유치의 탈구성 손상에 관한 후향적 분석: 고정술의 치료 결과
A Retrospective Study of Luxation Injuries in Primary Teeth: Prognosis with Splinting
Article information
Abstract
본 연구의 목적은 탈구성 손상을 받은 유치에 시행한 고정술의 치료 결과를 분석하는 것이다. 본 연구는 2010년부터 2015년까지 탈구성 손상으로 본과에 내원하여 유치에 고정술을 시행한 92명의 환아들을 후향적으로 분석하였다. 이들 중에서 6개월 이상 추적 검사에 참여한 환아들을 대상으로 치료 결과를 분석하였다. 치료 결과는 검진 기간동안 임상 및 방사선 검사에서 합병증의 존재에 따라 분석되었다.
평균 나이는 42.1개월이었으며 67.4%가 남아였다. 넘어짐이 가장 빈번한 원인이었으며, 평균 고정 기간은 2.4주이었다. 고정술의 성공률은 58.9%이었다. 아탈구가 가장 높은 성공률을 보였으며, 측방 탈구에서 정복 후 고정술을 시행한 경우 가장 낮은 성공률을 보였다. 탈구성 손상에서 치수괴사가 가장 빈번히 발생한 비호의적 치료 결과이었다.
본 연구결과, 유치의 탈구성 손상에서 고정술은 받아들일 만하였으며, 고정술은 유치의 탈구성 손상시 치료법으로 고려될 수 있다.
Trans Abstract
This study investigated the prognosis of luxation injuries in primary teeth treated with splinting. This study retrospectively analyzed 92 children with luxation injuries to their primary teeth who were treated with splints between 2010 and 2015. Prognoses were analyzed in patients who had been followed for more than 6 months. The prognoses with splinting were based on clinical and radiographic evaluations performed during the follow-up examinations.
The mean patient age was 42.1 months, and 67.4% were male. The most common cause of luxation injury was falling, and the mean splint duration was 2.4 weeks. The success rate of splinting was 58.9%. The highest rate of success was achieved following subluxation, while repositioning and splinting of lateral luxation had the lowest rate of success. Pulp necrosis was the most common unfavorable prognosis in the luxation injuries.
Depending upon the type of luxation, splint therapy had acceptable prognoses and might be a feasible treatment option.
I. Introduction
Luxation injuries comprise a large proportion of traumatic dental injuries (TDIs) in primary teeth, due to the resilience of alveolar bone [1]. Various luxation injuries are possible depending upon the force and direction of impact. Treatment methods vary according to the type of injury [1].
One of the treatments for stabilizing traumatized teeth is splinting, which allows periodontal tissue regeneration while providing protection from further injury. Flexible or semi-rigid fixation is sufficient for healing pulp and periodontium in most TDIs, and rigid fixation is recommended for cervical root fractures [1-3]. When ankylosis is not a significant risk, a fixation period of 2 - 3 weeks is recommended [1]. Following injuries to the bone, however, 1 - 2 additional weeks are required [4].
The International Association for Dental Traumatology (IADT) guidelines recommend splinting of the primary teeth only for alveolar bone fractures and root fractures [5]. Moreover, repositioning and splinting of traumatized primary teeth requires caution regarding the permanent successors [1].
Despite the significance of primary tooth injuries, few studies have examined this topic. Recently, however, trials have examined the splinting of traumatized primary teeth following alveolar process fracture, horizontal root fracture, and lateral luxation [6-9]. To advance our knowledge of TDIs, such trials are important, and should be continued. The purpose of this study was to evaluate the prognoses of luxation injuries following the splinting of primary teeth.
II. Materials and Methods
This study was performed in the Department of Pediatric Dentistry, School of Dentistry, Kyung Hee University, Seoul, Korea. The study proposal was reviewed and approved by the Ethics Committee (KHD IRB 1606-4). This study retrospectively analyzed the medical records of children who were treated using splints on their primary teeth between 2010 and 2015. A total of 838 patients (1534 teeth) visited our department for treatment of luxation injuries of their primary teeth. Of these, 92 patients (202 teeth) were treated using splints and selected for reevaluation. Among the 92 patients, 79 patients were treated with flexible round stainless steel wire (SS-GFS; Ormco, Orange, CA, USA) and flowable composite resin. Nine patients were treated with monofilament nylon fishing line (FL-GFS; HL-1553, HDF, Busan, Korea) and flowable composite resin. In two patients, the teeth were splinted with flexible tri-flex stainless steel wire (TF-RS; RMO, Denver, CO, USA) and flowable composite resin. In the others, the teeth were fixed with flowable composite resin.
Clinical records, intraoral photographs, and radiographs were assessed. Radiographic data were collected to evaluate the prognoses with splinting. Data were analyzed according to age, gender, cause of injury, type of TDI, splinting method, and fixation period. Patients with incomplete records or radiographic examinations were excluded.
Luxation injuries were classified into concussion, subluxation, intrusive luxation, extrusive luxation, lateral luxation, and avulsion [1,10]. Treatment prognoses were analyzed in 57 patients (124 teeth), with a follow-up period exceeding 6 months. Prognoses were categorized based on the presence of associated complications in the clinical and radiographic examinations. Favorable prognoses had total or partial pulp canal obliteration, without complications [5]. Unfavorable prognoses included pulp necrosis, pathological root resorption, loss of teeth, ankylosis, and pathological bone resorption [1]. Success rates were calculated as the ratio of teeth with favorable prognoses to the total number of traumatized teeth in each group.
