Prevalence of Dental Anomalies in Patients with Non-syndromic Cleft Lip with or without Cleft Palate
Article information

Trans Abstract
This study aimed to assess the prevalence and distribution pattern of dental anomalies in the permanent teeth of patients with non-syndromic cleft lip with or without cleft palate. Additionally, it aimed to compare differences in dental anomalies between cleft and non-cleft areas, considering gender and cleft phenotype. Panoramic radiographs of 164 patients diagnosed with non-syndromic orofacial clefts were retrospectively analyzed by a single examiner to confirm dental anomalies. The dental anomalies investigated included tooth agenesis, supernumerary teeth, microdontia, rotation, ectopic eruption, and enamel hypoplasia. Cleft phenotypes were categorized into 7 types based on medical and dental records. A significantly higher prevalence of supernumerary teeth was observed in males than females within non-cleft areas (p = 0.017), with no significant differences in other dental anomalies. In non-cleft area, patients with cleft palate exhibited a high prevalence of tooth agenesis (p < 0.0001) and microdontia (p = 0.012) compared to other cleft phenotypes. Maxillary incisor rotation was closely associated with adjacent tooth agenesis in unilateral cleft lip and palate cases (p = 0.034). This study suggests that the additional subphenotype based on dental anomalies in patients with orofacial cleft may serve as applicable clinical markers.
Introduction
Cleft lip with or without cleft palate (CL/P) is the most frequent congenital head and neck malformation, manifesting as either non-syndromic, as an isolated feature, or syndromic, accompanied by other congenital defects [1,2]. The epidemiology of CL/P varies depending on ethnicity, geographic region, socioeconomic status, maternal age, and fetal exposure to teratogenic agents [3]. Notably, orofacial clefts have an estimated prevalence of 11.09 per 10,000 live births in Korea, contrasting with 3.3 per 10,000 live births worldwide [4,5].
The discontinuity of the lip or palate in CL/P arises from the noncoalescence of embryonic facial processes between the 4th and 10th weeks of intrauterine life [6,7]. The etiology of orofacial clefts is complex, involving genetic factors with variable interactions between environmental influences [8]. Various studies have explored environmental contributors, such as maternal smoking, drug use, and folic acid deficiency [2,9,10]. The list of associated genes has undergone rapid expansion from the first reported TGF-α to a number of genes such as MSX1, IRF6, and PAX7 [11-13].
Dental anomalies linked to genetic or environmental factors are prevalent in patients with CL/P, comprising anomalies in tooth number, shape, size, structure, and position. Tooth agenesis is the most prominent dental anomaly, followed by supernumerary teeth [14,15]. The incidence of dental anomalies is higher in individuals with orofacial clefts compared with the general population, with the severity of anomalies often correlating with cleft severity. Some studies have indicated that teeth outside the cleft area have a higher likelihood of exhibiting dental anomalies, relative to individuals without clefts [6,16,17].
Since some dental anomalies may lead to complex circumstances such as edentulous spaces, it should be determined whether to treat such spaces with orthodontics or prosthetic restorations such as the crown, bridge, or implant. Furthermore, a multidisciplinary treatment plan is essential owing to the concurrence of multiple anomalies. Understanding the prevalence and emergence patterns of dental anomalies in patients with clefts plays a vital role for pediatric dentists, enabling them to develop long-term treatment plans and improve prognosis.
Previous studies have reported the genetic relations as clinical markers between dental anomalies and cleft phenotypes, supported by the suggestion that genetic alterations in clefts can hinder the odontogenesis process by changing the dental lamina signaling pathway, resulting in dental anomalies [17-19]. Since such insights could aid in understanding developmental mechanisms and potentially lead to novel cleft classification methods based on dental anomalies, the analysis of the prevalence and characteristics of dental anomalies associated with cleft types may be meaningful.
Based on the clinical applicability of dental anomalies in clefts, numerous studies have investigated variations in anomalies among cleft types across different ethnic and geographic backgrounds [7,14,15,17,18]. However, few have studied the dental anomalies in cleft area compared to non-cleft area by different cleft phenotypes. Additionally, research focused on Korean patients remains limited. Therefore, the present study aimed to analyze the frequency and emergence patterns of dental anomalies in the permanent teeth of patients with non-syndromic CL/P, specifically comparing cleft and noncleft areas according to gender and cleft type.
