상악 측절치 과잉치의 특징 분석
Analysis of the Characteristics of Maxillary Supernumerary Lateral Incisor
Article information

Abstract
이 연구의 목적은 상악 측절치 과잉치의 해부학적인 특징과 정상 측절치와의 관계에 대해 정량적 분석을 시행하는 것에 있다. 43명의 44개의 상악 측절치 과잉치를 대상으로 전산화 단층 방사선사진을 이용하여 측절치 과잉치의 위치, 형태, 방향 및 측절치 과잉치와 인접한 영구전치와의 관계를 관찰하였다. 또한 측절치 과잉치와 인접한 측절치 및 반대측 측절치의 크기를 비교하기 위해 각각의 치관 근원심 폭경을 계측하였고, 치아성숙도를 비교하기 위해 Nolla stage를 이용하여 각 치아의 치근 발육 정도를 평가하였다. 측절치 과잉치는 90.9%의 비율로 정위 방향으로 존재하였고, 84.1%가 보충형의 형태로 존재하였다. 측절치 과잉치는 인접한 측절치나 반대측의 측절치에 비해 치관의 크기가 통계적으로 유의하게 작았고(p< .0001), 치근 발육 단계에서는 통계적 유의미한 차이를 보이지 않았다. 결론적으로, 상악 측절치 과잉치는 정상측절치와 매우 유사하지만 치관 크기에 있어서 차이를 보인다. 상악 측절치 과잉치가 존재하는 경우, 교정적 혹은 심미적인 문제를 줄이기 위해 측절치와 과잉치를 정확하게 구분하여 치료하는 것이 중요하다.
Trans Abstract
This study aimed to investigate a quantitative analysis of the anatomical characteristics of the maxillary supernumerary lateral incisor and its relationship with lateral incisors. Forty-four supernumerary lateral incisors from 43 patients were evaluated for analyzing the position, shape, direction, and relationship between the supernumerary lateral incisor and the normal lateral incisors, using cone-beam computed tomography (CBCT). To compare the size of crown, the mesiodistal width was measured and the Nolla stage was used for evaluating the degree of root development to compare tooth maturity. The supernumerary lateral incisors were in the normal direction at a rate of 90.9%, and in a supplemental shape at a rate of 84.1%. The supernumerary lateral incisor was smaller in size compared to the adjacent lateral incisor and opposite lateral incisor (p < .0001). There was no statistically significant difference in the development stage of root. Based on these results, the supernumerary lateral incisor is similar with the lateral incisor, but has a difference in the size of crown. It is necessary to distinguish the supernumerary lateral incisor from the lateral incisor precisely to reduce clinical complications.
Ⅰ. 서 론
과잉치는 가장 흔하게 나타나는 치아의 발육장애 중 하나로, 정상적인 치아의 개수이외의 치아가 존재하는 것을 의미한다. 과잉치는 한 개 또는 여러 개가 나타날 수 있고, 정중구개부에서 가장 흔하게 나타난다[1]. Hyun 등[2]에 의하면 91.5%의 비율로 상악 전치부 구개측에서 관찰된다. 과잉치의 형태는 원뿔형(conical), 결절형(tuberculate), 보충형(supplemental)으로 분류할 수 있다[3,4]. 원뿔형은 왜소치와 유사하게 크기가 작은 원뿔형태로 나타나는 경우를 말하며, 결절형은 1개 이상의 교두나 결절이 존재하는 형태, 보충형은 정상적인 발육과정을 통해 정상 치아의 형태를 갖는 경우를 말한다.
측절치 과잉치는 지금까지 잘 알려져 있지는 않았지만 정중 과잉치와는 다른 특성을 가진 과잉치로 구분된다. Jung 등[5]은 상악 측절치에 발생한 보충형의 과잉치 증례를 통해 보충형 과잉치는 상악 측절치에서 호발한다고 보고하였으며, 이를 ‘double lateral incisors’라고 지칭하였다. Wedrychowska-Szulc 와 Janiszewska-Olszowska는[6] 측절치 과잉치는 인접한 측절치보다 작으며, 두 치아 모두 정상 측절치보다 크기가 작다고 언급하였다. Yildirim와 Bayrak는[7] 양측성 상악 측절치 과잉치 증례 보고에서 측절치 과잉치에서 구개면의 깊은 발육구나 치내치 경향을 보인다고 보고하였다. Arandi[8]는1974년부터 2020년까지 보고된 측절치 과잉치의 유병률은 0.05 - 1.59%이며, 하악보다 상악에서 호발하고, 편측성 및 보충형 형태로 나타난다고 보고하였다.
