매복 상악 견치의 처치
Management of Maxillary Impacted Canines
Article information

Abstract
상악 견치는 기능과 외모에 있어서 중요한 역할을 하지만, 맹출 장애로 인해 문제를 일으키는 경우가 많다. 상악 견치의 매복은 비교적 흔하며 구조적 장애, 발달 이상, 공간 부족, 유전과 같은 다양한 요인에 의해 발생할 수 있다. 상악 견치의 구개측 매복은 서양인에게서 흔한 것으로 보고되지만 한국인에게는 순측 매복이 더 흔한 것으로 관찰된다. 순측으로 변위된 상악 견치의 경우, 치아 총생 및 골격성 부정교합이 보일 수 있으며, 측절치의 선천적 상실이나 과잉 측절치는 상악 견치의 구개측 매복 가능성을 높일 수 있다. 상악 견치 매복의 조기 발견 및 적절한 처치는 조화로운 치열 발달과 정상적인 치아 기능을 위해 중요하다. 본 종설을 통해 매복 상악 견치의 다양한 처치법을 제안하고 그 원리를 설명하고자 한다.
Trans Abstract
The canine tooth is important both functionally and aesthetically, being positioned between the anterior and posterior teeth. The upper canine has the longest eruption path, forming in the deepest part of the maxillary bone and often experiencing eruption disorders, leading to significant aesthetic and functional issues. Early detection and management of canine impaction are crucial in pediatric dentistry, which focuses on tooth growth and eruption. The prevalence of maxillary canine impaction ranges from 1.1% to 3.0%. In Western populations, palatal impaction is twice as common as labial impaction, while some Korean studies report more labial impaction. Maxillary canine impaction occurs more frequently in women and is associated with various factors such as structural obstacles, pathological conditions in surrounding tissues, developmental abnormalities, and genetic factors. Labial displaced canines are linked to narrow maxillary intercanine width, total dental crowding, and skeletal Class III malocclusion. Maxillary palatal displaced canine impaction is more prevalent in patients with familial agenesis of lateral incisors or conical supernumerary lateral incisors. Understanding these factors aids in early diagnosis and appropriate intervention for canine tooth impaction, ensuring optimal oral health and aesthetics.
서론
치아가 악골에서 발생하여 기능하는 위치까지 이동하는 일련의 과정을 치아의 맹출이라 한다. 맹출 과정에 문제가 생겨 치아가 정상적인 위치에 도달하지 못하는 경우를 맹출장애라 한다. 유치열이 혼합치열기를 걸쳐 영구치열로 교환되는 소아 및 청소년기에서는 맹출 장애를 종종 관찰할 수 있다. 맹출장애에는 여러 가지 유형이 있는데, 이중 치아가 장애물에 가로막히거나 맹출 경로가 정상에서 많이 벗어난 경우를 매복이라 한다.
견치는 전치부와 구치부의 이행부에 위치하여 기능적 및 심미적으로 중요한 치아이다. 상악 견치는 턱뼈의 가장 깊은 곳에서 형성되어 완전히 맹출하기까지 가장 긴 맹출로를 갖기 때문에 맹출장애가 자주 발생하는 치아이며, 이 경우 심미적 및 기능적으로 큰 문제가 발생하게 된다. 따라서 치아의 발육 및 맹출을 관리하는 소아치과에서 매복 견치를 조기에 발견하고 관리하는 것이 중요하다.
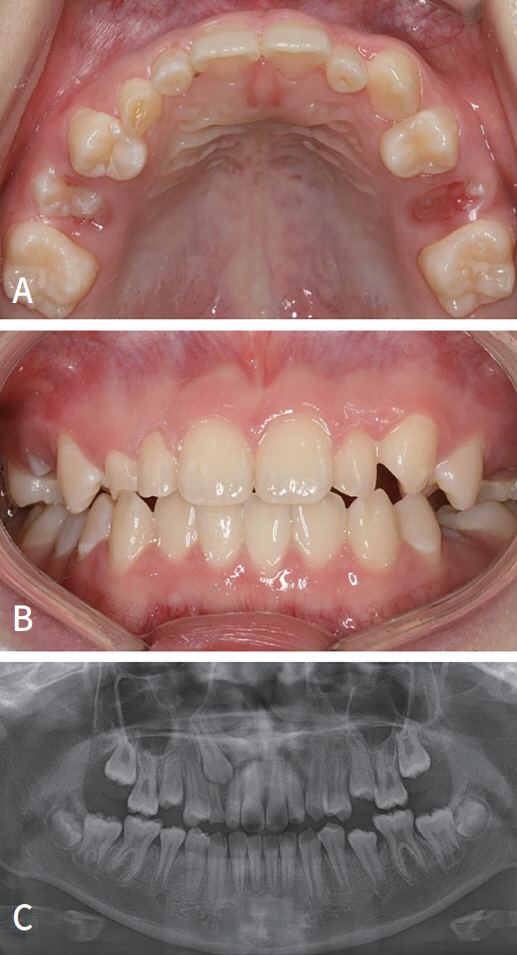
상악 견치 매복의 유병률은 1.1 - 3.0% 정도로 알려져 있다(Fig. 1). 서양인을 대상으로 한 연구에서는 입천장 쪽(구개측)으로 매복된 견치가 입술 쪽(협측)으로 매복된 견치보다 2배 가량 더 자주 발생하는 것으로 보고하고 있지만[1-3], 동양인에서 는 협측 매복이 더 많이 관찰된다는 연구들이 있다[,5]. 상악 견치 매복은 여성에서 더 호발하는 것으로 알려져 있다[3,6].
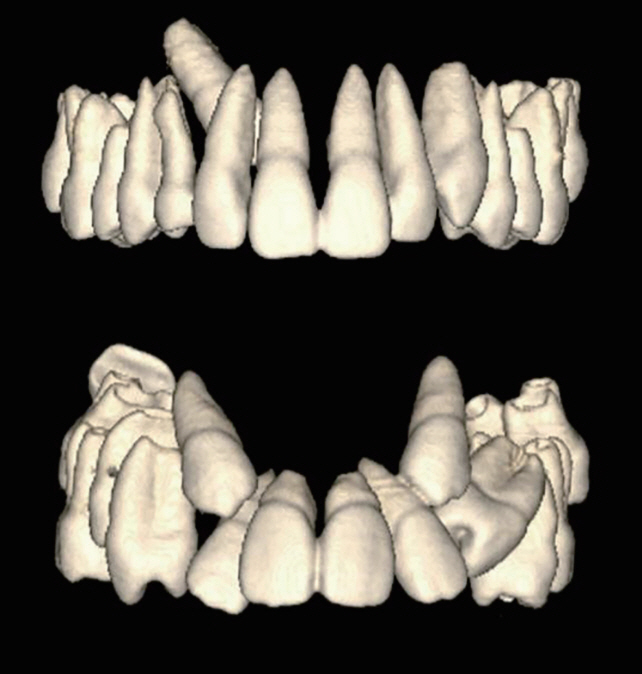
Most maxillary canine impactions diverge in either of the two directions: palatal or buccal.