III. Results
The study population consisted of 62 boys and 30 girls (sex ratio 2.07 : 1). The average age was 42.1 ± 17.4 months, and the most prevalent age was 4 - 5 years, followed by 2 - 3 years. Table 1 shows the distribution of splinting in primary teeth by age and gender.

Distribution of splinting in primary teeth by age and gender
The main cause of injury was falling (53.3%; Fig. 1); the most common place of injury was in the home (42.4%). All teeth treated by splinting were anterior teeth; the primary maxillary central incisor (67.7%) was the most commonly injured tooth. Table 2 shows the rates of splinting among the primary teeth. The highest rate of splinting was in extrusive luxation (28.9%), followed by lateral luxation (22.2%). The mean duration of splinting was 2.4 weeks (Table 2).
Distribution of splinting in primary teeth according to cause and age.
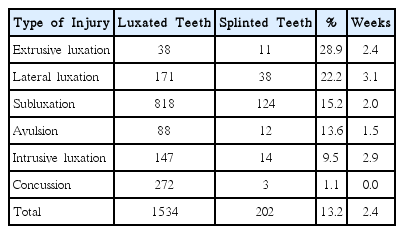
Rate of splinting in luxation injuries and mean splint durations
The total number of teeth analyzed was 124, and complications were diagnosed within an average follow-up period of 22.1 ± 14.5 months. The success rate of splinting was 58.9%; subluxation injuries had the highest success rate. Conversely, repositioning and splinting of lateral luxation injuries resulted in the lowest success rate (Fig. 2).

Treatment prognoses for splinting of primary teeth.
Pulp necrosis (16.1%) was the most common complication. The distribution of complications is shown in Table 3.
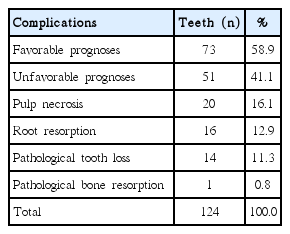
Distribution of complications
IV. Discussion
Traumatic dental injuries of primary teeth have a prevalence of approximately 30 - 40% [11-13]. In addition, luxation injuries are more frequent in primary teeth than are fractures [1,14]. Despite the prevalence of TDIs, few studies have examined splinting treatment in primary teeth. Therefore, this study focused on luxation injuries in primary teeth treated using splinting.
The predominant age group in this study was 4 - 5 years (Table 1). This was in agreement with studies that found an increased incidence of TDIs in children between the ages of 3 and 5 years [15-17]. However, this finding disagreed with other studies reporting that the peak age of TDI incidence in children is 2 - 4 years [1,15,18,19].
Boys had a higher incidence of injury than girls (2.07 : 1), which was consistent with other studies [11,18,20,21] and may reflect the observation that boys are more energetic and more likely to take part in outdoor activities than girls are [22]. The predominant age of boys in the series was 4 - 5 years, while that of girls was 2 - 3 years. This was in agreement with study that found the predominant age of boys was older than that of girls [17].
The most common cause of the injuries was accidental falls (Fig. 1). Falls and collisions accounted for 90% of cases, consistent with previous reports [18,21,23-25]. The most common location for TDIs to occur was the home, followed by the kindergarten classroom. This was also consistent with previous studies [18,23,24].
The rate of splinting of luxation injuries was 13.2% (Table 2). One study reported that 9% of luxated primary teeth were treated using splinting [26]. Splinting can decrease the initial mobility of teeth and related pain, and may prevent children from touching their mobile teeth [8].
The current guidelines recommend splinting of traumatized primary teeth only following root displacement and alveolar bone fractures [5]. Andreasen et al. [1] recommended a splint for 2 - 3 weeks in the case of luxation with occlusal interference. In agreement with this suggestion, the rates of splinting in extrusive and lateral luxation injuries were higher than those in other luxation injuries.
Traumatic dental injuries in the primary teeth can cause clinical complications, including color changes, pulp necrosis, pulp canal obliteration, external root resorption, and internal root resorption [1]. Favorable and unfavorable prognoses were identified based on the literature [5,19]. The frequency of secondary pulp necrosis among teeth with pulp canal obliterations is low [1,14,27-29]. Consequently, partial or total pulp canal obliteration was considered a clinical success. Unfavorable prognoses included pulp necrosis, pathologic root resorption, loss of tooth, and pathologic bone resorption.
The average success rate for splinting was 58.9% (Table 3, Fig. 2). As reported, severe periodontal tissue injuries resulted in complications [19,30]. Lateral, intrusive, and extrusive luxation injuries had lower success rates than other injuries. The replantation of avulsed primary teeth is usually not recommended based on the potential damage to permanent successors [1,5]. However, the success rate with avulsed teeth was high in this study, although this finding may have been biased due to the small sample size.
V. Conclusions
In this study, the highest rate of splinting following luxation injuries occurred in cases of extrusive luxation. The success rate of splinting luxated primary teeth was 58.9%, with subluxations having the highest success rates. This was the first study to investigate the clinical prognoses of splinting in luxated primary teeth, and could be the basis for additional studies investigating TDIs in primary teeth.