



Introduction
Odontogenic cysts are epithelial-lined pathologic cavities surrounded by fibrous connective tissues that originate from odontogenic tissues and occur in the maxilla and mandible [1]. Since there are few clinical symptoms, these cysts are often incidental radiographic findings. For example, when radiographs are taken during routine dental check-ups or when delayed eruption of the permanent teeth is noted [2]. In young children with developing permanent teeth, delayed detection of these cysts can lead to the displacement of the permanent successors as well as disturbance to the surrounding anatomical structures.
Treatment strategies for odontogenic cysts include enucleation, marsupialization, or decompression. Marsupialization and decompression have been defined as different surgical techniques, but this is the same in that these approaches are aimed at decreasing the size after opening the cyst to the oral cavity [3]. The choice of treatment is dependent on the size or location of the cyst and the surrounding structures affected by the cyst. For cysts that are large enough to displace anatomical structures, marsupialization or decompression is recommended to reduce complications, such as damage to the adjacent anatomical structures, facial deformation, tooth resorption, and nerve damage [4]. Once a cyst has been treated, the pediatric patient should be reviewed regularly via clinical and radiologic examinations. In particular, the eruptions of the permanent successors should be monitored. If the permanent teeth do not spontaneously erupt, surgical exposure, orthodontic traction, or other advanced treatment should be considered [5].
In previous studies of cysts in pediatric patients, the incidence of odontogenic cysts was 2.3 times higher in the mandible than in the maxilla [6]. As a result, some studies have shown that following the treatment of a cyst, spontaneous eruption of the permanent teeth mainly occurs in the mandible [6-9]. In contrast, comprehensive treatment, including eruption guidance after cyst treatment in the maxillary anterior area, which is referred to as ŌĆśSocial SixŌĆÖ and is clinically significant, is rarely reported.
In this report, we described two cases with good prognoses that were managed via multidisciplinary treatment. The large cysts, which displaced several permanent teeth and adjacent structures, such as the maxillary sinus, were treated by marsupialization, followed by obturator and eruption guidance.
Case Reports
This study was conducted with the approval of the Institutional Review Board of Kyungpook National University Dental Hospital (IRB No: KNUDH-2022-09-01-00). Informed consent was obtained from the patientŌĆÖs legal guardian for the publication of this case report and any accompanying images.
1. Case 1
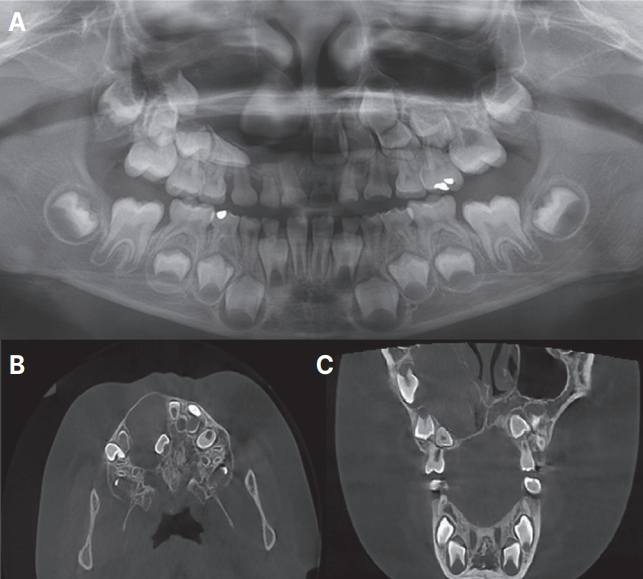
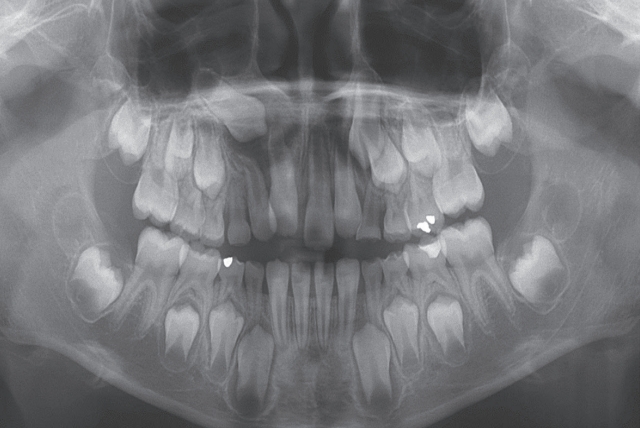
A 5-year-old boy was referred to the Department of Pediatric Dentistry at Kyungpook National University Dental Hospital by a local dental clinic for the management of right permanent central incisor impaction. His medical history was unremarkable. On dental examination, trauma to the right maxillary deciduous central incisor was noted, and the tooth was discolored. Radiological examination revealed a radiolucent lesion with a well-defined margin extending from the right maxillary first premolar to the right maxillary central incisor (Fig. 1A). Cone-beam computed tomography (CBCT) showed expansion of both the labial and palatal cortical plates in the affected region, displaced permanent successors, displacement of the lateral wall of the nasal cavity, and severe superior displacement of the sinus floor (Fig. 1B-C).