상악 견치의 매복은 과잉치, 치아종, 만기 잔존 유치와 같은 경조직 장애물, 유치 치근단 병소, 영구 견치 치낭의 확장과 같은 연조직 병변, 인접 측절치의 발육 이상 또는 결손으로 인한 맹출 유도의 부재, 맹출 공간의 부족, 유전적 요인 등의 병인 요소가 복합적으로 작용하여 발생하는 것으로 여겨진다[7].
협측과 구개측 매복의 양상에 따라 치아 및 악골의 특성에 차이가 관찰된다. 협측 매복 견치를 가지는 환자에서 좁은 상악 견치간 폭경, 상악 치열 총생, 골격성 3급 부정교합의 빈도가 높은 것으로 나타났다[8-10]. 한편 가족력을 보이는 측절치의 결손이나 원추형 왜소 측절치와 같은 이상이 있을 때 상악 견치의 구개측 변위의 발생 가능성이 높은 것으로 보고된다[11,12]. 즉, 상악 견치의 협측 매복은 공간 부족이, 구개측 매복은 맹출 유도의 부재 및 유전적 요인이 주요 원인인 것으로 여겨진다.
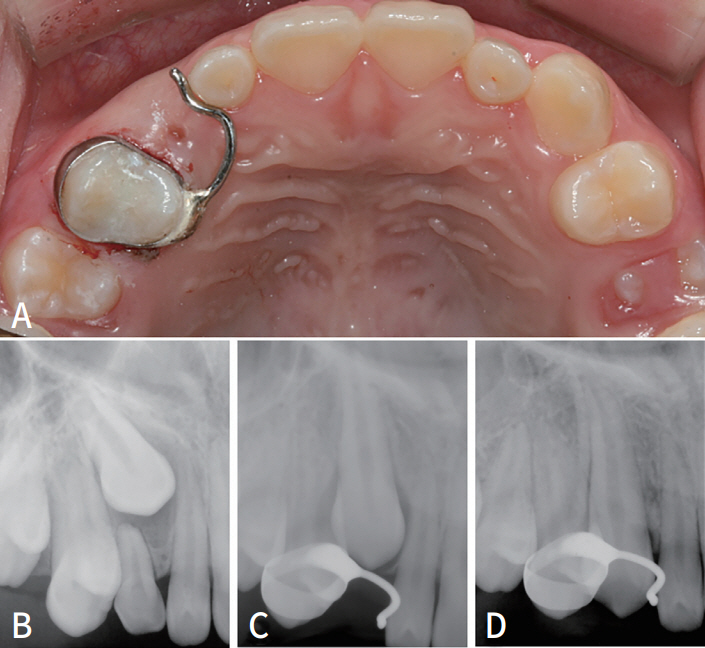
상악 견치가 매복된 경우 치열궁 길이의 감소, 인접 치아의 경사, 매복치의 낭종 형성, 인접치의 치근 흡수 등이 발생할 수 있다. 매복치에 의한 인접치의 치근 흡수는 비가역적이며 가장 심각한 합병증으로 볼 수 있는데[13], 최근 CBCT를 이용한 연구에서 매복 견치의 절반 정도가 인접치의 치근 흡수를 야기하는 것으로 보고되었다[14]. 인접치의 치근 흡수는 남성보다 여성에서 더 자주 발생하며, 구개측 매복 견치보다 협측 매복 견치에서 빈번히 나타난다는 보고가 있다[14,15](Fig. 2).
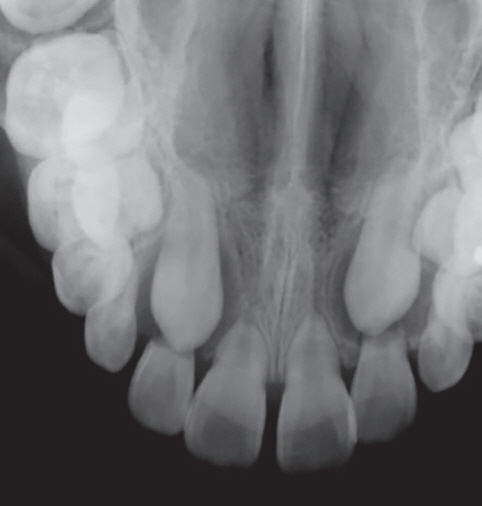
Impacted canines resorbed the roots of adjacent teeth.
치근 흡수에 따른 통증이나 동요도는 치근 흡수가 상당히 진행된 후에 나타난다. 따라서 인접치에 뚜렷한 증상이 없다 하더라도 매복 견치가 의심되는 경우 CBCT를 촬영하여 인접치의 치근 흡수 여부를 정확히 평가하는 것이 권유된다. 치근 흡수가 관찰되는 경우에는 즉시 적극적인 방법의 치료 개입이 필요하다.
본론
1. 진단
매복 견치로 의뢰되어 오는 많은 환자를 보면 예방과 치료 시기를 놓쳐 인접치의 치근 흡수를 일으키는 최악의 경우를 겪는 환자가 많다. 이는 견치 매복의 예측과 진단의 어려움 때문이다. 최근 파노라마 사진과 CBCT가 대중화되면서 매복 견치를 좀 더 일찍 발견하는 경우가 많아졌지만 방사선 사진뿐만 아니라 여러 가지 임상적 경험과 진단 방법을 동원해야 한다.
1) 언제 치아의 매복을 의심할 수 있나?
매복 견치는 사랑니처럼 큰 통증 등의 문제를 일으키지 않으며 유치 송곳니는 비심미적이긴 하나 일반인의 눈에는 큰 차이가 없기 때문에 견치 매복의 진단은 주기적이고 세심한 구강검사가 중요하다.
만약 반대편 치아가 맹출한 후 6개월 이상이 지나고 치근이 2/3 이상 형성되어 있는데도 치아의 방향이 정상에서 벗어나 있거나 구강 내와 어느 정도 거리를 유지하고 있다면 매복을 의심해야 한다.
만11 - 12세 때에도 견치가 맹출하지 않았거나 자연스럽게 폐쇄되어야 하는 중절치 간의 간격이 존재한다면 의심해 볼 필요가 있다.
2) 촉진
견치가 협측에 위치한 경우 맹출 2 - 3년 전부터 유견치 상방에서 촉진이 가능하다. 협측에서 촉진이 안되는 경우에는 구개 측도 확인하고 유견치의 동요도도 반드시 검사해야 한다.