Materials and Methods
This retrospective study was carried out with the approval of the Institutional Review Board of Asan Medical Center (IRB No. 2023-1039).
1. Study subjects
In total, 392 patients aged 6 - 17 who visited the Pediatric Dentistry department of Asan Medical Center between January 2013 and December 2022 were enrolled in this study. These patients had undergone panoramic radiographs due to a cleft diagnosis. The inclusion criteria included patients whose initial panoramic radiograph was taken before secondary alveolar bone grafting to rule out the possibility of dental anomalies caused by the iatrogenic influences of these surgery. The exclusion criteria were as follows: (1) patients under 6 years of age. Since dental anomalies in cleft patients were primarily found in maxillary incisors near the cleft area, 6 years old was set as the minimum age to ensure the complete crown calcification of permanent incisors (n = 78); (2) patients diagnosed with syndromes (n = 5); (3) patients lacking sufficient medical records or dental records, including patients whose panoramic radiographs were not taken serially and who did not take panoramic radiographs after the age of 11 to clearly differentiate the premolar agenesis (n = 111); (4) patients with prior permanent tooth extractions (n = 1); (5) patients with a history of orthodontic or prosthodontic treatment (n = 29); and (6) cases with poor-quality panoramic radiographs (n = 4). Based on these criteria, 164 patients were included in this study.
2. Study design
1) Data acquisition
Dental and medical records were analyzed to determine patient gender and cleft type. Among the panoramic radiographs before and after second alveolar bone grafting, the pre-surgery panorama was mainly examined in this study. Periapical radiographs and dental computed tomography, when available in radiographic records, were used for precise evaluations. Dental records were assessed to eliminate the possibility of permanent tooth extraction or premature tooth loss.
Cleft phenotypes were determined based on clinical records and dental radiograph confirmation, resulting in 7 phenotype groups: unilateral left cleft lip (LCL), unilateral right cleft lip (RCL), bilateral cleft lip (BCL), unilateral left cleft lip and palate (LCLP), unilateral right cleft lip and palate (RCLP), bilateral cleft lip and palate (BCLP), and cleft palate (CP).
2) Radiographic assessment of dental anomalies
A single examiner who is training in the pediatric dentistry assessed radiographs with acceptable contrast, density, and sharpness using PetaVision for Clinics version 2.0 (Asan Medical Center, Seoul, Korea), developed as an anonymized image viewer. Third molars and primary teeth were excluded from this study. Data were recorded based on the FDI system, and cleft and non-cleft areas were categorized. Cleft areas included the area adjacent to the cleft side, encompassing the maxillary central incisors, lateral incisors, and canines. Non-cleft areas comprised the remaining region. In the maxillary area, both sides of the premolars, molars, and incisors of the contralateral side in cases of unilateral clefts were included. In the mandibular area, incisors, premolars, and molars on both sides were included. Subjects were excluded if a definite assessment proved difficult. Evaluated dental anomalies were defined as follows:
(1) Tooth agenesis: The absence of a tooth or tooth germ on radiographs, resulting in incomplete dental arch development. Agenesis of premolars was determined if the contralateral premolar was present or if second molar tooth buds were visible, as they form after the premolars. In order to precisely determine the premolar agenesis, all panoramic radiographs taken after the initial panorama were examined. Initial panoramic radiographs were taken between the ages of 6 and 13, and the most recent panoramic radiographs were taken between the ages of 11 and 17. The average time interval between panoramic radiographs was 5.4 years.
(2) Supernumerary teeth: Identification of additional tooth germ calcification beyond normal dental series development on radiographs in any dental arch region [20]. In the cleft area, any additional tooth positioned mesially or distally to the cleft area in the presence of a lateral incisor was considered. The tooth selected as the supernumerary tooth was smaller or underdeveloped compared with the adjacent tooth.
(3) Microdontia: A tooth appearing smaller than expected in shape, including conical, peg-shaped, or with a tapered crown, fails to fill its dental arch space. A tooth appearing smaller than its contralateral homolog or the corresponding tooth in the opposing arch [21]. A tooth which is 40% or more smaller than its antimere if the judgement is uncertain.
(4) Rotation: A tooth rotated more than 45 degrees around its longitudinal axis, determined only after full eruption [22].
(5) Ectopic eruption: Eruption of a tooth in an abnormal location. Since this study investigated pan-oramic radiographs as a basis, the following ectopic eruptions were examined: ectopic eruption of the maxillary first permanent molar, which shows abnormal resorption of adjacent primary teeth [23]. transposition that a permanent tooth is located in the position where another permanent tooth should be occupied [24].
