Effects of Facemask Therapy for Class III Malocclusions in Patients with Different Vertical Skeletal Patterns
3급 부정교합 환자의 수직적 골격 양상에 따른 facemask 치료 효과 비교
Article information
Abstract
The purpose of this study was to evaluate the skeletal and dentoalveolar effects of facemask therapy and to compare the anchorage of a bonded expander in patients with Class III malocclusion and different vertical skeletal patterns.
Twenty subjects with Class III malocclusion were included in this study and were treated with a facemask and bonded expander. Based on the FMA, subjects were divided into two groups of 10 patients each: a high vertical group (HV; mean FMA 33.56º) and an average vertical group (AV; mean FMA 24.88º). Lateral cephalograms were taken and evaluated before and after treatment.
In both groups, forward movement of the maxilla and backward rotation of the mandible were observed after treatment, with no statistical differences between the groups. Vertical skeletal variables increased in both groups, but the increase of FMA was significantly larger in the HV group than the AV group. Mesial movement of maxillary molars and proclination of maxillary incisors which indicate anchorage loss of bonded expander were observed in both groups, with no significant differences between the groups.
In conclusion, facemask therapy resulted in effective maxillary protraction in both HV and AV groups. However, the open bite tendency was increased more in the HV group.
Trans Abstract
본 연구의 목적은 3급 부정교합 환자에서 facemask 치료 시 수직적 골격 양상에 따른 치료 효과를 비교하고, 구내 장치로서 bonded expander의 고정원을 평가하는 것이다.
Facemask 치료를 받은 20명의 환자를 대상으로 FMA를 기준으로 두 군으로 분류하였고(HV군; FMA > 27º, AV군; 23º< FMA < 27º), 치료 전과 후 측모두부방사선사진을 촬영하여 계측치를 비교하였다.
치료 후 두 군 모두 상악의 전방이동 및 하악의 후하방 회전이 관찰되었고, 두 군간에 유의한 차이는 없었다. 두 군 모두 수직적 골격 계측치가 증가하였고, FMA의 증가량은 HV군이 AV군에 비해 유의하게 크게 관찰되었다. 고정원 소실로서 상악 구치의 근심이동 및 상악 전치의 전방경사가 관찰되었고, 두 군간에 유의한 차이는 없었다.
결론적으로 수직적 골격 양상에 따라 상악의 전방이동 및 고정원 소실면에서는 유의한 차이가 없었으나, HV군에서 수직적 성장 경향이 더 증가하였다.
Ⅰ. Introduction
Orthopedic treatments are recommended for growing patients with Class III malocclusion. Orthopedic appliances such as facemask, functional appliance, and chincap have been used for the treatment of Class III malocclusion [1-3]. It has been reported that more than 60% of Class III malocclusions are due to maxillary deficiency [4,5], and maxillary protraction with a facemask is an effective treatment approach for Class III malocclusions with maxillary deficiency.
Many studies have reported the effects of facemask therapy [6-10], but few studies have been performed to compare the effects of the facemask in patients with different vertical patterns. In a study by Yoshida et al. [11], the orthopedic effects of combined maxillary protraction and a chincap appliance were compared between two groups (long versus short facial groups). The authors demonstrated that the short facial group showed significantly greater anterior movement of the maxilla than the long facial group, but there was no significant difference in vertical skeletal changes between the two groups. Koh et al. [12] compared treatment outcomes between groups treated with a tooth-borne facemask or a skeletal anchored facemask according to the vertical skeletal pattern (high versus low angle types). They reported that the tooth-borne facemask group showed greater opening tendency of the mandibular plane angle than the skeletal anchored facemask group when applied to the high angle type, but there was no significant difference in the vertical change between the groups when applied to the low angle type. However, they did not compare the results between high and low angle types within the tooth-borne facemask group.
It is known that facial types with an open bite tendency show weak bite force compared with those with a deep bite tendency [13]. Since the bite force could influence the degree of orthodontic anchorage [14], there might be differences in the anchorage of intraoral appliances used for the tooth-borne facemask according to the vertical skeletal patterns, which could in turn influence the skeletal and dentoalveolar effects of facemask therapy.
The purpose of this study is to evaluate the skeletal and dentoalveolar changes after orthopedic treatment with a facemask and to compare the anchorage of a bonded expander in patients with Class III malocclusion and different vertical skeletal patterns.