3) 방사선 검사
치근단 방사선 사진 및 교합 방사선 사진 등이 보조적으로 활용되지만, 파노라마 방사선 사진 및 CBCT 사진이 진단에 있어 가장 유용하다.
파노라마 방사선 사진은 전반적인 치열 및 악골을 전체적으로 보여주기 때문에 매복치를 찾아내는 데 있어 유용한 기본적인 방사선 사진이다. 일부 구조물들을 변형시키고 중첩시키는 경향으로 인해 매복치의 정확한 협설적 위치와 수평면에서의 치열궁과의 관계를 정확하게 결정하는 데에는 부적합하지만, 현실적으로 가장 유용한 수단이다.
CBCT는 치아의 위치를 정확히 보여주는 유용한 진단 도구이다. 방사선 기술의 발전으로 인해 현재 노출량도 현저히 감소하였다. 3차원 재구성 영상을 통해 개개 환자의 해부학적, 형태적 특성을 3차원적으로 인식하는 것을 돕고, 좀 더 적절한 치료계획을 수립할 수 있게 한다.
2. 치료
상악 견치의 맹출을 방해하는 과잉치, 치아종 등이 있는 경우에는 물리적인 장애물을 제거하는 것이 선행되어야 한다. 매복된 견치를 치료하기 위해서 다음과 같은 방법을 사용하게 된다.
1) 맹출 공간 확보 및 맹출의 주기적 관찰