(6) Enamel hypoplasia: Dental enamel showing either surface loss or breaks in continuity with evident radiolucency in panoramic radiographs, distinguishable from dental caries. Dental records and available periapical radiographs were compared with panoramic radiographs if the judgement was uncertain.
3. Statistical analysis
SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) was used to conduct statistical analysis, using a significance level of α = 0.05. Results were organized in terms of frequency and percentages for descriptive purposes. To avoid inter-examiner differences, a single examiner evaluated dental anomalies. Intra-examiner reliability was assessed by the same examiner re-evaluating a random sample of 20 sets with a 2-week interval, with Cohen’s Kappa tests performed. Standard Pearson chi-square tests or Fisher’s exact tests were used for comparisons of dental anomalies based on gender and cleft phenotype. Additionally, Fisher’s exact tests were used for single-tooth comparisons in each dental anomaly, with quadrant analysis used for tooth agenesis, and correlation analysis also applied for each dental anomaly.
Results
The results of Cohen’s Kappa tests revealed consistently high intra-examiner reliability, with tooth agenesis, supernumerary teeth, and rotation showing perfect agreement. Additionally, microdontia, ectopic eruption, and enamel hypoplasia showed almost perfect agreement, with coefficients of 0.886, 0.857, and 0.827, respectively.
1. Subject and dental anomaly distributions
In total, 164 subjects were included in this study, with 111 and 53 being male (67.68%) and female (32.32%), respectively (Fig. 1). Notably, the most common cleft phenotype for both genders was LCL, with 35 (31.53%) and 17 (32.07%) male and female subjects exhibiting this phenotype, respectively, followed by RCL and LCLP. CP was the least common phenotype for both genders. Among unilateral clefts, the left side was more affected than the right side in cleft lip cases (31.70% for LCL and 23.17% for RCL) and cleft lip and palate cases (14.02% for LCLP and 10.36% for RCLP).
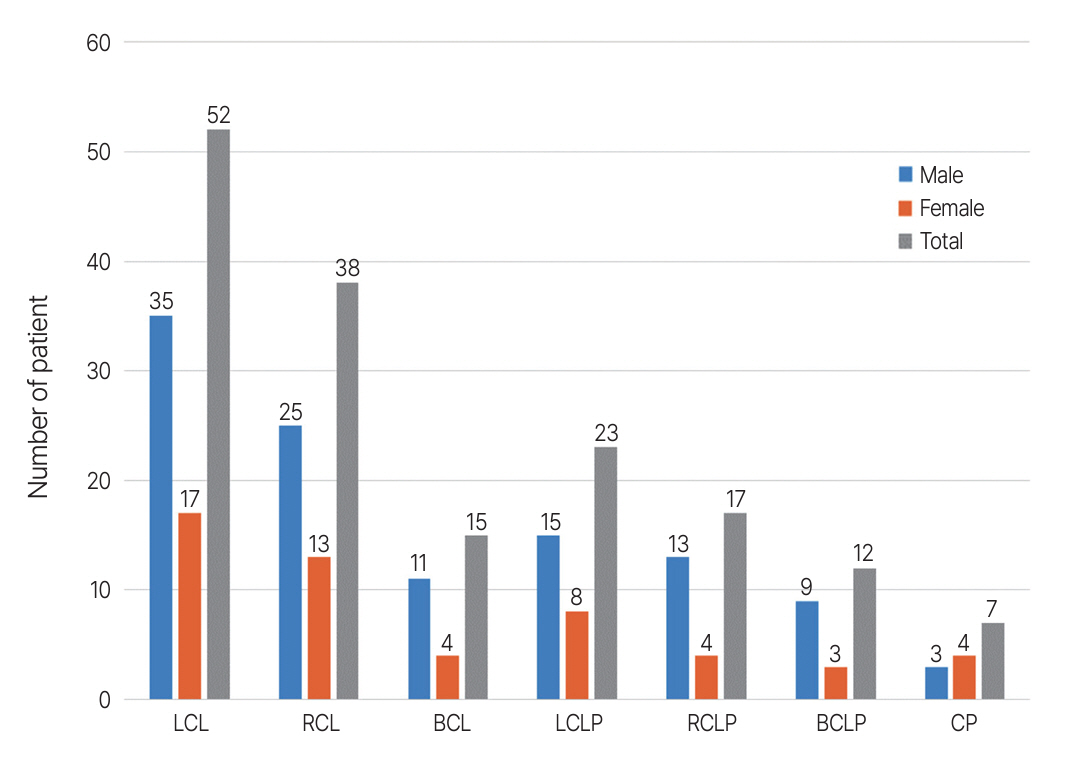
Study subject distribution based on gender and cleft phenotypes.