A tentative diagnosis of a dentigerous cyst was made. Considering the clinical and radiological findings, marsupialization was planned, and orthodontic traction was considered necessary due to the severity of the displaced teeth. The treatment plan was decided after discussing it with the guardian.
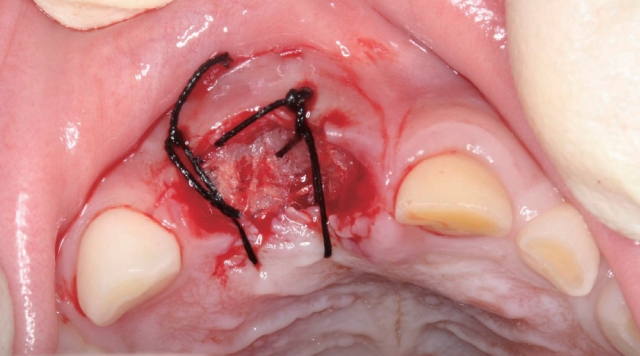
Under local anesthesia, the right maxillary deciduous central incisor and lateral incisor were extracted, and marsupialization was performed. Vaseline gauze was inserted into the extraction socket and sutured (Fig. 2). The opening was maintained by replacing the vaseline gauze and surgical cement regularly for up to 3 weeks after marsupialization. Vaseline gauze is located at the bottom of the opening site, and the surgical cement is located at the top, so it has a double-packed structure. After complete epithelialization, a customized acrylic obturator with extended resin projection inside the extraction socket was placed 3 weeks after marsupialization.
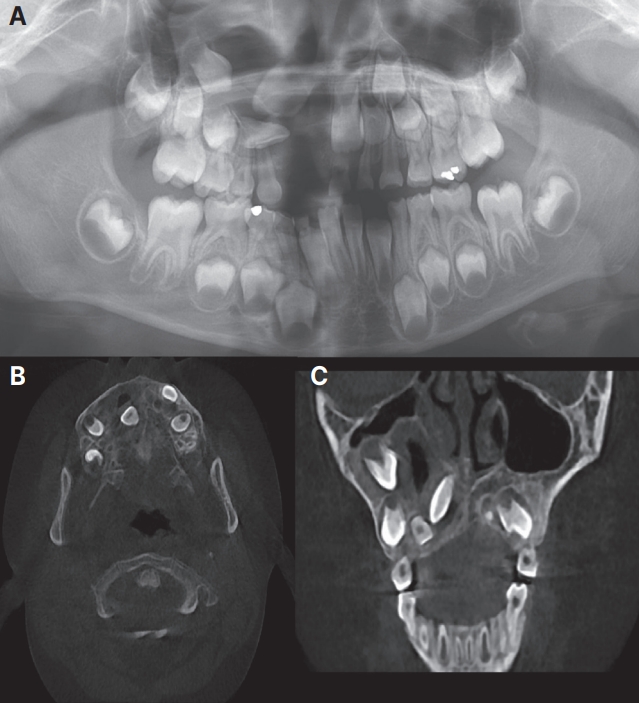
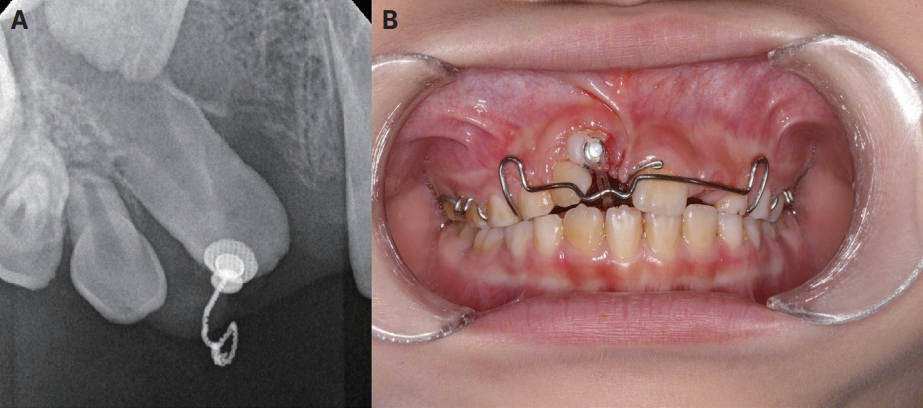
Three months after marsupialization, tooth movement associated with a decreased size of the lesion was confirmed by CBCT (Fig. 3). Five months after marsupialization, orthodontic traction of the right maxillary lateral incisor was performed (Fig. 4A). Twelve months after marsupialization, orthodontic traction of the right maxillary central incisor was carried out (Fig. 4B). Nineteen months after marsupialization, the area where the large cystic lesion was continued to heal, and the right maxillary central and lateral incisors erupted into the oral cavity (Fig. 5). However, the unerupted right maxillary canine appeared ectopic.