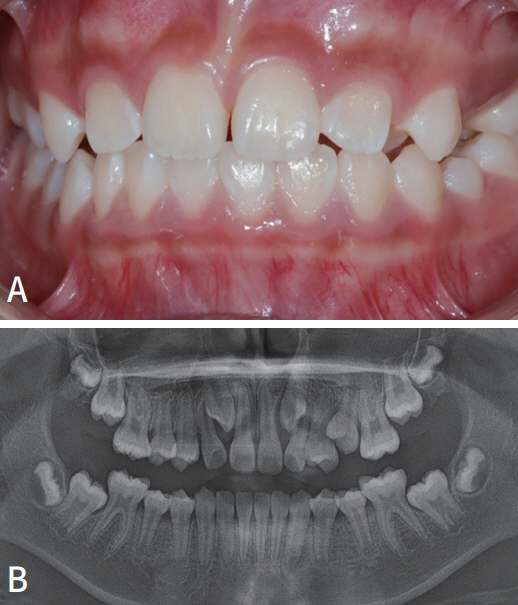
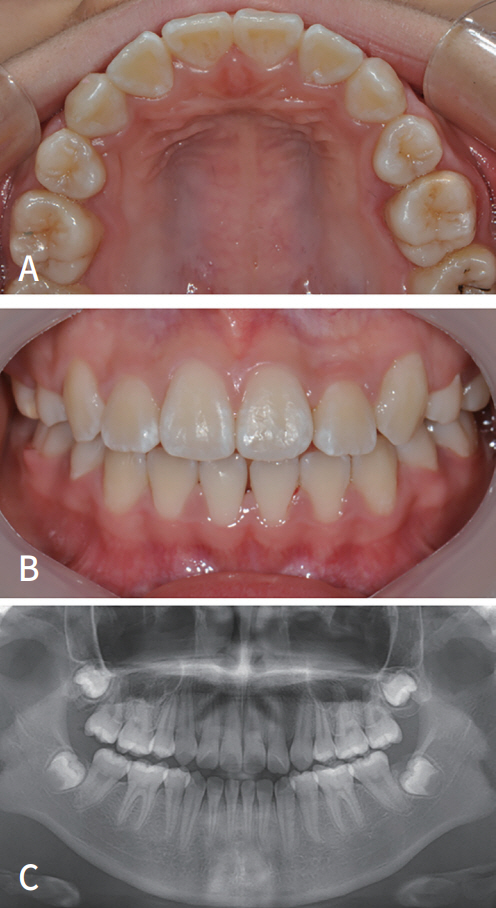
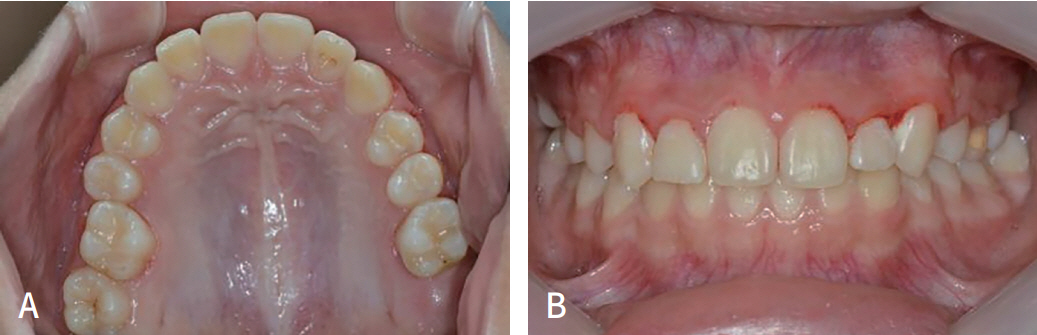
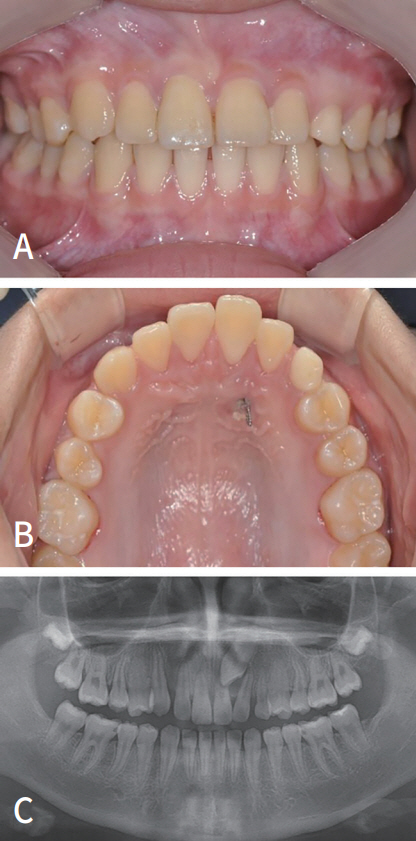
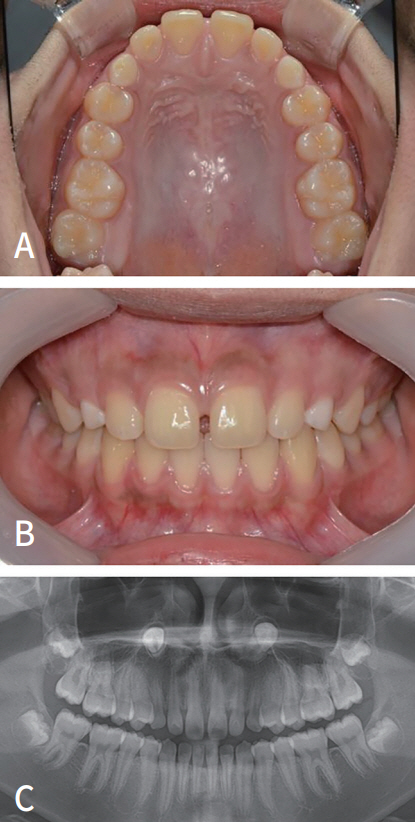
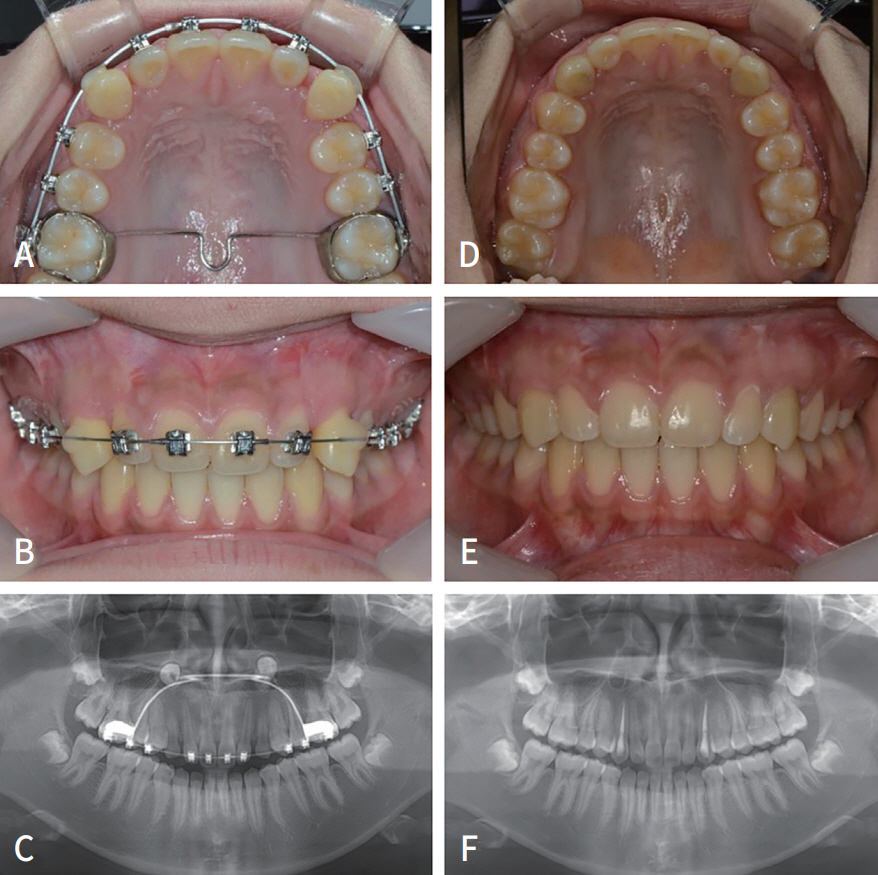
견치 매복의 원인이 부족한 악궁 공간에 의한 것이라 판단될 때는 악궁 확대 장치를 사용하면서 견치의 맹출을 주기적으로 관찰하는 것을 고려해 볼 수 있다(Fig. 3, 4).
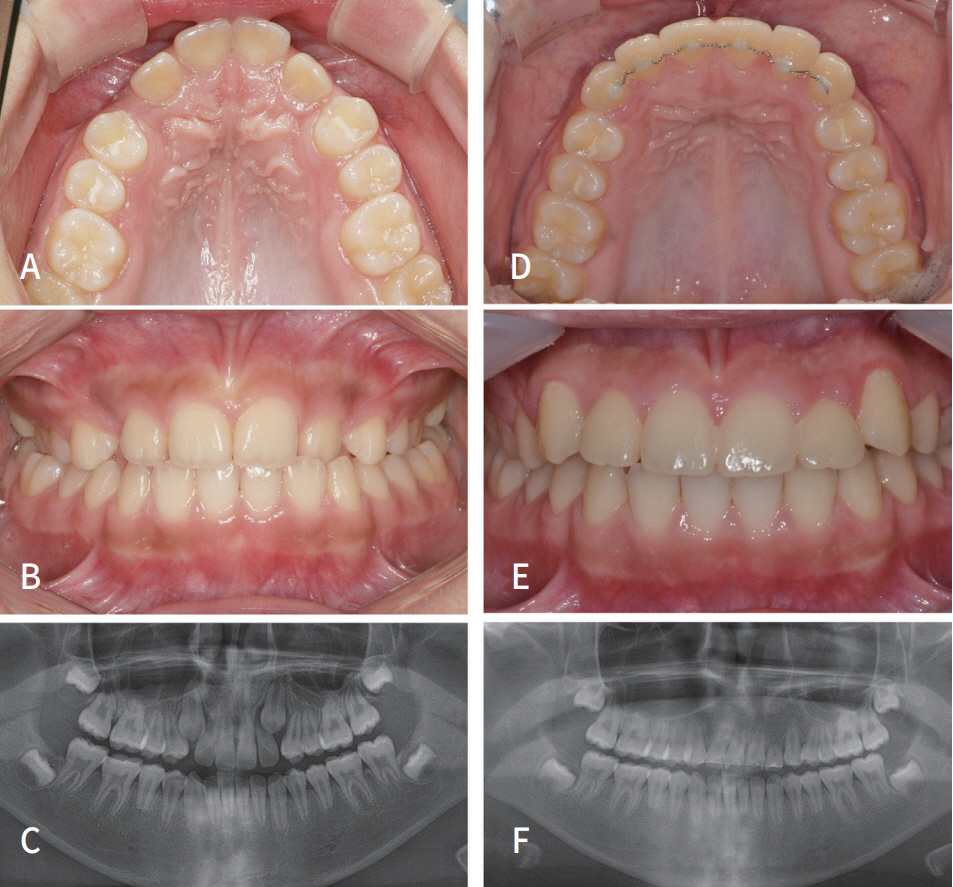
A 10-year-old girl had space deficiency and posterior crossbite (A - C). After 2 years of orthodontic treatment, including space augmentation, the teeth were well aligned (D - F).