LCL: unilateral left cleft lip; RCL: unilateral right cleft lip; BCL: bilateral cleft lip; LCLP: unilateral left cleft lip and palate; RCLP: unilateral right cleft lip and palate; BCLP: bilateral cleft lip and palate; CP: cleft palate.
Out of the 164 subjects, 161 subjects (98.17%) exhibited at least 1 dental anomaly (Fig. 2). Maxillary incisor rotation was the most frequent dental anomaly overall, with 117 subjects exhibiting this anomaly (71.34%), followed by microdontia (67.07%) and tooth agenesis (42.68%). Similarly, in male subjects, rotation was the most common dental anomaly (76.57%), followed by microdontia (67.56%) and tooth agenesis (38.73%). In female subjects, microdontia was the most common anomaly (66.03%), followed by rotation (58.49%) and tooth agenesis (50.94%).
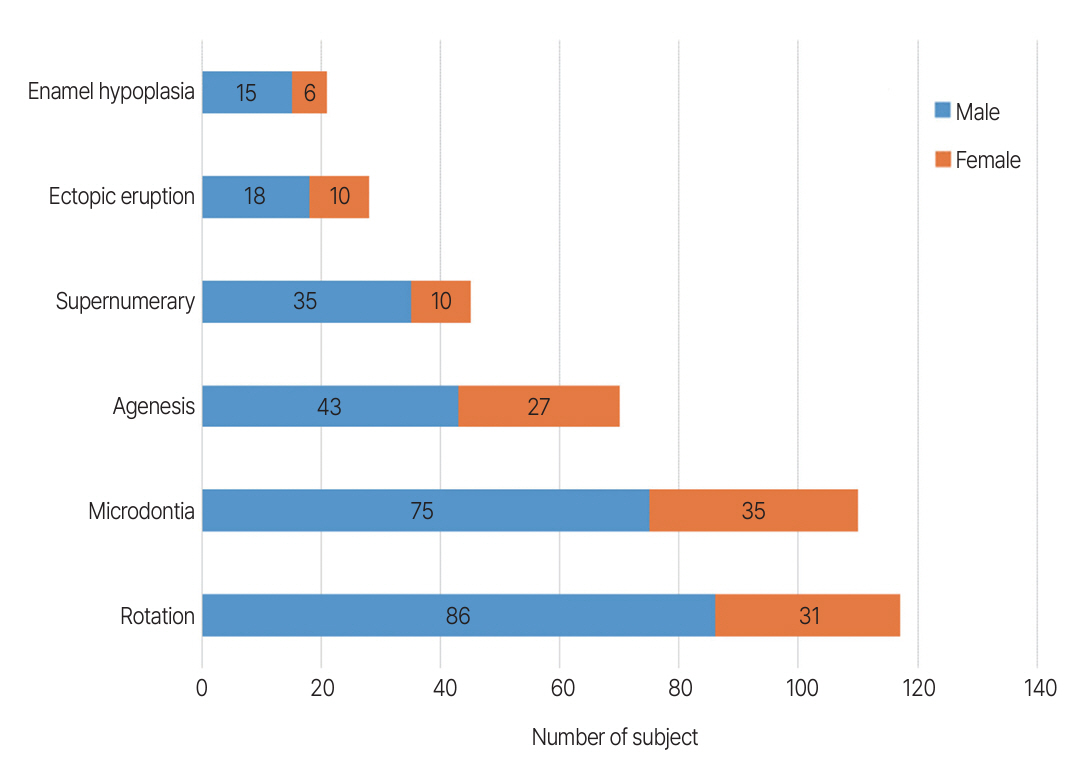
Dental anomaly distributions according to gender.
2. Comparison based on gender and cleft phenotype
In non-cleft areas, a significantly higher prevalence of supernumerary teeth was observed in males than females (p = 0.017), although there were no significant differences between males and females in supernumerary teeth in cleft areas. However, there were no significant statistical differences between male and female subjects in cleft areas and non-cleft areas regarding tooth agenesis, microdontia, ectopic eruption, rotation, and enamel hypoplasia (Table 1).
