소아청소년의 하악 대구치에서 협측소와 및 협측소와 결함의 발생 빈도
Frequency of Buccal Pits and Defective Buccal Pits in Mandibular Molars of Children and Adolescents
Article information

Abstract
협측소와는 하악 대구치 발달구의 말단에 나타나는 강한 점상의 함몰된 구조이다. 협측소와 결함은 협측소와가 상아질까지 침범한 상태로 정의할 수 있다. 이 연구는 콘빔 컴퓨터 단층촬영(CBCT) 분석을 통해 소아청소년의 하악 제1대구치 및 제2 대구치에서 협측소와 및 협측소와 결함의 발생 빈도를 조사하는 것을 목적으로 하였다. 연구는 2004년부터 2020년까지 연세대학교 치과병원 소아치과를 방문한 한국 소아청소년 417명을 대상으로 촬영한 CBCT 영상을 대상으로 수행하였다. 협측소와의 발현율은 29.1%로 보고되었다. 제4급 협측소와에 해당하는 협측소와 결함의 유병률은 총 7.9%였다. 협측소와는 양측성으로 나타나는 경향이 있었다. 이 연구는 협측소와의 빈도에 대해 가장 큰 표본 크기를 사용하여 시행한 포괄적인 연구이며, CBCT를 이용한 최초의 연구였다. 또한 협측소와 결함을 최초로 정의 내리고자 하였다.
Trans Abstract
A buccal pit is a prominent point-like depression that appears at the cervical end of the mandibular molar developmental grooves. A defective buccal pit can be defined as a buccal pit in which the continuity of the dentinoenamel junction is broken and the pit extends to the dentinal level. This study aimed to determine the frequency of buccal pits and defective buccal pits in un-erupted mandibular first and second molars using cone-beam computed tomography (CBCT). The analysis was performed on CBCT images taken from 417 Korean children and adolescents who visited the Department of Pediatric Dentistry, Yonsei University Dental Hospital between 2004 and 2020. Based on cross-sectional views of CBCT images, buccal pits were categorized into 4 classes according to the depth of the pits. The expression rate of the buccal pits was 29.1%. The prevalence of defective buccal pits was 7.9%. The buccal pits tended to develop bilaterally. To date, this is the most comprehensive study on the frequency of buccal pits with the largest sample size. This was the first attempt worldwide to analyze the depth of the buccal pit using CBCT images and to define a defective buccal pit worldwide.
Introduction
A buccal pit is a prominent point-like depression that appears at the cervical termination of the developmental grooves in the mandibular first and second molars [ 1,2].
Unlike a groove, which develops as a smooth coalescence of the lobes, a pit or fissure is formed due to faulty coalescence of the lobes during cuspal development [3]. The sealing of these sites has been emphasized to prevent pit and fissure caries [4,5]. However, class I cavity preparations are required at high rates for restoring buccal pits [6]. The common explanation for this is that food and plaque are easily trapped in buccal pits, which makes them susceptible to caries [1]. However, the cavitation of the buccal pit can be induced even before the eruption of the teeth.
In pediatric dentistry, clinicians often find buccal pits of recently erupted mandibular molars, showing a cavity-like appearance with exposed dentin (Fig. 1). In many studies that analyzed the structure of occlusal pits and fissures, it was found that the structures may extend to the dentinoenamel junction (DEJ) but never intrude the dentin [7-9]. It seems to be a unique characteristic of the buccal pit that it can protrude the dentin in some cases. In a study conducted by Jung et al. [10], the size of the pre-eruptive buccal pit radiolucency predicted the need for restoration with moderate accuracy.

Clinical photo of the defective buccal pit on mandibular second molar with partial eruption state.
