Comparison of Shear Bond Strength in Novel Calcium Silicate-Based Materials to Composite Resin
Article information

Abstract
The purpose of this study was to evaluate whether the newly introduced calcium silicate-based materials with fast-setting properties could be appropriately used as basement materials in indirect pulp treatment (IPT). This was performed by quantifying the durability of adhesion between the material and composite resin, measured by the shear bond strength (SBS). Five calcium silicate-based materials, TheraCal LC® (TLC), TheraCal PT® (TPT), TheraBase® (TB), Well-Root™ PT (WPT), and Endocem® MTA (EMTA), as well as two glass ionomer-based materials, Fuji II and Fuji II LC, were included. Specimens containing these materials were manufactured and bonded to composite resin with a universal adhesive applied in self-etch mode. The SBS values and failure modes were recorded, and the mean SBSs of the materials were compared. Both TPT and TB exhibited SBS values that were similar to TLC, while both WPT and EMTA appeared to have statistically lower SBS values. Mixed failure was commonly observed in TLC and TPT, while all WPT and EMTA samples showed cohesive failure. In comparison with TLC and TPT, more samples with cohesive failure were observed in TB, implying that this material forms a stronger bond with composite resin. Together with the ability of TB to chemically bind to dentin due to its 10-methacryloyloxydecyl dihydrogen phosphate component, TB seems to be a promising material for IPT within the limitations of this in vitro study.
Introduction
Recent literature recommends indirect pulp treatment (IPT) over other forms of vital pulp therapy in primary teeth with deep caries [1,2]. IPT also demonstrates promising results in permanent molars, as the three-year survival rate of indirect pulp treatment was reported to be 96.0% in primary molars and 93.0% in permanent teeth [3]. Calcium hydroxide has long been used as the medicament for IPT; however, due to its hydrolytic properties, it has been mostly replaced by calcium silicatebased materials [4]. For the clinical success of IPT, the basement material should adequately seal dentin and have sufficient bond strength with the overlying composite resin restoration [5].
Since its introduction as the first form of calcium silicate-based material in dentistry, mineral trioxide aggregate (MTA) has become one of the most versatile materials for vital pulp therapy [6]. However, several drawbacks limit the use of MTA in clinical situations. Apart from the long setting time, discoloration, difficult manipulation, and low initial compressive and flexural strength [7], the inconsistency arising from its cumbersome mixing process makes this material often unfavorable for clinicians. MTA also shows low bond strength to dentin [8], which is disadvantageous when considering it as a basement material for IPT [5].
Calcium silicate-based materials have been constantly developed to overcome the shortcomings of traditional MTAs, particularly to reduce the setting time. This was achieved by adding hydration accelerators, such as Biodentine ™ (Septodont, Saint-Maur-des-Fosses, France), or light-curable resin monomers, like TheraCal LC® [TLC] (Bisco Inc., Schaumburg, IL, USA). In Endocem® MTA [EMTA] (Maruchi, Wonju, Korea), the setting time was shortened by using small pozzolan cement particles [9]. All of these materials are known to have high clinical efficacy as basement materials in IPT [10,11]. However, both Biodentine™ and EMTA have insufficient bond strength to composite resin; therefore, in terms of bond strength, only TLC can be recommended for IPT [12-14].
In a later development in 2019, TheraCal PT® [TPT] (Bisco Inc.), a dual-cured resin-modified calcium silicate, was developed as a successor to TLC. It is primarily indicated for pulpotomies, but it can also be used as pulp capping or basement material. This material is known to be more biocompatible than TLC [15-17], in which unpolymerized resin monomers can cause harm to the healing pulp [18]. A recent study reported that the one-year clinical success rate of IPT in primary molars when using TPT was 93.9% [19]. Recently, TheraBase® [TB] (Bisco Inc.), a novel dual-cured resin-modified calcium silicate, was introduced to the market. This material is recommended for use as a basement material during IPT, and it can bind directly to dentin due to its 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP) component.