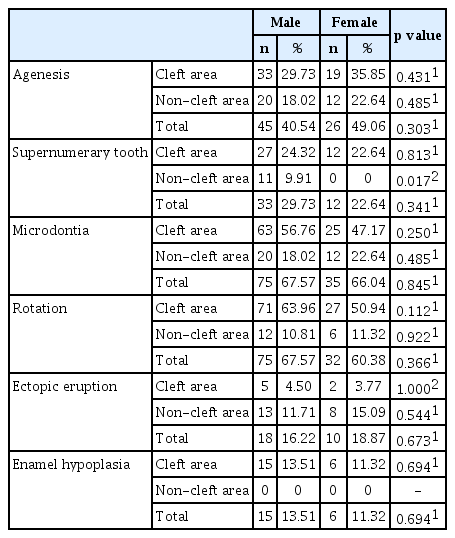
Comparison of dental anomaly prevalence between male and female
Tooth agenesis was notably prevalent in LCLP (65.22%), RCLP (76.47%), and CP (71.43%). LCLP (39.13%) and RCLP (41.18%) exhibited prominent ectopic eruptions, with a significant prevalence of rotation observed in LCLP (82.61%). Furthermore, differences were detected between cleft areas and non-cleft areas for certain dental anomalies. Tooth agenesis in cleft areas was significantly prevalent in LCLP (52.17%) and RCLP (64.71%), whereas CP had a high prevalence of tooth agenesis in non-cleft areas (71.43%). In non-cleft areas, microdontia was significantly observed in CP (57.14%). LCLP (30.43%) and RCLP (35.29%) had a high prevalence of ectopic eruption. For supernumerary teeth and enamel hypoplasia, no significant differences were found in both cleft areas and non-cleft areas (Table 2).
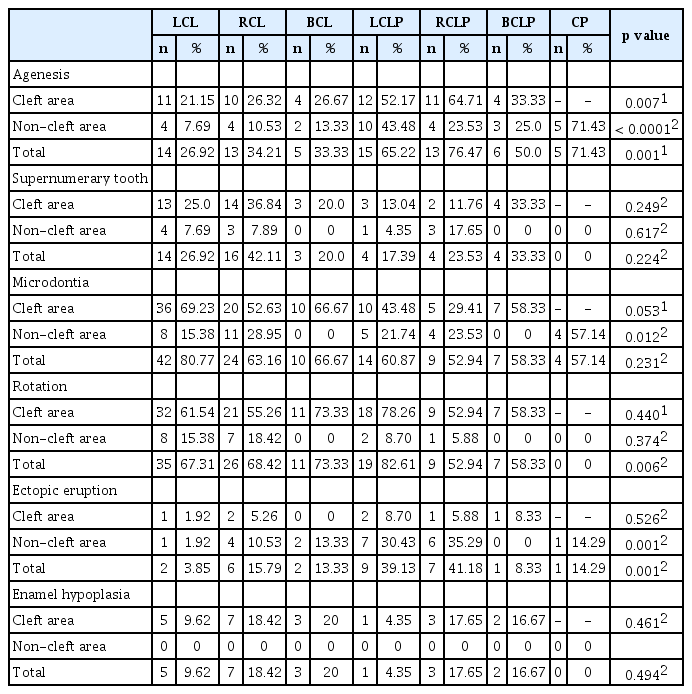
Comparison of dental anomaly prevalence among cleft phenotypes
3. Analysis of tooth agenesis in single tooth and quadrants
In total, 117 missing teeth were identified, with 57 (48.71%) in cleft areas and 60 (51.29%) in non-cleft areas. Maxillary lateral incisors exhibited the highest prevalence of tooth agenesis (29.05%), followed by the maxillary left second premolar (8.54%) and the maxillary right second premolar (6.83%). When considering non-cleft areas exclusively, the maxillary left second premolar was most commonly affected (16.66%), followed by the maxillary right second premolar (13.33%) and the maxillary right first premolar (10.0%).