Buccal pits that intrude into the dentin should be distinguished from pre-eruptive intracoronal resorption (PEIR). Although both conditions involve defective pre-eruptive lesions localized in the coronal tissue, an essential difference exists between them. PEIR is characterized by its localization within dentin [11-13], and in contrast, the buccal pit defect extends from the outer surface of the enamel to the dentin. Based on its unusual features, we suggested the term “defective buccal pit” to describe the condition in which the continuity of the DEJ is interrupted, and the pit extends to the dentinal level.
Little research has been conducted on the expression rates of buccal pits worldwide. Cone-beam computed tomography (CBCT) provides high-resolution images and enables three-dimensional imaging. The purpose of this study was to investigate the appearance rate of buccal pits and the prevalence of defective buccal pits. Additionally, we developed a definition for defective buccal pits by analyzing CBCT images. To our knowledge, this study is the first to categorize and analyze buccal pits according to their depth.
Materials and Methods
The study was approved by the Institutional Review Board (IRB) of Yonsei University Dental Hospital (IRB No: 2 - 2019 - 0079).
1. Subjects
This study was conducted on patients aged between 5 and 12 years who underwent CBCT imaging at the Yonsei University Dental Hospital between 2004 and 2020. Patients aged 7 - 12 years were included in the evaluation of mandibular second permanent molars, whereas those aged 5 - 9 years were included for the evaluation of mandibular first permanent molars. All the patients were Korean and free of any known series illnesses.
The scope was established as mentioned above, considering the age of tooth eruption and crown maturation. As patients usually begin undergoing radiography at 5 years of age, the minimum patient age was set as 5 years.
In this study, the unerupted mandibular first and second permanent molars of Demirjian stage D or higher were exclusively assessed to avoid any posteruptive impact on the buccal pits, such as acquired dental caries.
The exclusion criteria were as follows:
1) Patients with mandibular first and second permanent molars with severe tooth anomalies such as molar-incisor hypomineralization, molar-incisor malformation, and PEIR.
2) Patients having any jaw lesion (cyst or tumor) in the mandibular first and second permanent molar areas.
3) Patients with past medical history (syndromes, metabolic disease, etc) that could affect dental development. Ultimately, 417 patients (166 girls and 251 boys) were included in this study.
2. Methods
CBCT images used in the study were acquired using Alphard 3030 (Asahi Roentgen Ind., Co. Ltd., Kyoto, Japan) or Rayscan Symphony (RAY Co., Suwon, Republic of Korea). Cross-sectional views were analyzed to evaluate the depth of the buccal pit. Cross-sectional views were perpendicular to the curved dental arch and the slice thickness was 1.0 mm. A cross-sectional view with the slice showing the deepest buccal pit was selected for analysis of each tooth. Assuming the uppermost point of the orifice of the buccal pit to be U and the lowermost point of the orifice to be L, a line connecting U and L (U-L line) was assumed. The vertical distance from the U-L line to the DEJ was denoted as the V-DEJ. The vertical distance from the U-L line to the deepest point of the buccal pit was termed the V-buccal pit (Fig. 2). The ratio between the V-DEJ and V-buccal pit was analyzed, and used to
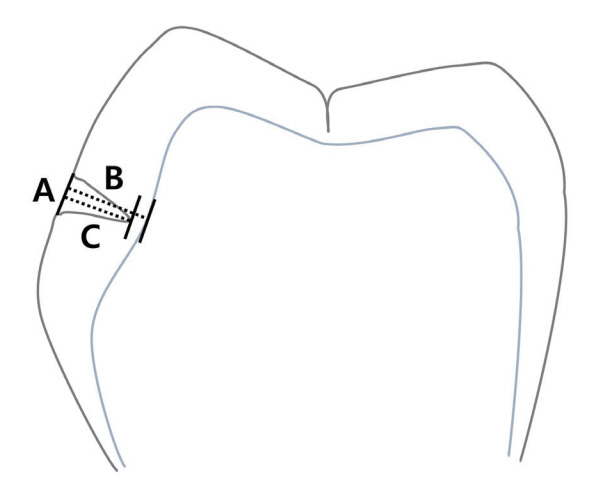
Detection of a buccal pit. (A) the line connecting the uppermost point and the lowermost point of the buccal pit (U-L line), (B) the vertical distance from the U-L line and DEJ (V-DEJ), (C) the vertical distance from the U-L line to the deepest point of the buccal pit (V-Buccal pit).
classify the buccal pit as follows:
Class I: Ratio below 1/3.