Ⅱ. Materials and Methods
1. Subjects and treatment procedures
This study was approved by the Institutional Review Board of Samsung Medical Center (IRB File No.: 2013-06-007-001). Subjects were collected from Samsung Medical Center from January 2008 to February 2013. Among 81 patients (42 boys, 39 girls) who were treated with a facemask during early mixed dentition, 20 subjects (11 boys, 9 girls) were selected for this study based on the following inclusion criteria:
1) Anterior crossbite including upper four incisors
2) Class III malocclusion with maxillary deficiency
3) Prepubertal growth stage
4) Use of bonded expander for an intraoral anchorage of the facemask
5) Four teeth covered by bonded expander on each side
6) No previous history of orthodontic treatment
7) Healthy patients without any medical history or syndromes
Based on the FMA, the subjects were divided into two groups, the high vertical group (HV; FMA > 27º) and average vertical group (AV; 23º< FMA < 27º). Each group consisted of 10 subjects: HV group (4 boys, 6 girls; mean age 8 years) and AV group (7 boys, 3 girls; mean age 8 years 3 months).
The bonded expander covered four teeth (primary canine, first and second primary molars, and first permanent molar) on each side (Fig. 1), and two hooks for maxillary protraction were added on the primary canine area. Maxillary expansion was performed for 1 - 4 weeks at a rate of a quarter turn a day until the required maxillary expansion was achieved according to the individual transverse discrepancy. After maxillary expansion, maxillary protraction was initiated with a Petit-type facemask (Ormco Co., USA). Elastics delivered a force of 450 g to each side. The vector of the force was approximately 30º downward from the occlusal plane. The subjects were instructed to wear the facemask for at least 14 hours a day, and the treatment was continued for 1 year.

The bonded expander covered four teeth (primary canine, first and second primary molars, and first permanent molar) on each side.
2. Cephalometric analysis
Lateral cephalometric radiographs were obtained before (T1) and after (T2) the facemask treatment. All radiographs were traced and measured by two investigators using V-ceph 6.0 software (Osstem Implant Co., Korea). The cephalometric landmarks and measurements used in this study are defined in Fig. 2. For evaluation of maxillary teeth movement, two reference planes were constructed. The horizontal reference plane (HRP) is a line passing from the ANS to PNS. The vertical reference plane (VRP) is a vertical line passing through ANS and perpendicular to the HRP (Fig. 3).
The cephalometric landmarks and measurements. Maxillary length and mandibular length indicate Co-A and Co-Gn, respectively.
Maxillary dentoalveolar measurements. 1. Incisal tip of U1a to VRPb (mm); 2. MBCc of U6d to VRP (mm); 3. MBC of U6 to HRPe (mm); a U1 (maxillary incisor); b VRP (vertical reference plane); c MBC (mesiobuccal cusp tip); d U6 (maxillary first molar); e HRP (horizontal reference plane).
3. Statistical analysis
The means and standard deviations of all cephalometric variables were obtained at T1 and T2. The cephalometric changes after the treatment (T2 - T1) were calculated; note that the changes of MBC (mesiobuccal cusp tip) of U6 (maxillary first molar) to VRP were calculated as T1 - T2 to yield a positive number. For evaluation of repeatedly measured cephalometric values by two investigators, statistical analysis using mixed-effects model was performed by SAS version 9.3 (SAS institute, USA). P - values were corrected by Bonferroni’s method and considered as statistical significance at the level of 0.05. The intraclass coefficient (ICC) was obtained to assess the reliability of cephalometric measurements evaluated by two investigators, and the ICC of all measurements showed high agreement between the two investigators.
Ⅲ. Results
1. Cephalometric measurements before the treatment
Initial cephalometric measurements before the treatment are shown in Table 1.
Cephalometric measurements before the treatment (T1) in the high vertical skeletal group (HV) and the average vertical skeletal group (AV)
1) Sagittal skeletal parameters
ANB was significantly larger in the HV group than AV group. SNB and Pog to N-perpendicular were significantly greater in the AV group than HV group. However, there were no statistical differences in maxillary and mandibular lengths, which represent the size of the maxilla and mandible respectively.
2) Vertical skeletal parameters
FMA and SN to mandibular plane angle (SN-MP) were significantly larger in the HV group than AV group.
3) Dental parameters
No significant differences in the inclination of maxillary incisors (U1 to SN and U1 to NA angular measurement) were found between the two groups. In contrast, the inclination of mandibular incisors was significantly more upright in the HV group than AV group.
2. Cephalometric changes after the treatment
Cephalometric measurements after the treatment (T2) and cephalometric changes (T2 - T1) are shown in Table 2 and Table 3.