Meanwhile, premixed calcium silicate-based materials were developed to improve the handling properties of MTA. Endocem® MTA premixed (Maruchi) and Well-Root™ PT [WPT] (Vericom Co., Chuncheon, Korea) are notable representative examples. These materials are provided in injectable forms, which do not require a separate mixing process and are set in the presence of moisture. WPT has been soundly demonstrated to have good sealing properties and adequate compressive strength as a basement material [20].
To the best of our knowledge, few studies have reported the shear bond strength (SBS) of composite resin to newly developed calcium silicate-based materials, such as TPT, TB, and WPT. Therefore, this study aimed to measure and compare the mean SBS values of various calcium silicate-based materials to composite resin, thereby evaluating whether these materials can be suitably applied as basement materials. The null hypothesis of this study was that there were no differences in the mean SBS values among the aforementioned materials to composite resin.
Materials and Methods
A total of 5 calcium silicate-based materials and 2 glass ionomer-based materials were included in the study. Calcium silicate-based materials included TLC, TPT, TB, WPT, and EMTA. Fuji II® [GI] (GC Co., Tokyo, Japan) and Fuji II LC® [RMGI] (GC Co.) were selected for the glass ionomer-based materials. The descriptive information about each material is shown in Table 1.

Detailed information about the materials used in the study
1. Sample preparation
A total of 84 identical cylindrical blocks, each measuring 25.0 mm in diameter and 7.8 mm in height, were fabricated with a self-curing acrylic resin, Ortho-Jet™ (Lang Dental Co., Wheeling, IL, USA). Each block had a central cylindrical notch measuring 10.0 mm in diameter and 1.8 mm in height (Fig. 1). Retention grooves were prepared in the inner walls of the notch with the FG-37 inverted cone carbide bur to prevent dislodgement of the material during shear bond testing. The samples were randomly allocated into one of the 7 groups, with 12 samples fabricated for each group. Materials that required manual mixing were prepared according to each manufacturer’s instructions and then moved into each of the cylindrical notches. Premixed or auto-mixing materials were directly filled into each of the cylindrical notches. According to its manufacturer’s instructions, WPT sets in the presence of moisture from the surrounding environment. However, due to the absence of moisture in the acrylic resin block, a drop of distilled water from the pipette of Ortho-JetTM liquid (Lang Dental Co.) was dropped into the cylindrical notch prior to filling.
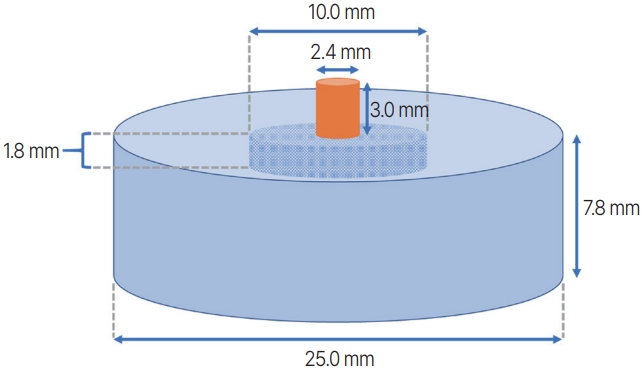
Schematic diagram of the sample used in the study. Each material was filled in a cylindrical notch, with a diameter of 10.0 mm and a height of 1.8 mm, within a cylindrical block fabricated from acrylic resin, with a diameter of 25.0 mm and a height of 7.8 mm. A composite resin mold with a diameter of 2.4 mm and a height of 3.0 mm was bonded to the material surface, as shown in the diagram.
After the placement of each material, a 10-mm-wide celluloid strip was gently placed on top and covered with a microscopic slide to create a homogeneous surface. Materials that contained resin monomers were lightcured with an LED curing unit, Valo® (Ultradent, South Jordan, UT, USA), according to each manufacturer’s instructions. Other chemically setting materials were cured during the setting time specified in each manufacturer’s instructions. Any excess material was removed carefully with a scalpel blade to cause as minimal as possible damage to the material surface. All samples were stored for 24 hours in 30 - 50% humidity at a room temperature of 25°C.