Class II: Ratio between 1/3 and 2/3.
Class III: Ratio above 2/3; however, the buccal pit did not reach the DEJ.
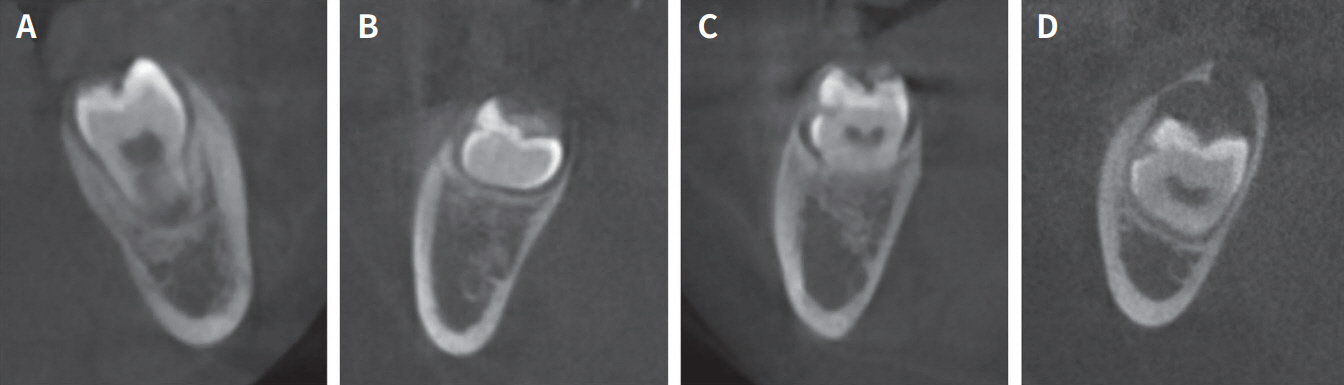
Class IV: Continuity of the DEJ was broken, and the buccal pit extended to dentin (Fig. 3).

Classification of the buccal pit by its depth. (A) Class l: The ratio between V-Buccal pit and V-DEJ is below 1/3, (B) Class ll: The ratio was between 1/3 and 2/3, (C) Class lll: The ratio was above 2/3, but the depth of the buccal pit did not reach the DEJ, (D) Class lV: Continuity of the DEJ is broken and the buccal pit extends to dentin area.
A skilled observer performed the radiographic analysis. Before the experiment, the buccal pits were analyzed and classified twice at two-week intervals to evaluate intra-observer reliability. Twenty randomly selected CBCT images with buccal pits were used in the analysis. The intra-observer reliability was represented by Cohen’s kappa coefficient and set to 0.95.
3. Statistics
Statistical analyses were performed using SPSS (version 35.0.0, SPSS, Chicago, IL, USA). The chi-square test and Fisher’s exact test were applied to compare the expression rates of the buccal pits between sexes, the right and left quadrants, and different types of teeth. The prevalence of defective buccal pits was analyzed using the same method. The relative risk was estimated to assess the risk of bilateral tendencies. The Kruskal-Wallis test was performed to compare the distribution of buccal pits according to the classes by tooth type.
Results
1. Appearance rate of the buccal pit
Of the 416 patients, buccal pits were observed in 121 (29.1%) patients, representing 195 (23.7%) out of 822 teeth.
The appearance rates in boys and girls were 29.2% (73 out of the total 250 boys) and 28.9% (48 out of the total 166 girls), respectively, which was not statistically significant. Among the teeth with buccal pits, 119 were found in boys (23.5%) and 76 were found in girls (24.1%); the difference in the appearance rate was also not statistically significant (Table 1).