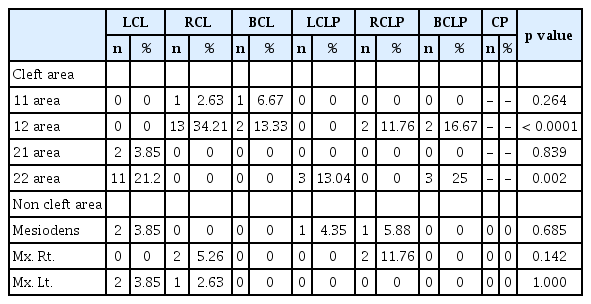
Comparisons of single-tooth agenesis among cleft phenotypes were conducted (Table 3). In cleft areas, the agenesis of the maxillary right lateral incisor was significantly prevalent in RCLP, whereas the maxillary left lateral incisor was significantly common in LCLP (p < 0.0001). In non-cleft areas, LCLP exhibited the highest prevalence of missing teeth (35.0%), followed by RCL and CP (18.33%). Regarding the agenesis of maxillary premolars, the right first and left second premolars were commonly affected in LCLP (13.04% and 17.39%, respectively) and CP (14.29% and 28.57%, respectively). In contrast, the right second premolar was largely affected in CP (28.57%).

Comparison of tooth agenesis among cleft phenotypes
The correlation between quadrants and cleft phenotypes for tooth agenesis was also investigated (Table 4). Tooth agenesis in the upper right quadrant was significantly prevalent in RCLP (76.47%), whereas tooth agenesis in the upper left quadrant was significantly prevalent in LCLP (65.22%). In terms of mandibular quadrants, tooth agenesis in the lower right quadrant was significantly prevalent in CP (28.57%).
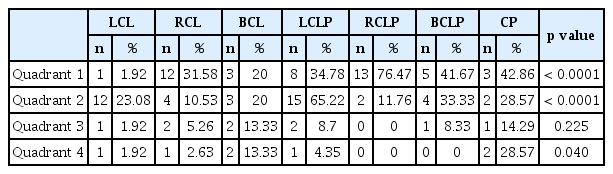
Quadrants analysis of tooth agenesis among cleft phenotypes
4. Analysis of the supernumerary tooth, microdontia and rotation
The most prevalent supernumerary teeth were observed in the maxillary lateral incisor regions (Table 5). Supernumerary teeth near the right lateral incisor were significantly more common in RCL (34.21%, p < 0.0001), whereas supernumerary teeth near the left lateral incisor were significantly (p = 0.002) prevalent in BCLP (25.0%) and LCL (21.15%). There was no significant difference among cleft phenotypes in non-cleft areas.
Comparison of supernumerary teeth among cleft phenotypes
Microdontia was primarily observed in maxillary lateral incisors near the cleft area (Table 6). BCL (66.67%) and RCL (52.63%) exhibited significant microdontia of the right lateral incisor (p < 0.0001). Conversely, microdontia of the left lateral incisor was significantly prevalent in LCL (69.23%, p = 0.002).

Comparison of microdontia among cleft phenotypes
Rotation was similarly common in maxillary incisors near the cleft area (Table 7). The rotation of the right central incisor was found to be significant in RCLP (52.94%) and RCL (52.63%). However, rotation of the left central incisor was significantly prevalent in LCLP (78.26%) and LCL (57.69%, p < 0.0001).

Comparison of maxillary incisor rotation among cleft phenotypes
5. Correlation analysis of dental anomalies
Dental anomalies were concurrently observed in cleft areas (Table 8). However, tooth agenesis and supernumerary teeth did not occur together in these areas. The concurrence between tooth agenesis and rotation was significantly prevalent in LCLP (39.13%) and RCLP (35.29%, p = 0.034). However, other concurrence patterns did not show significant differences in cleft phenotypes.

Correlation of dental anomalies in the cleft area among cleft phenotypes
Discussion
In this retrospective registry-based study, the relationships among dental anomalies, gender, and cleft phenotypes were explored in patients with non-syndromic CL/P. Furthermore, the characteristics of specific dental anomalies affecting individual teeth were evaluated based on cleft phenotypes. Except for variations in supernumerary teeth, no significant gender-based differences in dental anomalies were observed. However, significant differences in dental anomalies based on cleft phenotypes were confirmed, particularly regarding tooth agenesis, microdontia, and ectopic eruption in non-cleft areas.
