxillary right lateral incisor due to the lack of cooperation from the patient and frequent loss of the appliance (Fig. 5A). Therefore, a straight 0.012 inch NiTi wire was selected to secure sufficient space, which would then be followed by the arrangement using a minitube appliance. Minitube appliances of 2 mm length were attached to the maxillary anterior teeth with the exception of the maxillary right lateral incisor, which was then followed by the application of a 40 Thermo active 0.012 inch precurved NiTi. After 1 month, the wire was cut at the distal of the maxillary right central incisor. To secure space for the right lateral incisor, a straight 0.012 inch NiTi wire was prepared to be 1.5 times the length of the space for the lateral incisor, attached to the distal surface of the maxillary right central incisor with flowable resin, and bent before being fixed on the mesial surface of the right primary canine with flowable resin (Fig. 6E, 6F). When sufficient space was secured 3 months after the treatment, the wire was removed and a mini tube attached for the leveling of the lateral incisor (Fig. 6G, 6H). The patient was revisited at the hospital after 6 months due to personal reasons, but the alignment was reasonable without side effects such as root resorption (Fig. 5B, 6K, 6L).
Discussion
There have been constant developments in fixed orthodontic appliances, particularly prescribed brackets, since the 1970s, attributing torque, offset, and angulation. However, such appliances are generally perceived as unsightly, painful, expensive, and requiring long durations of treatment. One method to address such drawbacks, while also satisfying the need for aesthetic improvement, is to eliminate the tie wing and bonding base of the bracket by using a tube-shaped attachment. In general, this approach is used for orthodontic treatment of mild to moderate crowding or recurrence following prior orthodontic treatment. However, this method has the difficulties of requiring space to attach the tube and not easy to insert or replace the wire[11,12]. Therefore, new and simpler methods that attach the wire directly onto the teeth without the use of any attachments are currently being introduced. The biggest advantage of this method is that it can attach appliances rapidly and easily on parts that need application. The difficulty in the conversion of the wireŌĆÖs restitution force into couple force due to the lack of a gap and the absence of brackets is addressed by using elastic NiTi wire[13,14]. This is because NiTi wire has a torsional stress that is 1/4th - 1/5th that of stainless steel wire, sufficient strength, and low stiffness, so it can exert an ultra-light force. In addition, it has memory and can regain its original form without deformation. Therefore, it can be applied without any noticeable side effects[2,3]. For this reason, NiTi wire should be used rather than stainless steel wire in situations where the wire is being attached in its bent state.
In case 1, most of the crown of the mandibular right second molar was exposed in the oral cavity, and the tooth was mesially angulated impaction. As the first treatment option, insertion of a separator ring or brass wire was attempted, but insertion into the proximal surface was difficult. In general, such cases are treated with the application of halterman, humphrey appliances, or archwires with the attachment of brackets, where treatment is provided through loops and tip-back springs. However, traditional devices must undergo procedures in the dental laboratory and can be quite burdensome for the dentist, depending on the degree of impact. Moreover, there is a risk of detachment of the appliance, and many of the designs tend to induce discomfort in the soft tissue. The greatest advantage for the bracketless, direct fixation method is the immediate application on the affected parts without requirements for dental laboratory procedures, small volume, and the ease of application. This was particularly important for this patient who had an intellectual disability and could not adhere to treatment without restraining devices. For this patient, who was in the permanent-dentition stage, it seemed necessary to have an anchorage for alleviating the locking of the second molar. A 0.0175 inch multistranded wire was used to splint three teeth in the anterior segment, supplementing the anchorage. The locking started showing improvement from 1 month after the treatment, and the appliance could be removed by the second month. Fortunately, spontaneous eruption was guided for this tooth, and the problem was resolved without severe side effects.
In case 2, the crown was fractured due to severe caries of the mandibular left second premolar. Post and core, and crown restoration were required after root canal treatment. While the case could be treated through the attachment of a fixed appliance, performing leveling procedures, and securing space using an open coil spring, the patientŌĆÖs circumstances made typical treatment unavailable. Since the patient was reporting pain in the second premolar, rapid treatment was necessary, which, in turn, meant that treatment for securing space was also urgently needed. With considerations for the cost-effectiveness of treatment, a segmented NiTi wire was used to secure space within 2 months of treatment. The root canal treatment was completed within those 2 months, and the patient was referred to the prosthetics department for crown restoration. In this case, while the space for the second premolar was somewhat secured, it had been tilted distally compared to its normal location, and the spacing between the canine and the first premolar remained. It is worth speculating whether the outcome would have been better if additional alignment were made prior to preparing the crown after restoring the core. Since the treatment duration was relatively short and recall check attempts were unsuccessful, the stability of treatment and the outcome of prosthesis restoration could not be evaluated.