2. Case 2
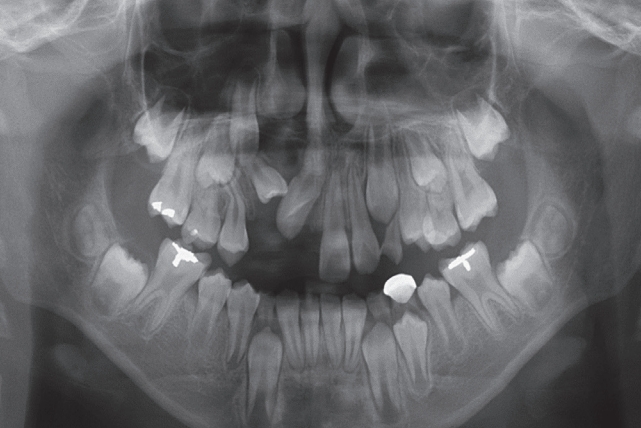
A 10-year-old boy was referred to Kyungpook National University Dental Hospital by a local dental clinic for the management of a cyst in the right maxillary anterior area. The patientŌĆÖs medical or dental histories were uneventful. Clinically, the left maxillary central and lateral incisors were present. Conversely, the right maxillary central and lateral incisors had not erupted. The right maxillary deciduous lateral incisor and canine were in the residual root state. Radiographically, a radiolucent unilocular cystic lesion extending from the right maxillary central incisor to the right maxillary canine was detected (Fig. 6A). CBCT demonstrated bony expansion and cortical bone thinning in the labiopalatal direction, and multiple permanent successors were greatly displaced. In the coronal view, superior displacement of the maxillary sinus floor was shown (Fig. 6B-6C).
Dentigerous cyst was the tentative diagnosis. Marsupialization was planned. Orthodontic intervention was also proposed if the permanent teeth did not erupt normally at the next follow-up appointment.
The right maxillary deciduous lateral incisor and canine were extracted, and marsupialization was performed under local anesthesia. Vaseline gauze and surgical cement were packed following marsupialization to maintain the opening (Fig. 7A). Three weeks after marsupialization, an obturator was placed buccally (Fig. 7B).