Patients with syndromic CL/P were excluded from this study. Since other genetic variants associated with syndromes may have influences on dental anomalies, they can interfere with the detection of direct associations between dental anomalies and orofacial clefts [25]. The excluded subjects included those with Goldenhar syndrome, ectodermal dysplasia, CHARGE syndrome, Down syndrome, and Treacher Collins syndrome. Typically, around 70% of patients with orofacial clefts present as non-syndromic cases with isolated clefts, whereas the remaining 30% exhibit syndromic features with multiple congenital defects [26]. The limited 5 number of syndromic cases in the present study could be attributed to several factors, including that patients registered only with a syndromic diagnosis were filtered during the data collection process or patients with severe syndromic complications being unable to receive dental management, thereby contributing to a lack of research data.
In terms of subject distribution, male subjects were approximately twice as likely to be affected by orofacial clefts compared with female subjects. This male-dominant trend was consistent across different cleft phenotypes, except for CP. This observation aligns with existing literatures [27,28]. In the present study, CL was the most common cleft type (64.02%), followed by CLP (31.70%) and CP (4.28%). However, another study conducted with Korean subjects revealed that CLP (63.6%) was the most common, followed by CL (26.8%) and CP (9.6%) [29]. Comparing unilateral and bilateral clefts, unilateral clefts significantly outnumbered bilateral clefts at a ratio of approximately 4:1, which was consistent with previous research findings [29]. Furthermore, left-sided cleft involvement was more frequent than right-sided involvement, both in unilateral CL (57.78%) and CLP (57.50%), with a similar pattern observed in prior studies [27-29]. The underlying reason for this left-sided predominance may be related to the slower facial artery development on the left side compared to the right side, although this hypothesis remains unconfirmed [30].
Rotation of maxillary incisors emerged as the most prevalent dental anomaly in cleft cases, followed by microdontia and tooth agenesis. Although the rotation of maxillary incisors remained the most common anomaly, it showed minimal variation in frequency compared with microdontia and tooth agenesis in a study involving Colombian subjects [22]. In contrast, another study conducted with a Brazilian population reported a higher occurrence of tooth agenesis compared with rotation, with almost twice the frequency [31]. Such disparities among studies can be attributed to variations in subject populations and differences in the criteria defining dental anomalies. The high frequency of maxillary incisor rotation observed in the present study may have been influenced by the skeletal characteristics often found in patients with orofacial clefts. These patients commonly exhibit a range of dental and skeletal malocclusions, predominately associated with Class III malocclusion and maxillary hypoplasia [29,32]. The discrepancy in eruption space due to maxillary hypoplasia, combined with the effects of the cleft itself, may exert compounding influences on the observed prevalence of maxillary incisor rotation.
Gender differences in supernumerary tooth prevalence in non-cleft areas were observed in the present study, with all supernumerary teeth found exclusively in male subjects. In the general population, previous studies estimated that the prevalence of supernumerary teeth was approximately 2 times higher in males than females, though it was found to be lower than in our results [20,33]. The male dominance of supernumerary tooth have been reported in other studies, though the differences were not statistically significant [34,35]. However, many studies have indicated no gender differences in the prevalence of dental anomalies, a trend consistent with the current findings for other dental anomalies [34,36,37]. This suggests that the mechanisms governing dental development may operate independently of somatic and sexual maturity, although the same factors contributing to the cleft condition may influence dental anomalies [38].
Significant differences in the frequency of tooth agenesis, microdontia, rotation, and ectopic eruption were observed across different cleft phenotypes. Additionally, differences in the prevalence of dental anomalies between cleft and non-cleft areas were highlighted. Notably, agenesis was prominent in unilateral CLP in cleft areas and in CP in non-cleft areas. Furthermore, ectopic eruptions within non-cleft areas were prevalent in unilateral CLP. These findings suggest that dental anomalies occurring in non-cleft areas may be related to the presence of the cleft and could potentially establish additional cleft subphenotypes [17,18].
In the present study, the frequency of tooth agenesis was 42.7%, whereas Rakhashan [39] reported a much lower prevalence of 0.15% - 16.2% in the general population. Furthermore, our findings showed a relatively lower prevalence of tooth agenesis in cleft cases compared with that in other studies, which reported rates of 62.0% and 66.8% [31,34]. Tooth agenesis in non-cleft populations often affects the mandibular second premolars, mandibular lateral incisors, maxillary second premolars, and maxillary lateral incisors in sequence [40]. However, our study revealed that the most frequently missing teeth were the maxillary lateral incisors, followed by the maxillary second premolars and the maxillary right first premolars, which was consistent with previous studies [37,41]. Agenesis of the lateral incisors may be attributed to the failure of coalescence between maxillary and medial nasal prominences, potentially leading to a deficiency of mesenchymal mass and contributing to orofacial clefts. The odontogenesis of the lateral incisors is closely related to these regions [36].