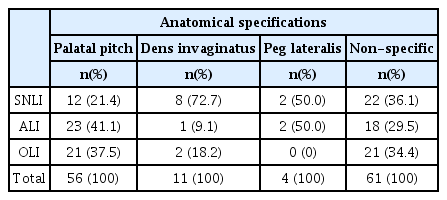
즉, 기존의 논문에 따르면 측절치 과잉치는 정중과잉치와 위치, 형태, 크기, 발육상태에 있어 차이를 보인다(Table 1). 첫번째로 정중과잉치는 주로 정중구개부에서 관찰되는 반면, 측절치 과잉치는 측절치의 근원심측에서 관찰된다[3]. 두번째로 정중과잉치에서는 원뿔형이 가장 많이 관찰되는 것과는 달리, 측절치 과잉치에서는 대부분 정상 측절치와 유사한 형태를 갖는 보충형의 과잉치가 관찰된다[2,8]. 세번째로 정중과잉치는 대부분 인접한 중절치보다 작은 크기이다[3]. 반면, 측절치 과잉치는 인접한 측절치와 거의 같은 형태로 나타나는데, 측절치 과잉치와 인접한 측절치 둘다 반대측의 정상 측절치보다 크기가 작은 경향이 있다[6,8]. 네번째로 정중과잉치는 유치보다는 치근발육이 느리나 영구치보다는 빠른, 유치와 영구전치의 중간정도의 치근 발육정도를 보인다. 그에 비해, 측절치 과잉치는 영구 측절치와 유사한 치근 발육정도를 보인다. 마지막으로 측절치 과잉치에서는 전반적인 크기와 형태는 정상 측절치와 유사하나, 깊은 구개측의 발육구 혹은 치내치와 같은 특징적인 치아 이상이 관찰된다[8].

Comparison of anatomical and clinical characteristics of mesiodens and maxillary supernumerary lateral incisor
지금까지 정중과잉치에 대해서는 활발한 연구와 문헌고찰이 이루어져 왔다. 반면, 상악 측절치 과잉치는 정중과잉치와 마찬가지로 임상적인 문제를 야기함에도 불구하고 이에 대해 증례보고 및 정성적인 연구가 있었고, 정량적인 연구는 없었다. 이 연구의 목적은 상악 측절치 과잉치의 해부학적인 특징과 정상 측절치와의 관계에 대해 정량적 분석을 시행하는 것이다.
Ⅱ. 연구 대상 및 방법
1. 연구 대상
이 연구는 경희대학교 치과병원의 임상 연구 윤리 위원회(Institutional Review Board)의 승인 하에 진행하였다(KHDT21007). 2015년 1월 1일부터 2020년 12월 31일까지 경희대학교 치과병원 소아치과에서 전산화 단층 방사선사진(cone beam computerized tomography, CBCT)을 촬영한 환자를 대상으로 상악 측절치 과잉치를 갖는 환자를 대상자로 선정하였다. CBCT 촬영을 위해 Alphard Vega Dental CT system (Asahi Roentgen Ind. Co., Kyoto, Japan)을 이용하였다. Zetta pacs(Tae young soft, Anyang, Korea)프로그램을 이용하여 전산화 단층방사선사진을 계측 및 평가하였다.