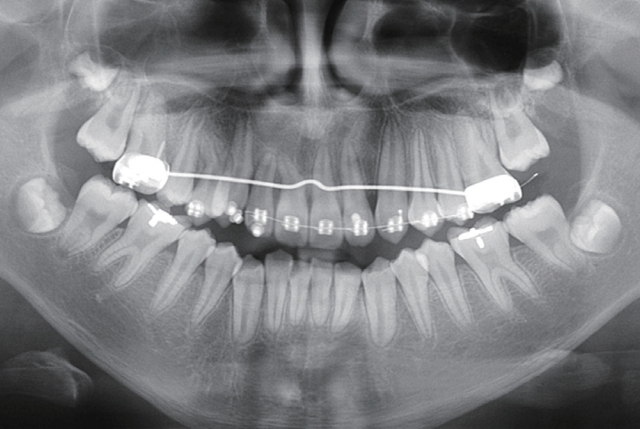
Five months after marsupialization, a panoramic radiograph was taken, which confirmed progressive bone healing (Fig. 8). Nine months after marsupialization, window opening was performed to improve the eruption paths of the central and lateral incisors (Fig. 9). Subsequently, fixed orthodontics was commenced. After 21 months of orthodontic traction with a fixed appliance, the right maxillary incisor, lateral incisor, and canine were aligned, and the surgical wound was replaced by new bone (Fig. 10).
Discussion
Marsupialization is a surgical technique that converts the inner wall epithelium of the cyst into oral epithelium by removing the lining of the cyst wall, which leads to regeneration of the surrounding structures by reducing pressure in the cyst, without causing tissue damage. Compared to enucleation, marsupialization is simple and easy. It preserves and protects the affected teeth and surrounding anatomical structures, such as the maxillary sinus and the inferior alveolar nerve. Moreover, complications such as infection or fracture are rare. Hence, marsupialization is recognized as a conservative and successful treatment[6].
However, there are disadvantages to the fact that pathological tissue remains in its original position and that the cystic cavity must be kept open for a long time. As a result, the treatment duration is long, and the cavity must be kept clean. Kim and Lee[4] argued that for large cysts, decompression is the preferred primary treatment because the histological changes following decompression result in tissues that are similar to the normal oral epithelium, and the recurrence rate is low. Nakamura et al. [10] and Furuki et al. [11] also recommended marsupialization for the management of cystic lesions, because there is no risk of recurrence or deterioration, even for the management of lesions with a high recurrence rate, such as ameloblastoma and odontogenic keratocyst.
In both cases, the large, expansive cystic lesions elevated the floor of the maxillary sinus and displaced three or more teeth. Management by enucleation was predicted to damage the surrounding anatomical structures and result in the loss of the displaced permanent teeth. Therefore, marsupialization was proposed to preserve the affected permanent teeth and surrounding structures, followed by eruption guidance. In both cases, migration of the displaced permanent teeth and recovery of the elevated maxillary sinus were observed after 3 - 5 months following marsupialization. Serra e Silva et al. [12] argued that the bone regeneration speed in children is faster than that of adults and that bone remodeling can only be induced by decompression of the cyst. Studies on the speed of bone regeneration have found that in marsupialization, new bone is generally formed after 6 - 12 months. However, another published report suggested 3 months [3].
When determining the opening site for marsupialization, it is important to widen the entrance while positioning the opening site at the bottom of the cyst for dressing from a surgical perspective [13-14]. In young patients with developing permanent teeth, it is necessary to consider not only cystic pressure relief but also the eruption guidance of the affected permanent teeth. For this purpose, an opening site in the alveolar ridge is preferred. In case 1, the opening site is maintained by the socket following the extraction of the affected deciduous teeth, which aims to promote cyst removal and eruption guidance at the same time. In case 2, marsupialization was performed from the buccal surface instead of the extraction socket because the right maxillary central and lateral incisors were close to the extraction socket.
In both of our cases, vaseline gauze and surgical cement were packed into the opening immediately after marsupialization. Vaseline gauze is a simple, safe, and comfortable way to treat osseous defects. It absorbs inflammatory exudate from large cysts and seals the cyst lumen to maintain a moist, antiseptic environment, which encourages early vascular and cellular invasion by close contact with the detached bony piece. As a result, bone regeneration occurs and the size of the cyst decreases. Moreover, the cyclical lining changes into an oral epithelium [15-17]. Similarly, surgical cement is used to maintain space for inserting the obturator, which functions as a physical barrier to prevent the entry of food and other foreign substances. For our 2 patients, the vaseline gauze and surgical cement were maintained for approximately 3 weeks. After changing the cyst lining to an oral epithelial lining, the obturator is constructed and inserted. In case 1, customized acrylic obturator with resin projection extended inside the extraction socket was selected to induce gradual ossification, space maintenance, and eruption guidance. A certain amount of the resin projection was adjusted at each follow-up visit to enable bone regeneration and the eruption of the permanent teeth. By using an obturator, the number of appointments is reduced, compared with the dressing. The patients were educated about the importance of periodic visits and optimal cleaning of the cyst cavity for the prevention of secondary infection.