2. Restorative procedure
Single Bond Universal (3M ESPE, St. Paul, MN, USA) was applied in self-etch mode. Using a microbrush, the rubbing motion of the adhesive was conducted for 20 seconds. The adhesive was then dried with a waterfree airway syringe and light-cured for 20 seconds with Valo® (Ultradent) with an intensity of 1000 mW/cm2 at a distance of 3.0 mm. This whole process was performed twice, since the double-layer application of universal adhesives strengthens the bond of composite resin to dentin, as recommended when using universal adhesives [21]. The Ultradent Bonding Jig was used to clamp the sample to the composite resin. Light-Core™ (Bisco Inc.), a light-cured core build-up composite resin, was filled into the cylindrical bonding mold inserts with a diameter of 2.4 mm and a height of 3.0 mm and light-cured for 20 seconds with Valo® (Ultradent) with an intensity of 1000 mW/cm2 at a distance of 3.0 mm.
3. Shear bond strength test
The SBS of each material to composite resin was measured by the Shear Bond Tester (Bisco Inc.). Each sample was held in the sample-holding clamp with the resinbonded surface of the sample flush with the top side of the clamp. A test cradle containing a test blade was placed over the sample-holding clamp to position the half-rounded notch of the test blade in contact with the base of the composite resin. An increasing shear force was applied by a crosshead speed set at 1.0 mm/min. By dividing the area of the bonded surface (4.45 mm2), the load at failure recorded in N was converted into MPa.
4. Failure mode analysis
After the shear bond test, the fractured surface of each sample was carefully examined by a single examiner under the Olympus SZX7 stereomicroscope at 40× magnification. Each failure mode was classified into cohesive within the tested material, cohesive within composite resin, adhesive (at the interface between the tested material and composite resin), or mixed (a combination of cohesive and adhesive failure).
5. Statistical analysis
The normality of the SBS values in each group was evaluated by the Shapiro-Wilk test. Since the values in each group followed normality, parametric tests were performed. One-way ANOVA was used to determine whether there were any differences between the mean SBSs between groups. Since the values between groups showed unequal variance according to Levene’s test, intergroup post hoc comparisons were performed by Dunnett’s T3 test. Using SPSS version 26.0 (SPSS Inc., Chicago, IL, USA), all statistical analyses were carried out with an alpha significance threshold of 0.05.
Results
The SBS of the TheraCal group (TLC, TPT, and TB) was significantly higher than that of the MTA group (WPT, EMTA). GI presented significantly lower SBS than TLC and TB but did not differ significantly from TPT. RMGI showed the highest mean SBS but did not differ significantly from those of the TheraCal group (TLC, TPT, and TB) (Table 2, Fig. 2).

Shear bond strength of the materials used in the study
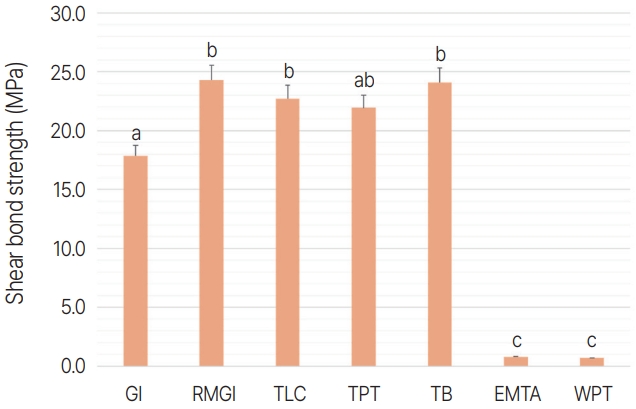
Mean shear bond strengths of composite resin to the materials used in the study. Different lower-case alphabets indicate statistically significant differences in the mean shear bond strength. Post-hoc comparisons were conducted by Dunnett’s T3 test after a one-way ANOVA test (p < 0.05).
GI: glass ionomer; RMGI: resin-modified glass ionomer; TLC: TheraCal LC®; TPT: TheraCal PT®; TB: TheraBase®; EMTA: Endocem ® MTA; WPT: Well-Root™ PT.
The predominant failure mode of both TLC and TPT was mixed failure, while cohesive failure within the tested material was more frequently observed in TB. All specimens of WPT and EMTA showed cohesive failure within the tested material. Cohesive failure within the tested material also prevailed in GI, while adhesive failure was the most common failure mode in RMGI (Fig. 3).