2. 연구 방법
1) 대상 선정기준 및 제외기준
이 연구에서는 Table 1에 열거된 상악 측절치 과잉치의 특징 6가지 중에서 마지막 항목인 드물게 나타나는 구개측의 발육구와 치내치를 제외한 5가지의 일반적인 특징 중 3가지 이상을 만족하는 경우를 상악 측절치 과잉치로 정의하였다. 측절치 과잉치의 판별이 어려운 경우에는 경력 11년의 소아치과 전문의 및 2년차 소아치과 전공의가 토의하여 판정하였다. 전신적인 질환에 의해 다수의 과잉치를 갖는 경우는 조사대상에서 제외하였다. 상악 전치부에 영구치의 결손이 있는 경우 및 과잉치가 상악 구치부, 즉 상악 견치보다 원심측에 존재하는 경우도 제외되었다. 이와 같은 선정기준에 따라 선정된 측절치 과잉치 증례들의 의무기록과 CBCT를 분석함으로써 상악 측절치 과잉치의 임상적인 특징을 평가하였다. 이 연구에서는 계측과정에서의 신뢰도 평가를 위하여 20개의 표본을 무작위로 골라 재현성을 평가하였다. 두 명의 소아치과 의사가 같은 CBCT이미지를 2주 간격으로 판독하였고, 조사자간 신뢰도 및 조사자내 신뢰도 값은 모두 0.90 이상으로 나타났다.
2) 측절치 과잉치와 정상 측절치의 구분
측절치 과잉치는 정상 측절치와 비슷한 시기에 발육하며, 형태와 크기가 매우 비슷하여 구분하기 매우 어렵다. 이 연구에서는 측절치 과잉치와 인접한 정상 측절치를 구분하기 위해 절단연 양 끝의 2개의 점각(point angle) 및 근원심 구개변연융선의 존재여부, 반대측 정상 측절치와의 치관 근원심 폭경의 차이를 기준으로 평가하였다(Fig. 1). 정상 측절치에서는 영구전치의 형태학적 특징인 근심 및 원심 구개변연융선이 뚜렷하게 관찰되며 절단연 양끝의 근심-설측 점각과 원심-설측 점각이 존재한다. 반면, 과잉치는 전반적인 형태는 측절치와 닮아 있으나 근원심 구개변연융선이 도드라지게 존재하지 않으며, 절단연의 점각이 도드라지지 않거나 존재하지 않는다.

CBCT images of the maxillary supernumerary lateral incisor on #22 area. (A) 3-Dimensional image of maxillary lateral incisor. (B) normal lateral incisor on opposite side(#12). (C) adjacent lateral incisor(#22). (D) absence of marginal ridge and point angle in supernumerary lateral incisor(red line and arrow: mesio- and disto-palatal marginal ridge, yellow spot: mesioand disto-palatal point angle, white arrow: the supernumerary lateral incisor).
3) 위치 분류기준
상악 측절치와 측절치 과잉치의 위치 관계를 분석하기 위해 다음과 같은 기준을 임의로 설정하여 이에 따라 과잉치의 위치를 분류하였다. 먼저 과잉치의 근원심적인 위치 분류를 위해 상악 중절치, 측절치 및 견치의 중심선을 기준으로 설정하였다. 상악 견치 중심선부터 상악 측절치 중심선까지의 부위를 Ⅰ, 상악 측절치 중심선부터 상악 중절치 중심선까지의 부위를 Ⅱ, 좌측 상악 중절치 중심선과 우측 상악 중절치 중심선 사이의 부위를 Ⅲ으로 구분하였다. 또한 과잉치의 전후방적인 위치 평가를 위해 인접한 양측의 두 치아보다 순측에 존재하는 경우를 L, 구개측에 존재하는 경우를 P로 구분하였다. 이와 같은 두가지 분류 기준에 따라 6개의 항목(ⅠL, ⅠP, ⅡL, ⅡP, ⅢL, ⅢP)으로 과잉치의 위치를 평가하였다(Fig. 2).