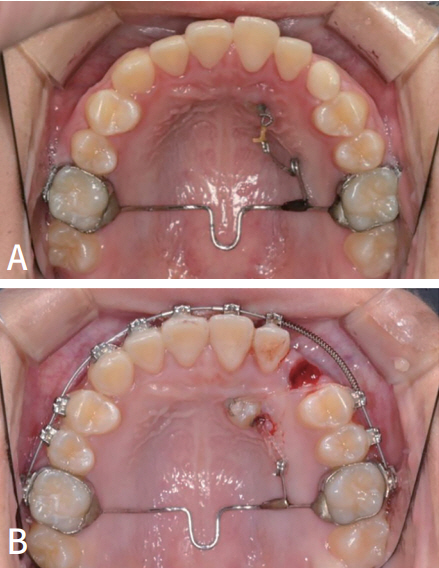
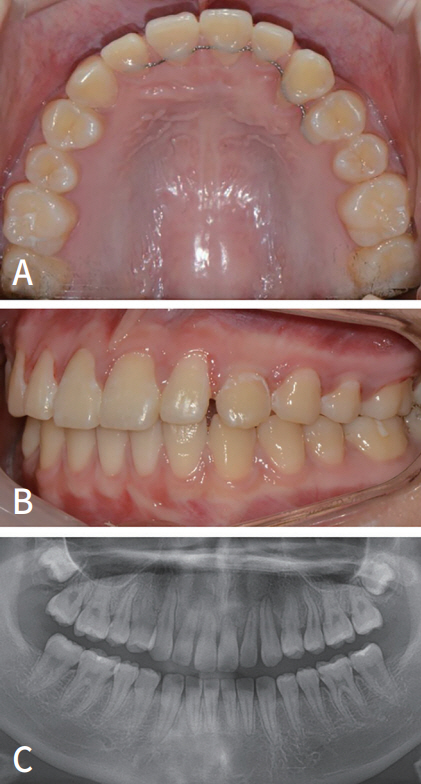
Space augmentation with the RME appliance and continued space opening with coil springs had been implemented (A - F). Maxillary expansion and space opening made room for an impacted canine. This may have stimulated the eruption of the canine into the correct position.
2) 유견치의 차단적인 발거
견치의 맹출방향이 근심 교합면을 향하고 인접치 치근과 겹쳐있을 때 유견치의 조기 발거 만으로도 어느 정도 견치의 정상적인 맹출을 유도할 수 있다(Fig. 5, 6). Ericson 등은 구개측 매복된 견치에서 60 - 90% 정도의 높은 성공률을 보인다고 보고하였다[16]. 저자의 경험 상 한국 어린이들에서 많이 나타나는 협측 매복에서는 높은 성공률을 보장할 수 없다. 한국 어린이들을 대상으로 유견치의 차단적 발거의 효과를 살펴본 최근의 연구에 따르면, 견치의 협측 매복은 차단적 유견치 발거의 성공률을 낮추는 요인으로 나타났다[17]. 치근 흡수가 없이 구개측 로 매복되어 있는 경우는 유견치의 발거 후 견치의 맹출 유도가 잘 되는 편이지만 견치 치관이 측절치 치근의 반 이상을 넘어간 협측 매복인 경우 유견치의 발거 만으로는 맹출 유도가 성공적으로 일어나지 않을 수 있다.
An 11-year-old girl had an ectopic eruption of the right maxillary canine (A - C).
After extraction of the primary canine, the pathway of the impacted canine was improved, and spontaneous eruption proceeded (A - D).
3) 매복 견치의 발거
치열궁의 공간도 부족하고, 매복 견치에 의해 주변 치아의 치근 흡수가 심하게 일어나거나 낭종 등이 문제를 일으키고 있는 상황에서, 견치를 제 위치로 유도하기 어려운 경우에는 견치의 발거를 고려한다(Fig. 7, 8). 특히 교정치료를 위해 소구치 발거가 필요한 어린이에게서 견인이 어려운 견치의 매복 상황이 발생하면 소구치 대신 견치 발거를 고려할 수 있다.
An 11-year-old girl had transposed impaction of both maxillary canines (A, B).
After removal of the canines, the prognosis for the incisors and alignment seems good (A, B).
4) 외과적 노출
종종 유치의 조기 상실 후 치유 과정에서 잇몸이 두꺼워져 영구치가 그 안에 갇혀서 맹출을 못 하는 경우가 있다. 매복치의 위치가 좋고 공간이 충분하며 치아가 잇몸에서 촉진되는 경우에 치아를 노출시켜 맹출을 촉진시킨다.
매복된 치아가 조금 더 깊이 있는 경우에는 단순히 노출시키는 것만으로 치아의 맹출이 일어나지 않을 수 있다. 치아가 맹출하는 속도보다 잇몸의 치유 속도가 빠르기 때문이다[18]. 이 경우 노출된 치아가 다시 잇몸으로 덮이는 것을 방지하기 위해 외과적 팩(surgical pack)을 적용할 수 있다.
5) 교정적 견인
외과적 노출만으로 치아의 맹출이 진행되지 않거나 치아가 정상 위치에서 많이 벗어난 경우 치아에 직접 힘을 가해 교정적으로 이동시켜야 한다. 치아에 교정력을 가하기 위해 버튼이라고 하는 장치를 붙이게 되는데, 매복된 치아를 노출시키기 위한 수술 과정이 동반된다.
수술법은 크게 open technique과 closed technique의 두 가지로 구분된다. Open technique은 수술적으로 치아를 구강 내 노출시키는 것이며, 추후 교정치료는 치아가 구강내에서 보이는 상태에서 진행된다. Closed technique은 잇몸을 열어 치아를 노출시킨 후 버튼을 붙인 후 다시 잇몸을 재위치 시켜서 덮고 봉합해 주는 방법이다. 매복된 치아의 버튼에 연결된 철사가 구강 내로 노출되어 이를 통해 교정치료를 시행한다. 각각의 방법은 장단점과 적응증이 있으며, 치과의사의 판단에 의해 적절한 수술법을 선택하게 된다[19].
다음으로 협측과 구개측 매복의 교정적 견인 치료 증례를 소개한다.
(1) 협측 매복의 교정적 견인에 의한 치료
첫 번째 증례는 매복된 상악 좌측 견치를 견인하기 위해 open technique을 사용한 증례이다. 초진 시 좌측 상악 견치는 측절치 치근으로 기울어 있었고, 협측으로 매복되어 있었다. 매복된 위치가 깊지 않았기 때문에 상방의 잇몸을 제거하고 버튼을 부착하였다. 가철식 교정장치(removable orthodontic appliance)에 고무줄을 걸게 하여 매복된 치아를 먼저 뒤쪽으로 견인한 후(Fig. 9), 치아가 측절치 치근에서 벗어난 이후에는 통상적인 고정성 교정치료로 배열하여 치료를 마무리하였다(Fig. 10).