Expression rate of the buccal pit based on gender
The distribution of buccal pit in each mandibular molar is presented in Table 2. There was no significant difference in the appearance rate between the right and left sided teeth or between the different types of molars.

Distribution of each mandibular molar with the buccal pit
Among the subjects with bilaterally unerupted second molars, 57 (21.7%) developed buccal pits bilaterally, a higher rate than that associated with unilateral appearance (16.3%). Moreover, among subjects with bilateral unerupted first molars, 12 (26.7%) developed buccal pits bilaterally, a higher rate than that associated with unilateral appearance (15.5%). Both results were statistically significant (Table 3, p < 0.0001 for the second molar and p < 0.0001 for the first molar). If a buccal pit occurred on the mandibular first and second molars, the risk of developing buccal pits on the opposite molars was 7.25 and 6.99 times greater, respectively.

Distribution of symmetrical pattern of the buccal pit among subjects with both un-erupted right and left molars
Of the 51 subjects with unerupted first and second permanent molars, 12 (23.5%) developed buccal pits on a single tooth type, and 8 (15.7%) developed buccal pits on both types of teeth simultaneously (Table 4, p = 0.05). If buccal pits were present on the mandibular first molars, the risk of developing buccal pits on the mandibular second molars was 4.38 times greater.
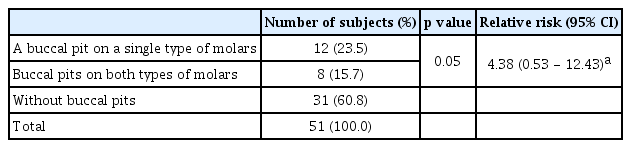
Distribution of simultaneous expression of the buccal pit on first and second molars among subjects with both un-erupted first and second molars
2. Classification of the buccal pit
The distribution of buccal pits according to the classification is shown in Table 5. Among all teeth with buccal pits, the proportions of class I, II, III, and IV buccal pits on the permanent mandibular molars were 17.9%, 28.7%, 32.3%, and 21.0%, respectively. No statistically significant differences were found in the distribution of the 4 types of teeth (Table 5, p = 0.792). However, because some groups were small, the possibility of a type 2 error in the statistics should not be excluded. The highest percentage of class IV (defective) buccal pits occurred in the left first permanent molar.
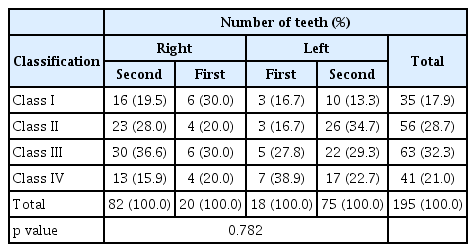
Distribution of the buccal pits by classification among the teeth with buccal pits
The distribution of buccal pits according to sex is presented in Table 6. The occurrence rates of class III and class IV buccal pits were higher in boys (58.0%) than in girls (46.1%). Nevertheless, there was no statistically significant difference in the distribution of all classes (Table 6, p = 0.054).
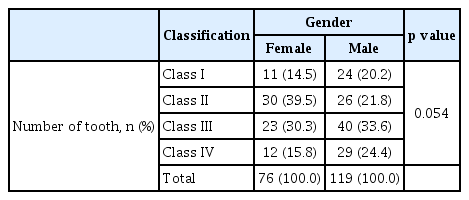
Distribution of the buccal pits by classification among the teeth with buccal pits in each gender
3. Prevalence of the defective buccal pit
Defective buccal pits, corresponding to class lV buccal pits, were observed in 33 (7.9%) of the 416 patient, representing 41 (5.0%) of the 822 teeth (Table 5 - 7).
No significant difference in the prevalence of buccal pits was observed between boys 8.8% (22 of 250) and girls 6.6% (11 of 166). Of the total number of teeth with buccal pits, 29 were observed in boys (5.7%) and 12 in girls (3.8%), demonstrating no significant difference in prevalence (Table 7).