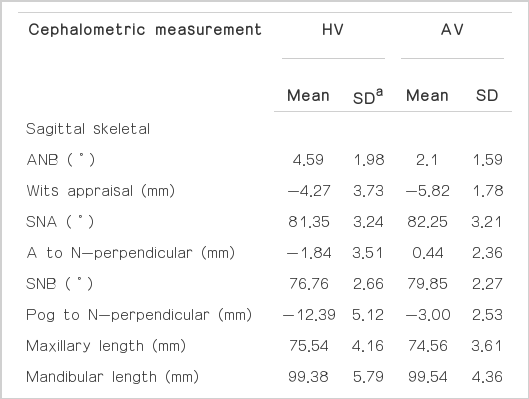
Cephalometric measurements after the treatment (T2) in the high vertical skeletal group (HV) and the average vertical skeletal group (AV)

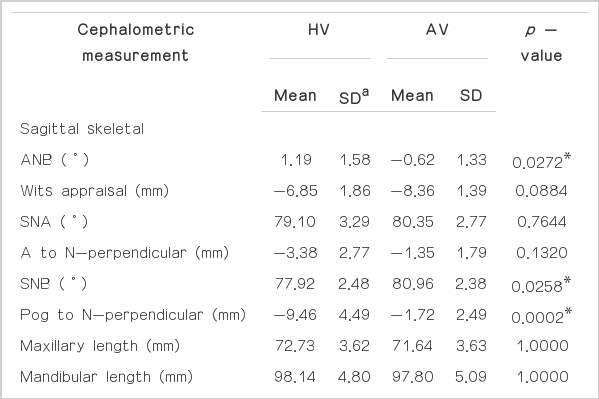
Cephalometric changes after the treatment (T2 - T1) in the high vertical skeletal group (HV) and the average vertical skeletal group (AV). Note that the changes of MBC of U6 to VRP were calculated as T1-T2 to yield a positive number
1) Sagittal skeletal parameters
ANB and Wits appraisal increased in both groups, with no significant differences between the two groups. An increase in SNA and A to N-perpendicular and a decrease in SNB and Pog to N-perpendicular were observed in both groups, and no significant differences were found between the groups.
2) Vertical skeletal parameters
Mandibular plane angles increased in both groups. The increase in FMA was significantly larger in the HV group than AV group. SN-MP also tended to increase to a greater extent in the HV group than AV group, although the difference was not statistically significant.
3) Dental parameters
Variables related to the maxillary incisors and molars (U1 to SN, incisal tip of U1 to VRP, and MBC of U6 to VRP) increased in both groups, with no significant differences between groups. However, the changes in mandibular incisors were significantly different between the two groups: both IMPA and L1 to NB (angular) decreased in the AV group after treatment, but no significant changes were observed in the HV group.
Ⅳ. Discussion
Many clinical studies have described a combination of skeletal and dentoalveolar effects of facemask therapy. Forward movement of the maxilla and backward rotation of the mandible contribute to improving the skeletal discrepancy of Class III malocclusion. In addition to skeletal effects, dentoalveolar effects including proclination of maxillary incisors and retroclination of mandibular incisors also contribute to correcting the anterior crossbite [6-10]. In general, vertical skeletal patterns are divided into high and low angle growth patterns [13]. Some previous studies have reported that patients with Class III malocclusion and high vertical skeletal pattern showed poor stability for orthopedic treatment outcomes [15,16], but little information is known about the effects of facemask therapy with different vertical skeletal patterns.
In general, two types of intraoral appliances, bonded expander and hyrax, are used as intraoral appliances in facemask therapy. Only subjects treated with a bonded expander splinting four teeth on each side were included in this study because the design of the intraoral appliance and the number of teeth splinted could influence the degree of intraoral anchorage for facemask therapy.
In some cases with crowded maxillary incisors and palatally positioned lateral incisors, fixed orthodontic appliances can be used to align the maxillary incisors during the facemask therapy. However, in this study, patients who were treated with a fixed orthodontic appliance simultaneously with the facemask to align maxillary incisors were excluded because dentoalveolar changes of maxillary incisors after the treatment might not reflect the actual facemask effects, and the anchorage value of the intraoral appliance could be affected because whole maxillary teeth were splinted as a single unit through the fixed orthodontic appliances.
Regarding cephalometric changes after facemask therapy, ANB and A to N-perpendicular increased in both groups with no significant difference. Yoshida et al. [11] demonstrated a difference in the response to treatment with maxillary protraction and a chincap appliance in Class III malocclusion patients with different vertical skeletal patterns, in which forward movement of the A point was significantly larger in the short face group than in the long face group. The authors explained that the short face group was considered to have a better potential for anterior growth of the mandible and this led to greater anterior movement of maxilla in the short face group through interdigitation with the mandible. In the present study, however, there was no significant difference in anterior movement of maxilla between the two groups. It is possible that use of a bonded expander as an intraoral appliance in this study meant that there was little influence on the interdigitation of occlusion.
