


Ⅰ. Introduction
The ultimate goal of orthodontic treatment is to achieve and maintain optimal function and aesthetic appearance[1]. It is crucial to take into account both the functional and aesthetic improvement when making an orthodontic diagnosis or establishing a treatment plan. When observing the soft tissues in profile, the appearance of the face is the most important aspect to evaluate[2].
Many reports have already acknowledged the importance of the soft tissues in orthodontic treatment[3-7] and attempted to apply these principles to clinical practice. Tweed[3] considered that the mouth plays an important role in portraying the beauty and character of the face. According to Tweed[3], the shape and esthetics of the lips are affected by the occlusal relationships of the teeth and are closely related to the changes in the inclination of the mandibular incisors relative to the basal bone.
The Tweed triangle is used in clinical practice based on this principle. Ricketts[4], Merrifield[5], and Peck and Peck[6] have studied aesthetic aspects of the facial soft tissues, while Holdaway[7] used soft tissue analysis to demonstrate the irrationality of utilizing only hard tissue analysis when establishing an orthodontic treatment plan.
With regard to the relationship between the retrusion of the maxillary and mandibular incisors and the upper and lower lips, a large number of studies have been conducted to establish a ratio between posterior movement of the lips and the incisal edge of the anterior teeth[8-12]. Jacobs et al .[12] reported a ratio of 0.7 : 1 for the movement of the upper lip and retraction of the maxillary incisors and a ratio of 1 : 1 for the movement of the lower lip and retraction of the mandibular incisors. The latter is known to be less predictable than the former. Caplan and Shicapuja[13] reported ratios of 1.75 : 1 and 1.2 : 1 for the retraction of the upper and lower lips, respectively, depending upon the retraction of the upper and lower incisors in African Americans. In a study on Japanese participants, Yasutomi et al .[14] reported these ratios to be 1.85 : 1 and 1.32 : 1.
The soft tissue profile is determined by multiple factors, including growth of the facial skeleton, growth of the nose, and the inclination of the teeth. Pediatric dentistry, in particular, requires awareness of changes in the growth of soft and hard tissues, because children are continually growing and their facial appearance is constantly changing. Nanda et al .[15] examined changes in the facial appearance of children aged 7 - 18 years and presented patterns of change in soft tissues by age and sex.
Furthermore, previous findings on changes in the facial soft tissue profile with age or its relationship with inclination of the incisors following orthodontic treatment have been reported. However, only a few studies have addressed the relationship between the soft and hard tissues in developing children who have not undergone orthodontic treatment; there are especially very few studies on Korean children.
Therefore, this study aimed to investigate the correlations between the anterior and posterior inclination of the maxillary and mandibular teeth, which are part of the facial hard tissues, and the lower-nasolabial angle (L-nasolabial angle) and mentolabial angles, which are part of the facial soft tissues. To this end, measurements from cephalometric radiographs was analyzed, checked for statistical significance, and assessed whether the results would be useful for orthodontic diagnosis.
Ⅱ. Materials and methods
1. Study participants
Subjects consisted of 375 children (181 boys and 194 girls), aged 7 - 11 years, who had undergone cephalometric radiography at Wonkwang University Dental Hospital between January 1, 2003 and December 31, 2015. The 22 patients for meeting the exclusion criteria, which included a history of orthodontic treatment or current orthodontic treatment, or having a craniofacial deformity such cleft lip and palate were excluded. All participants were classified into skeletal class I, Ⅱ, or Ⅲ malocclusion (Table 1).