Prevalence of the defective buccal pit based on gender
The distribution of the mandibular molars with defective buccal pits is presented in Table 8. The percentage of second permanent molars with defective buccal pits was 4.3% (30 out of 682 teeth), and the percentage of first molars with defective buccal pits was 7.8% (11 out of 140 teeth), which is a much higher result. However, this difference was not statistically significant (Table 8, p = 0.087).

Distribution of each mandibular molar with the defective buccal pit
Discussion
In this study, the expression rate of buccal pits and prevalence of defective buccal pits in the mandibular first and second molars were investigated in children who visited Yonsei University Dental Hospital.
The occurrence of buccal pits is closely associated with the molar pattern. During the development of the molar pattern, secondary enamel knots act as signaling centers that interact with the mesenchyme, leading to the folding of the inner enamel epithelium for cuspal development until all cusps coalesce [14]. Cells proliferate outside the enamel knot and apoptosis occurs inside the knot, causing an interruption in cell signaling. The timing of apoptosis is known to influence the shape and size of the cusp, and consequently determines the shape of the pits and fissures [15,16]. Symons et al. [17] suggested that narrower angles between cuspal inclines resulted in deeper fissures.
A characteristic of buccal pits is that they typically develop farther from the signal center than occlusal pits do. Since the duration of enamel deposition decreases as the distance from the signal center increases, the increased distance may be related to the formation of defective buccal pits. However, the mechanism underlying defective buccal pit formation remains unclear.
Histological studies on pits and fissures have provided more information. It has been found that the interior of pits and fissures is composed of ameloblasts and some red blood cells. Crowded ameloblasts in the fissure area are subjected to pressure during cuspal development. The cells are prevented from matrix production and maturation, they fail to converge with other enamel organs to form a reduced enamel epithelium, and remain entrapped resulting in pits and fissures [18]. This is consistent with the findings of Awazawa [19] and Gwinnett [20], who revealed the hypomineralization of the fissure floor.
The terminology for dentin intrusion by buccal pits must be carefully considered. In this study, the defective buccal pits lacked enamel but they also invaded dentin. Although both enamel and dentin were affected, this phenomenon appears to be more analogous to enamel hypoplasia. Enamel hypoplasia means a deficiency of enamel and usually indicates a reduction in the quantity of enamel, sometimes exposing the underlying dentin [ 21,22]. Histological studies have been conducted that could explain the dentinal changes under hypoplastic areas. The reports revealed that the DEJ is often bent and altered in the hypoplastic area [22,23]. Moreover, it is well known that the ameloblast plays an important role for differentiation of the odontoblast and initial dentin formation [24]. Nevertheless, the histological analysis of buccal pits alone can verify the mechanism of the phenomenon; therefore, the term “Defective Buccal Pit” was chosen in this study.
Few studies have been published on the frequency of buccal pits. Pfeiffer [1] studied the frequency of erupted mandibular molars in a Kleinburg ossuary population (approximately 1600 AD). In her study, the number of teeth with buccal pits was significantly lower after 18 years of age than that in younger patients. The study concluded stating that teeth with buccal pits are most likely to be lost. The calculated expression rates were 20.4% for the right first molar, 19.4% for the left first molar, 21.8% for the right second molar, and 22.4% for the left second molar. The rates in the study were slightly higher for the second molars, which is inconsistent with the results of the present study. However, since the study was based on an ossuary population, and the post-eruptive effect was not excluded, a direct comparison with the present study is difficult.
According to a study by Oh [2] on the shape and size of the mandibular molar crown, teeth with deep developmental grooves comprised 82% of the first molars and 64% of the second molars, and teeth with buccal pits comprised 35% of the first molars and 20% of the second molars.