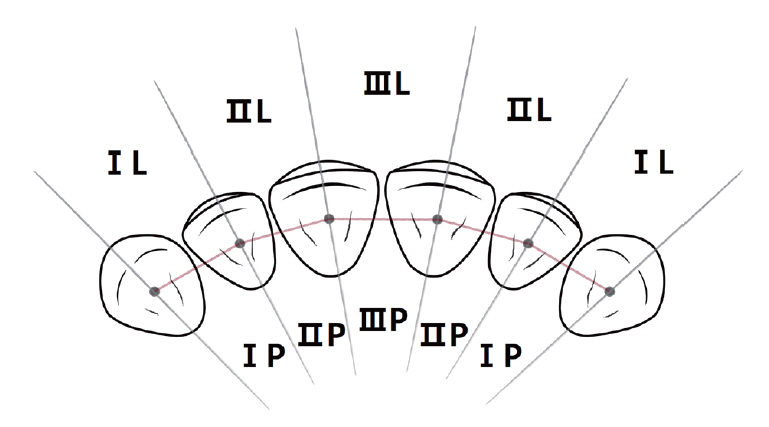
Position of supernumerary lateral incisor according to the transverse view of the anterior maxilla: region ⅠL-located at disto-labial area of the adjacent lateral incisor; region ⅠP-located at disto-palatal area of the adjacent lateral incisor; region ⅡL-located at the labial area between lateral incisor and central incisor; region ⅡP-located at the palatal area between lateral incisor and central incisor; region ⅢL-located at the labial area between both central incisors; region ⅢP-located at the palatal area between both central incisors.
4) 측절치 과잉치의 형태 및 발육학적 특징
(1) 측절치 과잉치의 형태 및 방향 분류
형태 분류는 원뿔형, 결절형, 보충형의 3가지로 분류하였다. 측절치 과잉치의 형태는 Zetta pacs프로그램을 이용하여 파노라마 방사선사진 및 CBCT를 평가하여 분류하였다. 과잉치의 방향은 정위(normal direction), 역위(inversion), 회전(rotation)의 3가지로 분류하였다.
(2) 치관의 크기
상악 측절치 과잉치의 크기를 측정하여 과잉치가 존재하는 해당악의 측절치 및 반대측 정상 측절치와의 크기 비교를 위해 Zetta pacs프로그램을 이용하여 CBCT상에서의 상악 측절치 과잉치 및 측절치의 근원심 폭경을 계측하였다. CBCT의 수직절단면 상에서 관찰되는 상악 측절치 과잉치 및 인접한 측절치, 반대측 측절치의 근원심 폭경의 최대값을 계측하여 각 치아의 크기를 비교하였다.
(3) 치근 발육 단계
측절치 과잉치와 인접한 측절치 및 정상 측절치의 치아 성숙도를 비교하기 위해 Nolla stage를 이용하여 각 치아의 치근 발육 단계를 평가하였다. Nolla stage의 각 단계는, 0단계는 치와의 부재, 1단계는 치와의 형성, 2단계는 초기 석회화의 개시, 3단계는 치관의 1/3 형성, 4단계는 치관의 2/3 형성, 5단계는 치관의 대부분이 형성, 6단계는 치관 형성 완료, 7단계는 치근의 1/3 형성, 8단계는 치근의 2/3 형성, 9단계는 근단공이 개방된 상태로 치근 대부분이 형성, 10단계는 근단공의 폐쇄를 의미한다[9]. 이 연구에서는 조사대상의 치근 발육 단계를 평가하는 과정에서 치아의 만곡이나 회전, 영상의 중첩으로 인해 Nolla stage의 정확한 관찰이 어려운 경우, Shin 등이[10] 제시한 성별에 따른 영구치의 평균발달 연령과 대상자의 연령을 참고하여 판정하였다.
(4) 형태학적 특징
CBCT상에서의 측절치 과잉치와 양측의 측절치의 구개측의 발육구, 치내치 및 왜소치 여부를 관찰하였다.
5) 통계분석방법
상악 측절치 과잉치의 위치, 형태, 크기, 치근 발육 단계와 같은 특징 간의 연관성을 살펴보기 위해 ANOVA와 Kruskal-Wallis test를 사용하여 분석하였다. 이 연구의 통계분석 프로그램은 SAS statistics프로그램(version 9.4, SAS Institute, USA)을 이용하였다.
Ⅲ. 연구 결과
1. 인구학적 특성
전체 985명 중 선별조건을 만족하는 43명의 어린이가 최종 대상자로 선정되었고, 그 비율은 4.37%였다(Table 2). 남자는 29명, 여자는 14명으로 남자가 여자보다 약 2배 많았다. 측절치 과잉치가 발견된 시점의 연령은 평균 7.83세로 6세부터 9세까지가 약 79%의 비율로 가장 많았다. 대상이 되는 상악 측절치 과잉치는 총 44개였다.