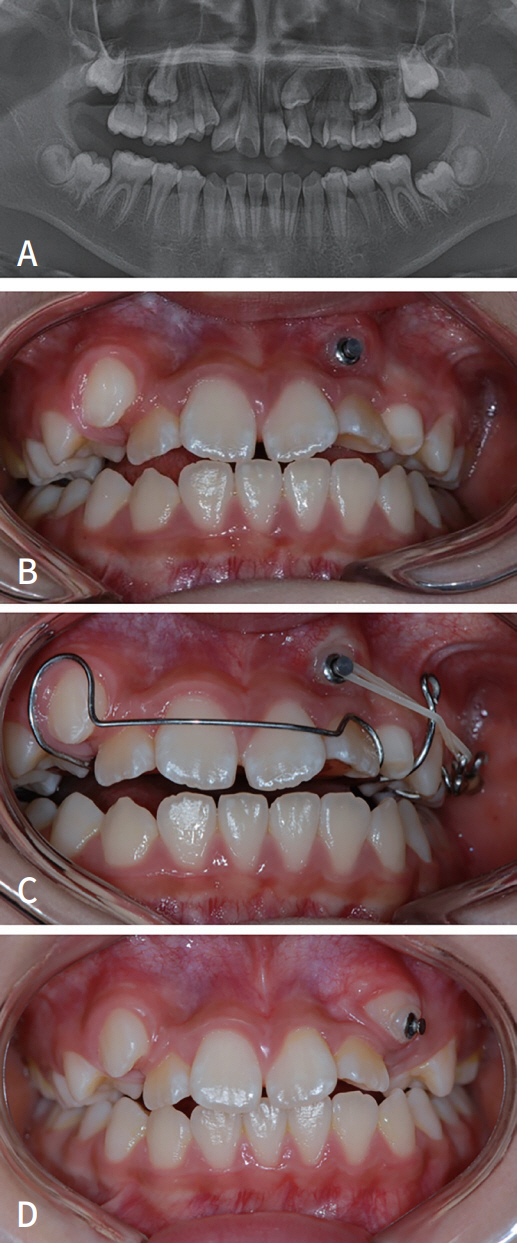
An open technique was used for orthodontic traction of the impacted left maxillary canine (A - D).
After the impacted teeth deviated from the root of the lateral incisor, alignment was achieved with conventional fixed orthodontic treatment (A - C).
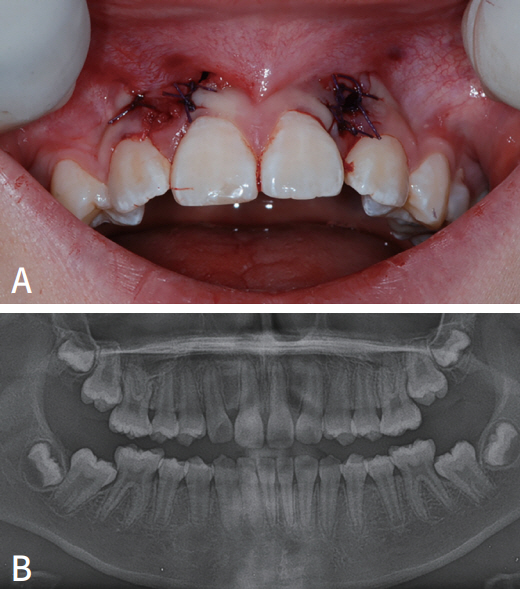
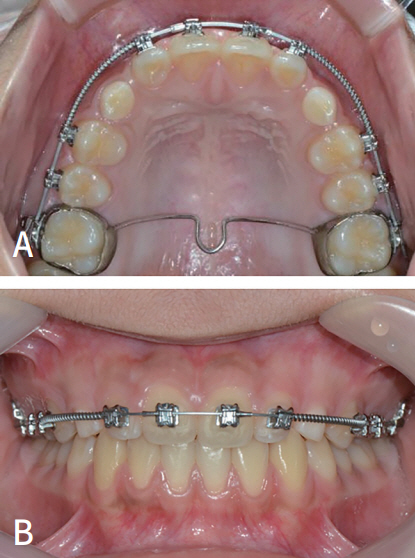
두 번째 증례는 매복된 양측 상악 견치를 견인하기 위해 closed technique을 사용하였다. 초진 시 양측 상악 견치가 측절치 치근과 겹쳐 있는 상황이었다. 측절치 치근흡수를 방지하기 위해 뒤쪽으로 견인이 필요한 상황이었다.
잇몸을 열어 치아를 노출시킨 후 버튼을 부착하고, 잇몸을 다시 재위치 시키고 봉합하였다. 버튼에 연결되어 잇몸을 통해 노출된 철사를 통해 교정력을 가하게 된다. 견인을 위한 고정식 장치를 부착하고 고무줄을 걸어 뒤쪽으로 원심 및 협측으로 견인한다(Fig. 11). 2달 후 사진처럼 치아의 위치가 얕아지면 자연스럽게 치아가 구강내로 노출될 수 있다. 6개월 정도의 견인 후 견치의 위치는 측절치를 벗어나 안전한 위치로 이동되었다(Fig. 12). 이후 통상적인 교정치료로 치료를 마무리하였다(Fig. 13).
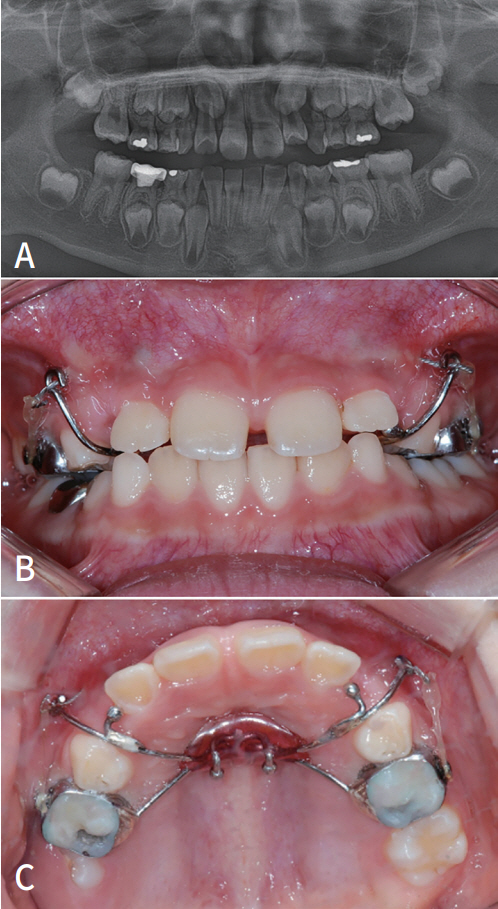
A 9-year-old girl had a buccally impacted canine. The cusp of the canine had passed severely medial to the midline of the lateral incisor (A). Using the guiding wire from the modified Nance holding arch, the direction of traction could be controlled to avoid the blockage of the incisor root (B, C).