In the present study, the frequency of buccal involvement was 29.1% with the occurrence in the first molars(27.1%) being higher than that in the second molars(23.0%), which is consistent with the findings of Oh [2]. There were no sex-based differences, and the buccal pits showed bilateral characteristics. When expressed on one side, there was a high risk of developing buccal pits on both sides (RR, 7.25: first molars and RR, 6.99: second molars). In addition, a high risk of developing buccal pits occurred in the second molars when the first molars already had buccal pits (RR, 4.38).
To our knowledge, this is the first study to investigate the depth of buccal pits before eruption. Pitting extending to the dentin is a phenomenon observed only in buccal pits and not in occlusal pits. Therefore, the depth of the pit was identified as an important factor affecting the susceptibility to caries in the buccal pit. By analyzing the cross-sectional views, buccal pits were classified into 4 categories, and it was verified that some of the buccal pits lost their enamel base and invaded the dentin (Fig. 4). These buccal pits were defined as defective buccal pits.
The cross-sectional view of (A) a molar without a buccal pit, (B) a molar with a buccal pit and (C, D) a molar with a defective buccal pit.
The prevalence of defective buccal pits was 7.9%, with no statistically significant difference according to sex. The prevalence of defective buccal pits in the first molars was higher than that in the second molars; however, this difference was not statistically significant.
Although depth is an important factor for caries susceptibility, other factors should also be considered. Deep pits and fissures in the occlusal area are usually I- or Kshaped, with relatively narrow width. V- or U-shaped occlusal pits and fissures are wide and shallow; therefore, they are self-cleansing [4]. This implies that the width and shape should also be considered when evaluating buccal pit characteristics. However, in this study, depth was the only criterion used for classification. Therefore, further studies are required.
Jung et al. [10] measured the radiolucent area of buccal pits in pre-eruptive mandibular first molars using panoramic views. The correlation between the size of the buccal pit radiolucency and need for restoration after eruption was investigated. The ratio of the buccal pit area to the total crown area was 2.225 ± 1.695‰ in the experimental group and 0.121 ± 0.968‰ in the control group (p < 0.001). Therefore, it was proven that the larger the radiolucent area, the higher is the probability of the tooth requiring a restoration after eruption.
A limitation of this study was that the depth of the buccal pit was the only criterion for classification, and the width or shape of the pit was not considered. Since cross-sectional views cannot accurately represent the morphology of buccal pits, other methods should be considered in future studies. In addition, the sample size, particularly the number of unerupted first molars, was insufficient. The possibility of a type 2 error should not be excluded in this study. Finally, as this was a retrospective study that analyzed cross-sectional views and the interval between the slides was set to 1mm, buccal pits may have been underestimated. Defective buccal pits and the deepest point of the buccal pits may have been missed between the slides.
Future studies will require a larger sample size and analysis of the morphology and volume (including width and depth) of the buccal pits. In addition, histological and biological studies on the occurrence of buccal pits are necessary.
Conclusion
The purpose of this study was to investigate the expression rate of buccal pits, and the prevalence of defective buccal pits in the mandibular first and second molars of children who visited Yonsei University Dental Hospital. The following conclusions were drawn from the retrospective analysis of CBCT radiographs.
The expression rate and prevalence of buccal pits were 29.1% and 7.9%, respectively. Buccal pits tended to appear bilaterally or simultaneously on different types of molars. Since restoration is often required for buccal pits immediately after tooth eruption, especially if they are defective buccal pits, clinical assessment of buccal pits on mandibular molars is essential. Clinicians should understand the anatomical characteristics of buccal pits to achieve an optimal diagnosis and treatment plan.
Notes
Conflict of Interest
The authors have no potential conflicts of interest to disclose.
Funding information
This study was supported by the student research fund from Oral Science Research Center, College of Dentistry, Yonsei University (2-2019-0079)
Acknowledgements
This study was supported by the student research fund from Oral Science Research Center, College of Dentistry, Yonsei University (2-2019-0079).