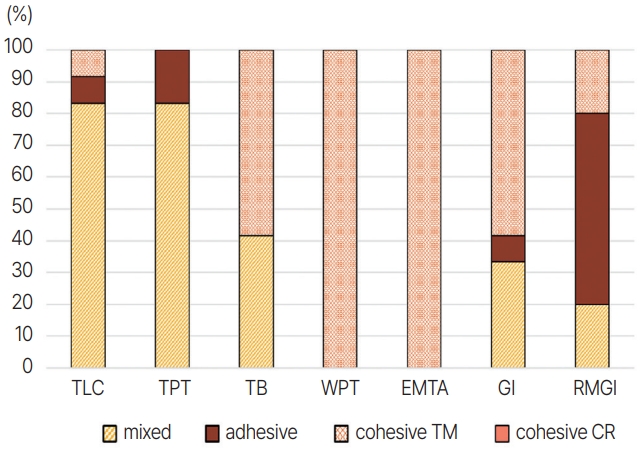
Distribution of the failure modes (%) of the materials used in the study.
TLC: TheraCal LC®; TPT: TheraCal PT®; TB: TheraBase®; WPT: Well-Root™ PT; EMTA: Endocem® MTA; GI: glass ionomer; RMGI: resin-modified glass ionomer; cohesive TM: cohesive failure within the tested material; cohesive CR: cohesive failure within composite resin.
Discussion
A durable bond between the basement material and the overlying composite resin restoration during IPT is necessary for its clinical success [5]. A range of 17 - 20 MPa of dentin bond strength to composite resin is required to withstand its polymerization shrinkage stress [22]. Of the calcium silicate-based materials studied, TLC, TPT, and TB fulfilled this criterion. Other calcium silicate-based materials, such as WPT and EMTA, failed to reach an adequate bond strength to composite resin. This may be primarily due to the low initial bulk strength of these materials, as in Biodentine™ [23], which can be supported by the fact that all of the specimens showed cohesive failure within the tested material. Secondly, the methacrylate monomers in the TheraCal group (TLC, TPT, and TB) can contribute to the adhesion by forming a chemical bond with the adhesive, as shown by the difference in the SBS between GI and RMGI.
The SBS of TPT did not differ significantly from that of TLC. This was in accordance with a similar in vitro study comparing the SBS of TPT, TLC, and Biodentine™ [17]. However, different results were obtained by another study that compared the micro SBS of the same materials [24], where TPT showed significantly higher micro SBS than TLC and Biodentine™.
Albeit not significantly different from the results of TLC and TPT, TB resulted in the highest mean SBS of the studied materials. Also, more samples of TB showed cohesive failure within the tested material (> 60%), while mixed failure was observed in most of the samples of TLC and TPT (> 90%). A more durable bond will result in cohesive failure of either the calcium silicate-based material or composite resin rather than adhesive or mixed failure, which involves a deterioration of the adhesive layer. In addition, the 10-MDP constituent of TB is expected to contribute to the chemical bond to composite resin.
A similar condition is assumed to appear with EMTA as Biodentine™, in which the full maturation of the material takes at least 2 weeks [23,25]. Unlike the other types of MTAs, the compressive strength of EMTA increases significantly over time. A study comparing the compressive strength of various MTAs according to time revealed that this material reached its maximum compressive strength after 7 days [26]. This implies that fast-setting calcium silicate-based materials may require a prolonged time to reach their maximum physical properties. However, another study showed different results, showing that there were no significant differences in the SBS of Biodentine™ between immediate and delayed (7-day) restoration of composite resin [27].
There has been a lack of studies to date about the bond strength of WPT to composite resin. Studies on other types of premixed calcium silicate-based materials, namely premixed bioceramics, show that these materials have lower SBS than conventional powder-and-liquid mix types [28,29]. Also, moisture from the surrounding environment is needed in the setting process of these materials. In this study, a drop of distilled water was applied before injecting WPT into the cylindrical notch. This could have hindered the setting reaction, especially near the surface. In our experimental setting, dehydration may have occurred during storage, altering the setting reaction of WPT. Covering the surface with a wet cotton pellet might have prevented this, thus leading to more accurate results. Also, a better model resembling the moist environment of dentin, such as using plaster molds, may have been a better alternative [30].