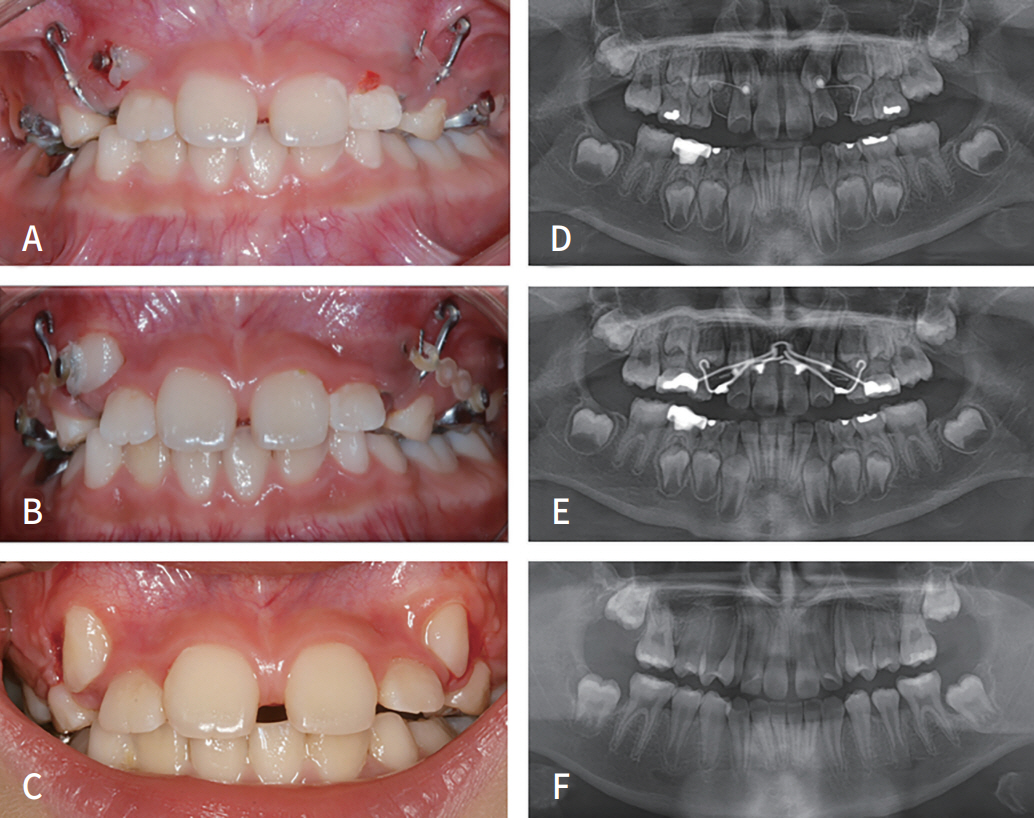
After 2 to 4 months of traction, the impacted teeth could be naturally exposed to the oral cavity (A, B, D, and E). After 6 months of traction, the position of the canines moved beyond the lateral incisors to a safe position (C, F).
Alignment was achieved with conventional fixed orthodontic treatment (A, B).
(2) 구개측 매복의 교정적 견인에 의한 치료
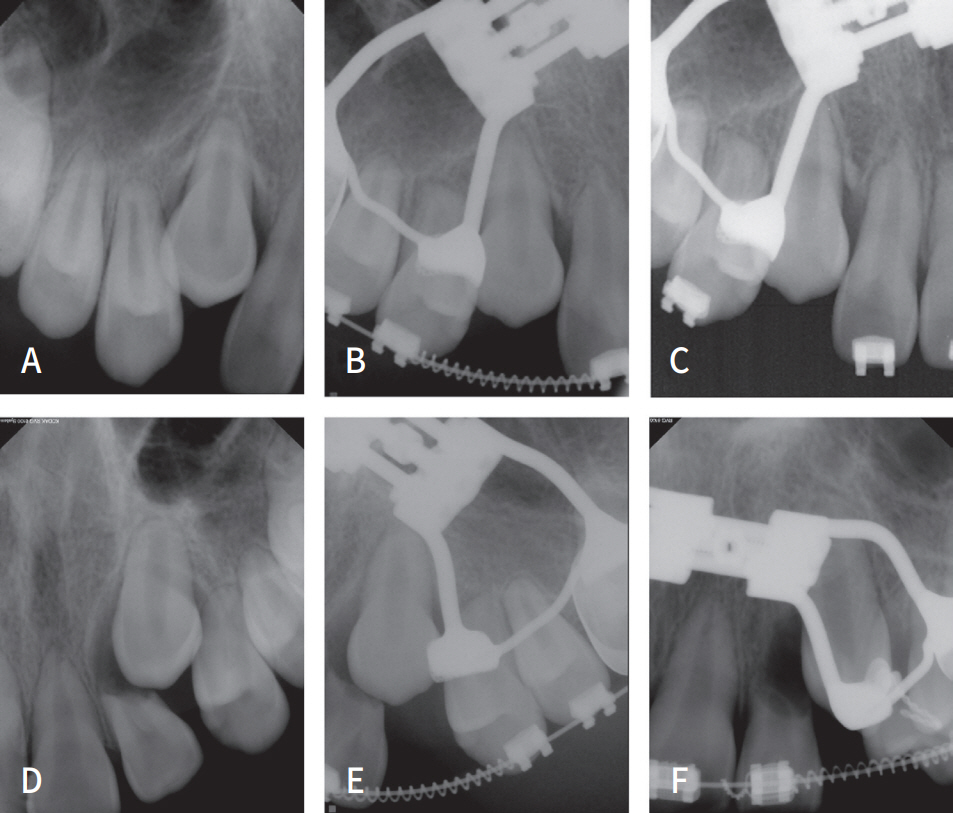
구개측 매복된 견치는 일단 중절치 및 측절치의 치근 흡수를 방지하기 위해 구개의 좀 더 깊은 부위로 견인하는 과정이 선행된다. 먼저 치아를 뒤쪽으로 견인하여 위험한 위치에서 벗어나게 하고, 이 과정에서 치아가 좀 더 드러나서 협측에 장치를 붙일 수 있게 되면 버튼을 추가적으로 붙인 후 치아를 적절히 회전시키면서 협측으로 견인한다(Fig. 14 - 16).
A 12-year-old girl had a palatally displaced canine with incisor root resorption. The impacted canine crown is close to the root of the central incisor (A - C).