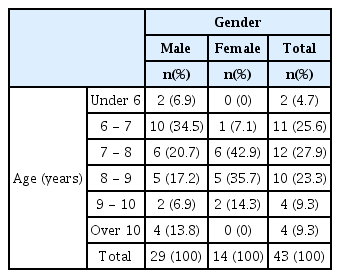
Incidence of the maxillary supernumerary lateral incisors by gender and age
2. 측절치 과잉치의 위치
측절치 과잉치는 인접한 측절치의 원심순측인 ⅠL에서 약 36%의 비율로 가장 많이 나타났고, 중절치와 측절치 사이의 구개부인 ⅡP에서 약 31%의 비율로 두번째로 많이 나타났다. 이처럼 측절치와 측절치의 과잉치 중에서 근심측의 치아는 구개측, 원심측의 치아는 순측에 위치하는 형태로 존재하는 경우가 가장 많았다(Fig. 3A). 측절치 과잉치가 존재하는 경우 측절치와 측절치 과잉치가 상악 전치부의 이상적인 치열을 갖지 않는 경우가 대부분이었다(Fig. 3B).
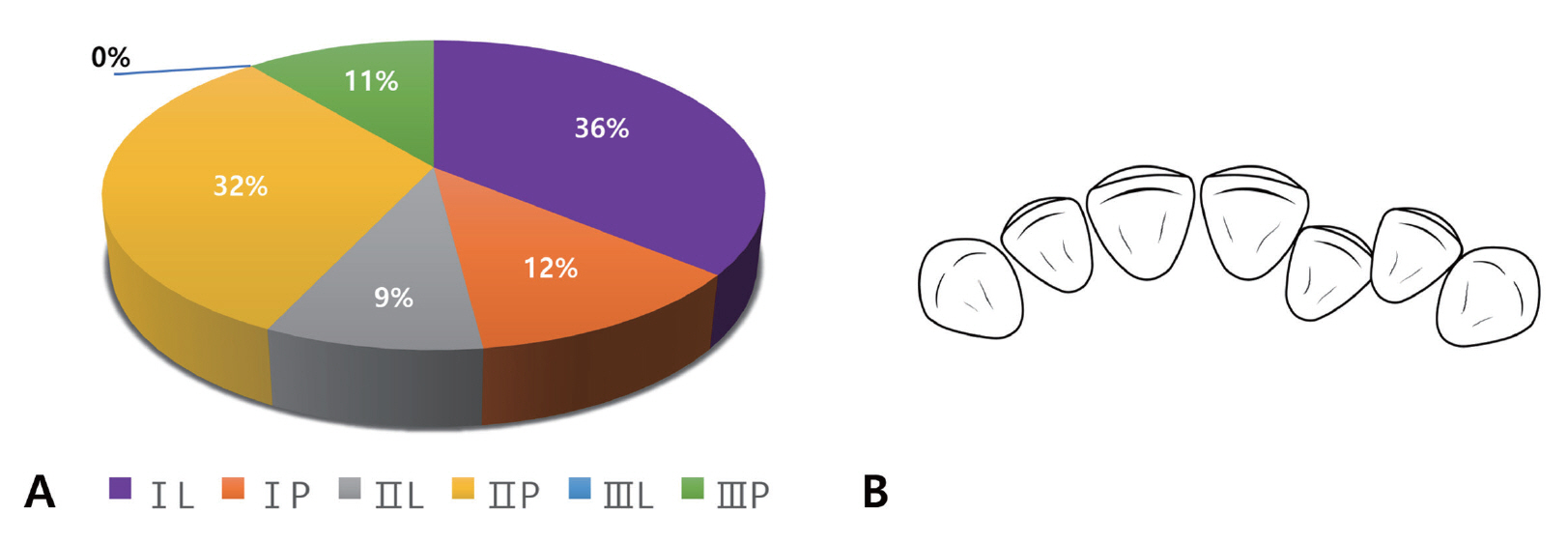
Distribution of the maxillary supernumerary lateral incisors in each region. (A) The supernumerary lateral incisors occurred the most frequently in region ⅠL (n equals 16), flowed by region ⅡP (n equals 15), region ⅠP (n equals 5), region Ⅲ P (n equals 5) and region ⅡL (n equals 4). The supernumerary lateral incisor did not exist in region ⅢL. (B) The most common alignment of supernumerary lateral incisor and adjacent lateral incisor.