The optimal results of maxillary protraction with a tooth-borne facemask are to achieve maximal skeletal effects and minimize undesired dental effects such as mesial movement or angulation of maxillary teeth. Nonetheless, it is inevitable that undesired tooth movement accompanies skeletal effects when elastics transfer the force to the intraoral appliance. The undesired tooth movement indicates anchorage loss. It has been reported that anchorage loss might differ according to vertical facial types, because a long facial type has weaker molar bite force than a short facial type, which could result in greater anchorage loss [13,14]. In this study, however, the changes of the MBC of U6 to VRP, incisal tip of U1 to VRP, and U1 to SN which indicate mesial movement of maxillary teeth and proclination of maxillary incisors showed no statistical difference between the two groups. The bonded expander used in this study splinted four teeth on each side, and is considered the maximum anchorage that can be obtained in early mixed dentition. Facemask treatment with bonded expander splinting three teeth (e.g., first and second primary molars, and first permanent molar) on each side may lead to different results with vertical skeletal patterns.
Vertical skeletal changes showed significantly different results between the two groups. FMA increased in both groups, but the HV group showed a pronounced increase compared with the AV group. SN-MP also tended to increase more in the HV group than AV group, although there was no significant difference. A previous study showed that opening of mandibular plane angles in facemask therapy was caused by counterclockwise rotation of the maxilla and extrusion of maxillary molars [17,18]. Since there was no statistical difference in palatal plane angle (SN-PP) between the two groups, the degree of maxillary rotation was thought to be similar between the groups. However, the increase in FH-OP tended to be larger in the HV group than AV group, even though there was no significant difference between the groups. Therefore it could be assumed that the difference in vertical changes occurred because of different changes in occlusal plane between the groups. The difference in bite force with different vertical skeletal patterns could also explain why the occlusal plane angle increased more in the HV group. For these reasons, applying facemask to Class III malocclusion patients with high vertical skeletal patterns could worsen the open bite tendency of the patients.
Tanne et al. [19] and Hirato [20] revealed that the maxillary complex had a center of resistance between the root apices of the maxillary first and second premolars. In order to place the vector of force closer to the center of resistance of maxilla and to minimize rotation of maxilla, hooks for maxillary protraction should be located in the canine or first primary molar area above the occlusal plane, thus reducing clockwise rotation of the mandible. In addition, the recommended direction of force is 30˚ downward to the occlusal plane to minimize the maxillary rotation [21]. Together with these efforts to prevent vertical opening by modifying the design of the intraoral appliance, skeletal anchorage has been introduced to provide absolute anchorage and transfer the force as close as possible to the center of resistance of maxilla. Koh et al. [12] demonstrated that a skeletal anchored facemask did not aggravate the open bite tendency when it was applied to patients with a high vertical type. However, in spite of this benefit, most of the patients indicated for the facemask are too young to apply skeletal anchorage and additional surgical operations are required to place and remove the miniplates.
In previous studies, retroclination of mandibular incisors was reported as a result of facemask therapy [6,7]. In the present study, the AV group showed a significant decrease in IMPA, whereas the HV group showed no statistical change in IMPA after treatment. Initial IMPA of the AV group was 93.71˚, representing flared mandibular incisors compared with normal. A possible explanation for this result is that patients in the AV group often have greater incisal overbite than those in the HV group and this can easily cause a labially directed force and traumatic occlusion of mandibular incisors. After correction of the anterior crossbite with facemask therapy, the flared mandibular incisors would spontaneously become upright. On the other hand, the HV group rarely has traumatic occlusion of mandibular incisors due to the shallow overbite, therefore the different change in mandibular incisors might reflect different overbite status of the two groups.
To order to ensure similar treatment protocols between the two groups, patients enrolled in this study were selected by specific inclusion criteria, for example the same type of intraoral appliance and number of teeth covered by the bonded expander. However, application of these selection criteria resulted in a relatively small sample size. Despite this limitation, significant findings were obtained regarding different outcomes of facemask therapy in patients with different vertical skeletal patterns. Further investigations including more samples are needed for more reliable results about the effects of facemask therapy with different vertical skeletal patterns.
Ⅴ. Conclusions
Effects of facemask therapy for Class III malocclusions in patients with different vertical skeletal patterns were evaluated in this study. After treatment, a significant increase in ANB resulting from forward movement of maxilla and backward rotation of mandible was observed in both HV and AV groups. The anchorage loss of bonded expander (mesial movement of maxillary molars and proclination of maxillary incisors) was observed in both groups, with no statistical difference between groups. In vertical changes, an increase in mandibular plane angles was observed in both groups, but the HV group showed a significantly larger increase than the AV group.