Orthodontic traction is first applied in a lingual and vertically downward direction to erupt the tooth into the palate (A). After exposure of the buccal surface of the canine, an additional button is paced on the buccal aspect, and then buccal traction is applied to the buccally placed button (B).
Although the result after completion of traction and alignment was not the best, the patient and her parents were satisfied with the stoppage of the resorption of the central incisor and the repositioning of the canine (A - C).
6) 자가 치아 이식술
매복 견치의 자가 치아 이식술은 주위 해부학적 구조물 때문에 교정적 견인에 의한 치료가 불가할 경우 최종적으로 고려할 수 있는 술식이다(Fig. 17 - 20). 심미적인 관점이나 교합의 측면에서 견치는 다른 어떤 치아보다 중요하기 때문에 자가 치아 이식술이 적극적으로 사용된다. 11 - 12세의 어린이에서 견치 매복이 진단되고 다른 치료 방법이 어려울 경우 치아이식은 좋은 치료법이 된다. 이 나이에는 이식 후 견치의 치수 및 치주조직의 정상적인 치유가 기대된다.
A 14-year-old girl had diastema and prolonged retention of primary canine. Orthodontic traction was difficult because the teeth were impacted close to the nose (A - C).
As the first step in autotransplantation, enough space must be made at the recipient area by an orthodontic treatment before the surgery (A, B).
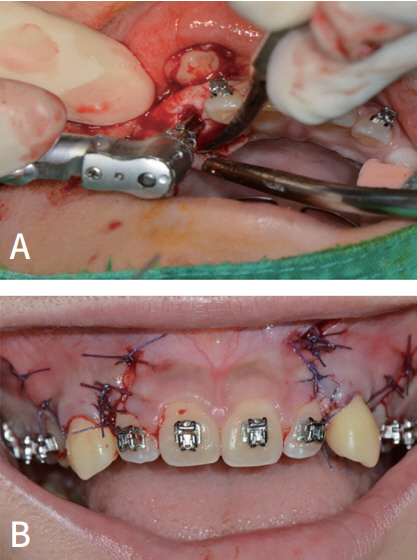
The location of the impacted tooth was confirmed after flap elevation. After the canines were luxated carefully, the recipient site was prepared with an implant drill (A). The impacted canine was carefully removed and placed at the recipient site. The gum was sutured, and the implanted tooth was fixed (B).
Orthodontic treatment was resumed 2 months after autotransplantation (A - C). Although root canal treatment was required in this case, the periodontal ligament healed well, and orthodontic treatment was completed in a relatively short time (D - F).
자가 치아 이식술의 과정을 간단히 살펴보면, 첫 번째 과정은 치아가 이식될 부위(수용부)를 이식될 치아가 들어갈 수 있게 모양을 형성해 주는 것이다. 수용부에 존재하는 유치를 발거하고 추가적으로 뼈를 삭제하여 이식될 치아가 들어갈 수 있도록 충분한 공간을 형성하게 된다. 수용부 형태가 완성되면, 이식될 치아를 손상이 가지 않도록 주의하여 발치한다. 발치한 치아를 수용부에 식립하고, 교정용 철사와 레진을 사용하여 주변 치아에 고정한다. 고정장치는 보통 3 - 4주 정도 유지 후에 제거한다.
치아 이식 후 합병증의 발생 여부를 확인하기 위해 술 후 4주 및 8주 정도에 임상 및 방사선검사를 시행한다. 이식된 치아는 치아 뿌리를 둘러쌓는 조직인 치주인대의 손상이 적을수록 성공률이 높아진다. 합병증으로 감염이나 염증이 발생할 수 있는데, 이는 대부분 이식 후 4 - 8주 내에 나타난다. 합병증이 발생한 경우 근관 치료가 필요할 수 있으며, 예후가 불량할 경우 이식한 치아를 발치해야 할 수도 있다.
이식한 치아가 성공적으로 안착되면 교정치료는 이식 후 3개월 정도 지나면 시작할 수 있다. 견치의 경우 처음부터 좋은 위치로 이식하기가 어려워 수용부를 깊이 형성한 후 견치를 일단 교합되지 않는 상태로 이식한 후, 초기 치유가 완료된 후 교정 치료로 정상 교합위치로 이동시키는 술식을 많이 쓰게 된다.
결론
견치는 상악 치열의 주춧돌(cornerstone)로 불리울 만큼 기능 및 심미적으로 중요한 치아이다. 견치가 매복될 경우 심각한 문제를 초래할 수 있음에도 불구하고 특별한 증상을 나타내는 경우가 드물어, 주변 치아 뿌리의 흡수와 같은 문제를 이미 일으키는 시점에서 발견되는 경우가 많다. 견치의 매복을 늦게 발견할수록 문제는 심각해지고, 이를 치료하기도 어려워진다.
견치가 매복되는 것을 예방하고, 조기에 발견하기 위해 성장기 어린이들은 충치 같은 다른 문제가 없더라도 적어도 6개월에 한 번 이상 치과에 방문하여 치아의 발육 및 맹출 상태를 확인하는 것이 필요하다. 턱뼈 내에서 치아가 발육하고 맹출하는 것은 육안으로 확인할 수 없기 때문에 파노라마 방사선 사진을 주기적으로 촬영하는 것이 추천된다.
매복된 견치가 발견되면, 적절한 방법으로 조기에 개입하여 치료하는 것이 필요하다. 정도가 심하지 않을 때에는 악궁 확장, 유견치 발거, 외과적 노출만으로도 정상적인 맹출을 기대할 수 있다. 하지만 맹출로가 정상에서 많이 벗어나거나 주변 치아에 위해를 가하고 있을 때에는 외과적 노출 후 교정적 견인을 시행해야 할 수도 있다. 이러한 치료 과정은 긴 시간과 비용이 소모되는 힘든 과정이지만, 교합과 심미적인 관점에서 소중한 견치를 보존할 수 있다는 면에서 충분한 가치가 있는 치료 과정이다. 치아의 위치가 교정적 견인을 할 수 없을 정도로 좋지 않은 경우 자가 치아 이식을 고려해 볼 수 있다. 자가치아 이식은 난이도가 높으며 매번 성공하는 것은 아니지만, 견치를 보존하기 위한 최후의 수단으로 여겨진다. 다른 치료방법이 실패하거나, 자가 치아 이식도 불가능할 만큼 견치를 위한 공간이 없을 경우 매복된 견치를 발치해야 한다. 이후 자발적인 배열을 기대해 보거나, 공간을 성장기까지 유지한 후 성인기에 임플란트를 시행한다.
Notes
Conflict of Interest
The authors have no potential conflicts of interest to disclose.