3. 측절치 과잉치의 발육학적 특징
1) 측절치 과잉치의 형태 및 방향
측절치 과잉치의 형태는 보충형이 84%의 비율로 관찰되었다. 측절치 과잉치의 방향은 약 90%가 정위로 존재하였으며, 10% 비율로 회전된 방향으로 존재하였으며, 역위로 관찰되는 경우는 없었다.
2) 측절치 및 측절치 과잉치의 치관 크기
측절치 과잉치와 인접한 측절치, 반대측 측절치의 근원심 폭경을 측정하여 비교한 결과, 측절치 과잉치와 인접한 측절치 및 반대측 측절치의 치관 크기는 통계적 유의차가 있었다(p < .0001). 각 치아의 치관 크기 평균값은, 측절치 과잉치의 경우 6.17 ± 0.78, 인접한 측절치는 6.62 ± 0.66으로 나타났고, 반대측 측절치의 경우는 7.00 ± 0.48이었다. 세 치아의 근원심 폭경의 평균값을 기준으로 치관의 크기는 측절치 과잉치가 인접한 측절치보다 작았고, 인접한 측절치 또한 반대측의 정상 측절치보다 작은 것으로 관찰되었다(Table 3, Fig. 4A).

Comparative measurement of the crown size in the maxillary supernumerary lateral incisor and both lateral incisors

Comparison of mesio-distal width and Nolla stage between supernumerary lateral incisors, adjacent and opposite lateral incisors(SNLI: supernumerary lateral incisor, ALI: adjacent lateral incisor, OLI: opposite lateral incisor). (A) Mesio-distal width. (B) Nolla stage.
3) 측절치 및 측절치 과잉치의 치근 발육 단계
세 치아의 치근 발육 단계를 측정한 결과, 측절치 과잉치의 Nolla stage 평균값은 6.77 ± 1.05, 인접한 측절치의 경우 7.07 ± 1.11, 반대측 측절치의 경우는 7.36 ± 1.16로 조사되었다. 측절치 과잉치와 인접한 측절치 및 반대측 측절치는 치근 발육 단계에 있어서는 통계적으로 유의한 차이가 나타나지 않았다(p = 0.07). 세 치아의 Nolla stage의 평균값은 측절치 과잉치가 가장 작았고, 인접한 측절치, 반대측 측절치 순으로 큰 값을 보였다(Table 4, Fig. 4B).
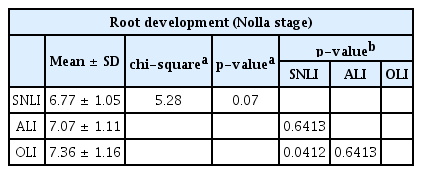
Comparative measurement of the root development in the maxillary supernumerary lateral incisor and both lateral incisors
Ⅳ. 총괄 및 고찰
측절치 과잉치는 정중과잉치처럼 상악 전치부에서 나타나지만 해부학적, 발육학적으로 다른 특징을 갖는 과잉치로, 드물게 나타나는 유형의 과잉치이다. 현재까지 많은 연구가 이루어져 있지 않기 때문에 이번 연구에서는 기존의 연구들에서 조사된 측절치 과잉치의 임상적인 특징에 대하여 통계적인 분석을 시행하고자 하였다. 추가적으로 측절치 과잉치에서는 관찰되지 않는 정상 측절치의 해부학적 구조를 확인함으로써, 임상에서 측절치와 형태학적으로 매우 유사한 측절치 과잉치를 구분하는데 있어 도움이 되고자 하였다.