Only the bond strength between the basement material and composite resin was evaluated in this study. Another important factor in the success of IPT is whether the basement material adequately seals the underlying dentin [5]. A weak bond to dentin might cause dislodgement of the material together with its overlying restoration. Although grooves were prepared inside the cylindrical notch for mechanical retention, dislocation of the material from the acrylic resin block was observed in some of the specimens during shear bond testing. The mechanism of adhesion of calcium silicate-based materials to dentin is unknown, but studies suggest that both micromechanical and chemical adhesion play significant roles [8,31]. Tag-like structures impregnated in the underlying dentinal tubules were observed in microscopic images of the interface between Biodentine™ and human dentin [31]. Also, the alkaline nature of hydrated calcium silicates produces a corrosive effect on the exposed collagen fibrils of dentin, thereby allowing minerals from the hydrated calcium silicate to penetrate into intertubular dentin [31,32].
The tested samples containing the calcium silicatebased materials were not human dentin, as acrylic resin blocks were used as an alternative. Due to differences in the interfacial bond strengths of the studied materials to dentin and acrylic resin, the SBS values should be taken into consideration when applying them to a clinical situation. Of the materials used in this study, TB seems to form a more solid bond with dentin due to its 10-MDP composition. Further studies are needed comparing the SBS of calcium silicate-based materials to dentin to verify this hypothesis.
The surface properties of some specimens of EMTA and WPT were altered during the restorative procedure, particularly when the surface of WPT dissolved or fell off after rubbing it with the bonding agent. According to recent studies, WPT has a higher solubility than those of other calcium silicate-based materials, such as EMTA and RetroMTA (BioMTA, Seoul, Korea) [33,34]. Compared to TLC, in which the solubility value rapidly decreases after setting, WPT appears to have a smaller decrease in its solubility value, persisting over 5% at 7 days after setting [33]. Due to water in Single Bond Universal, the surface of WPT was largely affected. Therefore, in clinical practice, the application of bonding agents to WPT should be carefully done. Other adhesives containing ethanol or acetone as a solvent may be considered, but there are few studies up to date describing the influence of various adhesives on WPT.
A universal bond was applied in self-etch mode during the restorative procedure. The adhesive strategy during restorative procedures in a clinical situation may be a matter of concern since it can influence the bond strength between the adherents. Bayrak et al. [35] and Tunç et al. [36] reported that the bond strength to white MTA was significantly higher when using etch-andrinse adhesives compared to self-etch adhesives, while Neelakantan et al. [37] and Shin et al. [38] recommended using one-step self-etch adhesives over white MTA. In the meantime, a comparative study of the bond strength of RetroMTA (BioMTA) to composite resin showed similar bond strength whether the universal bond was applied in etch-and-rinse or in self-etch mode [39]. Studies also reveal conflicting outcomes with TLC [40,41], suggesting that the adhesive strategy may not influence the bond strength in most of the calcium silicate-based materials to composite resin. According to a recent metaanalysis, the etch-and-rinse mode is preferred over the self-etch mode both in MTA and TLC [42]. However, only four studies of TLC were included; thus, more studies should be carried out to confirm the influence of adhesive strategy on the SBS of TLC to composite resin. As far as we know, there are no studies comparing the SBSs of either TPT, TB, or WPT to composite resin depending on the adhesive strategy. Further studies are expected to be carried out to reveal any relevance between the adhesive strategy and the bond strengths of these materials to composite resin.
Conclusion
Firm adhesion between the basement material and the overlying composite resin is a vital factor in the success of IPT. From the perspective of bond strength, TLC, TPT, and TB all appear to be suitable for basement materials during IPT. In contrast, both WPT and EMTA are relatively weak materials; therefore, they are inappropriate for immediate composite resin restoration in IPT. Within the limitations of this in vitro study, which will be addressed in future research, TB seems to be a promising material that has good adhesive characteristics that lead to better SBS.
Notes
Conflict of Interest
The authors have no potential conflicts of interest to disclose.