In case 3, the reason why the mini tubes for aligning of the maxillary anterior teeth, his cooperation with previous treatment using a removable orthodontic appliance was not good. After the alignment had been minorly established, it is necessary to secure space for the maxillary right lateral incisor. Open coil springs could not be used with the mini tube appliance for securing space. Instead, securing space through stripping was one of the treatment options. However, to use methods that would not involve the removal of teeth, space was to be secured using a segmented straight 0.012 inch NiTi wire. Due to relatively severe eruption toward the palate, there were tilts in the axes of adjacent teeth in the process of securing space, and when the right lateral incisor was moved into normal position, extensive decalcification was observed. Fortunately, side effects such as root resorption did not occur, but treatment for decalcified teeth is necessary after removal of the appliance.
As seen in the above three cases, this method can be applied in various locations within the oral cavity including the anterior teeth, premolars, and molars. In the current case study, it was used to treat the locking of the second molar, but it could also be useful for the locking of the first molar in the early mixed dentition stage. However, it can only be used if the eruption is sufficient to allow the tooth surface to be used for attachment. In addition, it can be used as an alternative for inter proximal reduction for securing space when using fixed appliances for anterior alignment during the mixed-dentition stage. However, this method has some limitations since the torque cannot be adjusted, and there is a tendency to induce distobuccal tilt in the case of insufficient space. Therefore, while this method is certainly simple and inexpensive, it cannot establish perfect occlusions or address other abnormalities within the oral cavity. Instead, it should be applied for the appropriate indications, with due consideration for potential side effects. Furthermore, since it has a high probability of resulting in unwanted tooth movement if used without reinforcement of appropriate anchorage, it requires rigorous monitoring[15].
Open coil springs, typically used to secure space, require the attachment of fixed appliances and must be used with sturdy wires after completing teeth alignment. Open coil springs can induce load on the target tooth and the adjacent teeth. However, the straight 0.012 inch NiTi, superelastic wire used in the current study has advantages related to the load since the restitution force is fully distributed to the dental arch and can be efficient for the movement of the target tooth. Optimal orthodontic tooth movement can be induced by light and continuous force. The NiTi wire can exert a light force over a wide area, and its anchorage is less burdensome since it does not apply unnecessarily large forces to move teeth. While the diameter of the NiTi wire is not related to the degree of alleviation of crowding, larger diameters can shorten the time required for tooth movement. However, this decrease in time is at the cost of potential distobuccal tilts or extrusion of teeth, which can even lead to damage to nearby tissues due to strong orthodontic forces. Therefore, the current study used 0.012 inch NiTi wire, rather than 0.014 inch or 0.016 inch, to minimize side effects in the process of achieving tooth movements[16-18]. If a circular wire is bent before it is placed, it always exerts a couple force in its balance of power, as the wire tries to return to its original shape. Since the wire is shaped in the form of a circle, it is unlikely that there will be an imbalance in the force exerted by the wire. However, depending on the anchorage, tooth movement on either side can result in an imbalanced outcome. Moreover, the length of the wire segment was designed to be 1.5 times the distance between the centers of the teeth, to which the wire was attached, to enable the attachment of the wire to the distobuccal center of teeth using flowable resin. When both ends are fixed, doubling the length of the wire increases the intensity twofold while decreasing the elasticity to 1/4th. Thus, this length of the wire was appropriate and did not result in excessive force[3].
Through these three case studies, orthodontic treatment through bracketless, thin, straight 0.012 inch NiTi wire segments has been demonstrated to be simple and have a short duration, resulting in acceptable outcomes without serious side effects. While this method cannot be considered more complete than existing orthodontic treatment methods, it is considered to be useful as an alternative treatment option in applications for patients transitioning from their mixed-dentition stage to the permanent-dentition stage.
Summary
Orthodontic treatment using the light force exerted by straight 0.012 inch NiTi wire segments has shown satisfactory outcomes for impacted teeth and insufficient space occurring in various locations within the oral cavity for pediatric patients, considering the relatively short durations of treatment and effectiveness. This treatment method can be a compromised minor orthodontic treatment considering the maturity of teeth, patient cooperation, and economic aspects.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