남녀 43명의 CBCT사진을 분석하여 상악 측절치와 측절치 과잉치의 형태학적 및 발육학적 특징을 평가한 결과, 측절치 과잉치는 대부분 정상 맹출 방향을 갖는 보충형의 형태로 존재하였다. Jonson[11]은 측절치 과잉치에 대한 연구에서 측절치 과잉치는 87%의 비율로 보충형 형태를 갖는다고 보고하였다. 이와 같이 측절치 과잉치는 측절치와 유사한 보충형이 대부분이기 때문에 쌍생치로 분류될 수 있으나, 정상 측절치와 형태, 크기, 발육학적 특징에 있어 차이를 보인다는 점에서 단순히 쌍생치의 개념으로 접근하기보다 과잉치의 개념으로 접근하는 것이 바람직하다.
측절치 과잉치는 여러 임상적 문제를 야기할 수 있다. 첫번째, Andrei 등[12]은 측절치 과잉치가 존재하는 경우 낭성 병소, 영구전치의 이소맹출이나 맹출지연과 같은 임상적인 문제가 나타날 수 있다고 보고하였다. 두번째, 측절치 과잉치는 정상 측절치와 크기와 형태가 유사하기 때문에 임상적인 문제를 동반하지 않고 정상 맹출하는 경우 환자 및 보호자들이 과잉치를 인지하지 못하는 경우가 많다. 이처럼 과잉치가 자연적으로 맹출한 경우에도 측절치 과잉치로 인한 과도한 수평 피개, 총생 및 정중선 변위, 인접한 영구치의 회전, 변위 및 치근 형성 이상과 같은 임상적인 문제가 나타날 수 있어 주의가 필요하다[12-14].
측절치 과잉치가 존재하는 경우 과잉치의 발거와 교정적인 치료가 필요하다[6]. 또한 과잉치로 인해 이환측 견치의 맹출지연 혹은 맹출장애가 야기될 수 있으므로 과잉치의 발거 후 견치 맹출 공간을 유지하기 위한 치료가 필요할 수 있다[15]. 정중과잉치의 경우 과잉치를 발견하는 즉시 제거하는 것과 달리, 측절치 과잉치의 경우 발거할 치아에 대한 추적관찰과 신중한 판단이 필요하다. 측절치 과잉치의 치료에 있어 임상적으로 유리한 치아를 잔존시키는 것도 중요하지만, 객관적인 기준를 토대로 정상 측절치와 구분하는 것이 선행되어야 한다. 이러한 이유에서 이 연구에서는 측절치 과잉치와 측절치의 차이점을 확인하고자 하였다.
반면에, 측절치 과잉치는 측절치와 유사한 형태를 갖기 때문에 반대측 측절치의 임상적인 문제로 발거가 필요한 경우 이를 대체할 수 있다. 1979년 Taylor[16]는 좌측에 상악 측절치가 융합치이고, 우측에 측절치 과잉치가 존재하는 증례에서 좌측의 융합치를 발거하고 우측의 측절치 과잉치를 자가 이식하여 좌측의 측절치를 대체한 증례를 보고하였다. 이와 유사하게 Robertson 등[17]은 1984년 양측성의 측절치 과잉치 증례에서 상악 좌측 측절치 및 측절치 과잉치의 깊은 우식으로 인해 두 치아를 모두 발거하고 우측의 측절치 과잉치를 자가 이식하였다고 보고하였다.
이 연구에서 측절치 과잉치와 인접한 측절치 및 반대측 측절치의 근원심 폭경 수치를 통계적으로 비교 분석한 결과, 측절치 과잉치는 양측의 측절치에 비해 치관의 크기가 작았다. 이전의 연구에서 Khalaf 등[18]은 과잉치를 갖는 환자의 경우 중절치와 측절치 치관의 크기가 평균보다 크고, 중절치가 측절치보다 더 많이 영향을 받는다고 하였다. 이와 반대로 Jonson[11]은 측절치 과잉치를 갖는 환자를 대상으로 한 연구에서 인접한 측절치가 반대측의 정상 측절치보다 크기가 작은 경향이 있다고 보고하였다. 또한 Wedrychowska-Szulc와 Janiszewska-Olszowska[6]는 파노라마 영상과 진단 모형을 살펴봄으로써 측절치 과잉치는 정상 측절치보다 작다고 보고하였다.