In marsupialization, cooperation of patients is required due to the construction and fitting of the obturator, treatment period and follow-up visits. Although the degree of cooperation affects the prognosis for most treatments, patient and guardian cooperation is essential, especially after marsupialization. Tanaka et al. [18] concurred that patient cooperation in maintaining oral hygiene affects the success of marsupialization more than the skills of the dentist. In our cases, continuous cooperation during the protracted treatment and observation periods was evident. Cooperation was enhanced because we explained the expectations and long duration of the treatment during the initial discussion. The patient and guardian were informed that the final treatment goal was the eruption and alignment of the permanent teeth. Understanding this led to excellent cooperation and ultimately, a good prognosis.
In our patients, tooth movement was observed within 2 to 3 months after marsupialization. After marsupialization, approximately 31% - 89% of the affected teeth erupt [12,19-20]. The age of the patient, the position of each displaced tooth, the angulation of each tooth, the eruption potential of each tooth, and the degree of root formation are important factors for eruption [21-22]. Jena [23] also indicated that displaced teeth usually erupt into the oral cavity, regardless of the degree of root growth, cyst size, and dental arch size. In both of our cases, the potential for spontaneous eruption was considered good because the development of the affected tooth root was not yet complete. After marsupialization, we monitored the eruption periodically. The movement of the teeth was confirmed, but the ectopic position was observed. Nawrocka et al. [24] recommended that when the depth of the impact tooth is above the line crossing 1/2 root of adjacent tooth, when angulation is severe, or when there is insufficient alveolar boundary condition, starting orthodontic traction is preferable to waiting for spontaneous eruption after marsupialization. Intervention to optimize tooth eruption was necessary in our cases. Eruption guidance started 5 - 9 months after marsupialization. Of note, Miyawaki et al. [5] highlighted that 3-month after marsupialization is an important time for deciding whether to perform tooth extraction or orthodontic depending on the extent of migration of the displaced tooth.
Various factors can hinder normal tooth eruption in the maxilla following marsupialization. These include the severity of the tooth or teeth displacement, the size of the cyst, and the anatomical features of the maxilla. A cyst in the maxilla can expand from mesial to distal, or buccal to palatal, and from the maxillary sinus to the alveolar ridge. Thus, considering the longer eruption paths, maxillary teeth are less likely to erupt into their normal positions after the removal of the lesion causing the tooth displacement. Moreover, Kjaer [25] reported that the eruption speed and tendency for ectopic eruption are affected by the quality and maturity of the compact bone. Ectopic eruption may be caused by rapid tooth movement in the maxilla due to weak resistance, such as at the opening site before the bone is healed [26]. Contrary to what we observed in our cases, Ertas and Yavuz[27] reported a case in which the arrangement was completed with the marsupialization of a large mandibular cystic lesion only, although 4 teeth were displaced in the mandible.
Our findings suggest that ectopic eruption and space management should be kept in mind when a large maxillary cyst is detected in the maxillary anterior region. If these are observed, surgical and orthodontic interventions should be performed at an appropriate time. Moreover, it is also important to continuously monitor tooth movements.
Summary
In our cases, we described eruption guidance about 2 patients who showed displaced 3 or more permanent teeth and adjacent structures due to expansive large cyst. Marsupialization was performed to protect the surrounding structures, and after 3 weeks of confirming the epithelialization of the cyst lining, a customized acrylic obturator was inserted for eruption guidance. The ectopic path of the affected teeth was observed during regular checkups, and orthodontic traction was started after 5 - 9 months of marsupialization. Displaced teeth were erupted into the arch and aligned after 19 - 21 months of marsupialization. We recommend that pediatric patients with developing permanent teeth large cysts be managed via a comprehensive and long-term treatment plan with consideration to patient cooperation.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