In terms of single-tooth associations between tooth agenesis and cleft phenotype, LCLP exhibited the highest prevalence of tooth agenesis, followed by CP, RCLP, and BCLP. This is in contrast to other studies, where BCLP was associated with the highest prevalence of tooth agenesis [31,37,42]. In cleft areas, agenesis of maxillary lateral incisors was significantly more prevalent in ipsilateral CLP compared with CL. In non-cleft areas, 33.9% of missing teeth were found in LCLP, followed by CP (18.6%), with the most common missing teeth being the maxillary second premolars. The severity of clefts may be positively correlated with the prevalence of tooth agenesis, with this relationship likely linked to the extent of the alveolar cleft.
Quadrants analysis among cleft phenotypes revealed that tooth agenesis in quadrant 1 was correlated with RCLP, whereas quadrant 2 was associated with LCLP. Quadrant 4 was related to CP in the mandible, which is consistent with previous studies [37,42]. These results suggest that tooth agenesis in cleft cases may be regulated by genetic control mechanisms and anatomical irregularities near the cleft area [37].
In the present study, most supernumerary teeth (80.0%) were primarily located in the maxillary incisors within the cleft area on the mesial or distal regions near the alveolar cleft. Unlike tooth agenesis, which was predominantly observed in CLP and CP, unilateral CL exhibited a significant prevalence of supernumerary teeth, while both unilateral and bilateral CL had prevalent microdontia of the maxillary incisors, aligning with findings from another study [41,42]. The development of supernumerary teeth in the cleft area may be attributed to the misfusion of separated epithelium, whereas partial epithelial tissue deficiencies may lead to microdontia. In cases of severe epithelium deficiency, tooth agenesis may occur. This variation in dental anomalies between patients with CL and CLP could be explained by the degree of alveolar defects related to epithelial tissue deficiency, which is typically less pronounced in CL cases [41].
In the current study, rotation was largely examined in the maxillary central incisors, in contrast to the lateral incisors. Right central incisor rotation was notably prevalent in RCLP and RCL, whereas left central incisor rotation was prominent in LCLP. These results contrast with findings in other studies, where rotation of the maxillary incisors was significantly prevalent in BCLP [43,44]. Considering the concurrence between tooth agenesis and the maxillary incisor rotation in unilateral CLP, the pattern of maxillary incisor rotation in our study may be related to tooth agenesis in specific cleft phenotypes.
A limitation of our study was that only orofacial cleft patients were selected as study subjects. To identify den-tal anomalies that occur prominently in orofacial cleft patients, it is necessary to conduct a study comparing cleft patients and non-cleft patients as controls. Additionally, alveolar cleft involvement was not considered when investigating patients with CL. Given the close relationship between alveolar clefts and dental anomalies near cleft areas, it is essential to account for the presence or absence of alveolar clefts. Furthermore, potential iatrogenic effects on developing teeth during alveolar bone grafting procedures should be considered. Despite these limitations, our study’s major contribution lies in the differentiation of cleft areas and non-cleft areas, which facilitates a more comprehensive understanding of dental anomalies. Moreover, this study offers a comprehensive classification of cleft phenotypes compared with prior studies with limited phenotype categorization.
The results of this present study emphasize the importance of phenotyping based on dental anomalies in patients with clefts. Given the substantial challenges that dental anomalies present to clinicians, conducting a thorough examination of these anomalies may be beneficial in establishing long-term and elaborate treatment strategies, potentially leading to improved quality of life for cleft patients and their caregivers.
Conclusion
Our findings suggest that the prevalence of supernumerary teeth in non-cleft areas was significantly higher in males, whereas other dental anomalies showed no statistical gender-based differences. In non-cleft areas, significant differences were observed in tooth agenesis and microdontia, which were most commonly found in patients with CP, whereas ectopic eruption was prevalent in unilateral CLP. Additionally, the rotation of maxillary incisors was closely associated with adjacent tooth agenesis in unilateral CLP. Overall, the present results raise the possibility of subphenotyping or categorizing patients with orofacial clefts based on dental anomalies.
Notes
Conflict of Interest
The authors have no potential conflicts of interest to disclose.