Pamecha와 Dayakara[19]의 상악과 하악의 중절치, 측절치 및 견치의 근원심 폭경을 측정한 논문에 따르면, 상악 우측 측절치의 근원심 폭경 평균은 6.98 mm, 상악 좌측 측절치의 근원심 폭경 평균은 6.90 mm으로 양측의 측절치의 크기가 0.08 mm의 차이를 보였다. 정상 치아 개수를 갖는 경우에도 불구하고 양측의 측절치는 크기가 동일하지 않았고, 그 차이는 측절치 근원심 폭경의 1.15%였다. 이 연구에서는 측절치 과잉치와 인접한 측절치의 근원심 폭경 평균은 6.62 mm, 반대측 측절치의 근원심 폭경 평균은 7.00 mm로 0.38 mm의 차이를 보였다. 이는 측절치 근원심 폭경의 5.43%에 해당하는 수치로, 정상 치아 개수를 갖는 경우보다 양측의 측절치 간의 근원심 폭경 차이가 더 많이 나는 것을 의미한다.
측절치 과잉치와 측절치가 치아 형성 및 발육 정도에 있어서도 차이를 보이는지에 대한 조사된 연구는 적다. Nur 등[20]은 Demirjian method와 Nolla stage가 치아의 연령을 평가하는데 유효한 방법인지 분석한 연구에서 Nolla stage가 치령의 평가함에 있어 더 정확한 방법이라고 보고하였다. 이에 근거하여 이 연구에서는 과잉치와 측절치의 치령을 비교하기 위해 각 치아의 Nolla stage를 평가하여 비교 분석하였다. 연구 결과 치근 형성에 있어 측절치 과잉치와 인접한 측절치 및 반대측 측절치 간에 통계적으로 유의미한 차이를 보이지는 않았다. 이번 연구에서는 측절치 과잉치가 존재하는 경우, 과잉치뿐만 아니라 인접한 측절치 또한 치아 형성 및 발육이 느리게 나타날 것으로 예상하였으나, 표본의 수가 적어 환자의 성별이나 연령과 같은 요인에 의한 측정값의 편차가 컸기 때문에 통계적인 유의성을 확인하기 어려웠다. 향후 더 정확한 분석을 위해 많은 표본을 대상으로 하는 연구가 필요하다.
이번 연구에서는 CBCT를 이용하여 측절지 과잉치와 인접한 측절치, 반대측의 정상 측절치를 3차원적으로 분석함으로써 기존 연구에서 조사된 바 없는 측절치 과잉치와 측절치의 치관 크기 및 치근 발육 단계의 차이에 대한 통계적 유의성을 확인하였다. 측절치 과잉치는 반대측의 정상 측절치 및 인접한 측절치보다 치관의 크기가 더 작은 것으로 나타났다. 이번 연구는 후향적 연구로서 측절치 과잉치를 측절치와 객관적인 기준을 토대로 구분함에 있어 지표가 될 수 있지만, 표본이 작고 과잉치를 갖지 않는 대조군을 설정하지 않았다는 한계점이 존재한다. 정확한 진단과 치료계획을 수립하는데 참고가 되는 임상적인 가이드라인을 제시하기 위해서는 향후 정상 치아 개수를 갖는 대조군을 포함한 광범위한 표본을 대상으로 한 연구가 필요할 것으로 사료된다.
Ⅴ. 결 론
상악 측절치 과잉치는 정중과잉치와는 다른 특징을 갖는 독립적인 유형의 과잉치로, 측절치와 매우 유사하지만 점각과 구개 변연융선과 같은 정상 측절치의 해부학적 구조가 불분명하다는 점에서 구분되었다. 측절치 과잉치는 측절치에 비해 통계적으로 유의미하게 치관의 크기가 작은 것으로 나타났다. 상악 측절치 과잉치가 존재한다면 치료 계획에 앞서 측절치와 과잉치를 정확하게 구분해야 한다. 향후, 상악 측절치 과잉치의 발육학적 특징 및 유전학적 인과관계 등에 대한 보다 많은 수의 표본을 대상으로 한 연구가 필요하다.