1) Cephalometric radiograph analysis
The following landmarks and measurements were used in this study:
(1) Landmarks
① Hard tissue landmarks (Fig. 1)
Nasion (N) : Most anterior point in frontonasal suture
Subspinale (A) : The greatest concavity of the maxilla between anterior nasal spine and the maxillary dental alveolus
Supramentale (B) : The greatest concavity of the mandible between infradentale and pogonion
Porion (Po) : Most superior point of outline of external auditory meatus
Orbitale (Or) : Most inferior point on margin of orbit
Gonion (Go) : Most posterior inferior point on angle of mandible
Gnathion (Gn) : The most anterior-inferior point on the mandibular symphysis
Root apex of upper incisor (Ur)
Incisor superius (Is)
Incisor inferius (Ii)
Root apex of lower incisor (Lr)
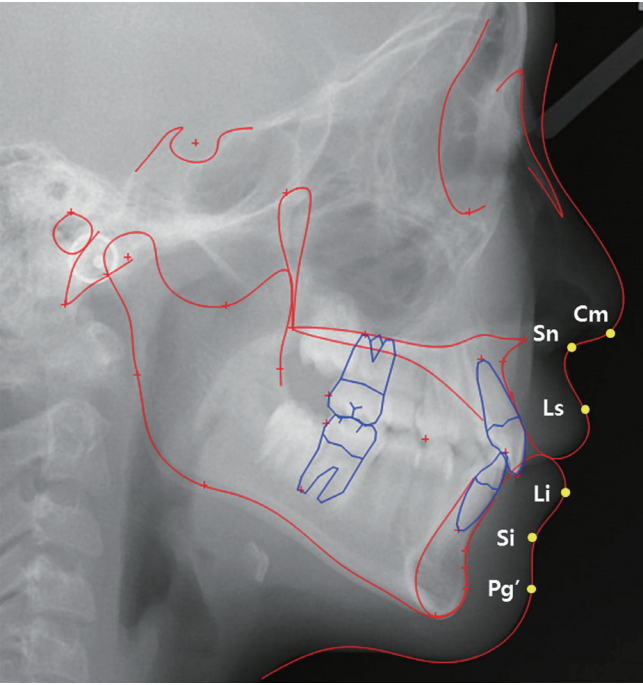
② Soft tissue landmarks (Fig. 2)
Columella point (Cm) : The most anterior point on the columella of the nose
Subnasale (Sn) : The point of convergence of the nose and the upper lip
Labrale superius (Ls) : The most anterior point on the convexity of upper lip
Labrale inferius (Li) : The most anterior point on the convexity of the lower lip
Sulcus inferius (Si) : The point of greatest concavity in the midline between the lower lip and soft-tissue chin
Soft tissue pogonion (Pg') : The most anterior point of the soft-tissue chin
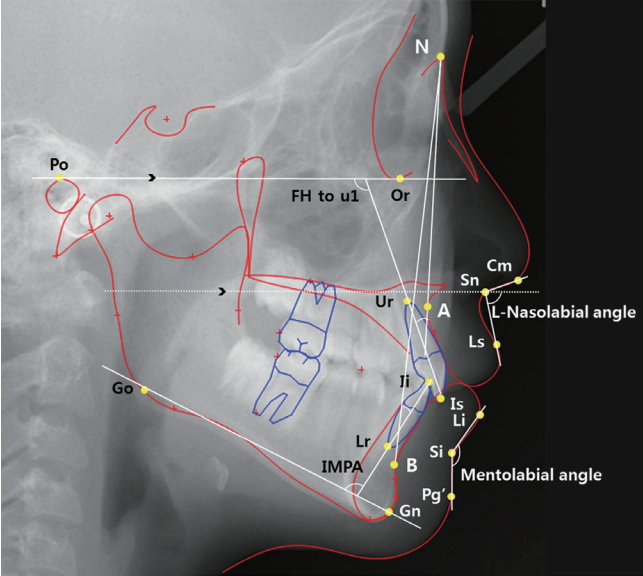
(2) Measurements (Fig. 3)
Frankfort horizontal plane (FH) : Orbitale-porion horizontal line
Upper incisor angle : Angle of Ur-Is line (U1) to FH, angle of U1 to NA line
Lower incisor angle : incisor-mandibular plane angle (IMPA), angle of Ii-Lr (L1) to NB line
Lower-nasolabial angle (L-nasolabial angle) : Angle of FH plane to Sn-Ls line
Mentolabial angle : The angle between Li and Si and Pg'
Upper lip thickness (ULT) : Length of A point to Sn
Upper lip length (ULL) : Length of Ls to Sn
Lower lip thickness (LLT) : Length of B point to Si
Lower lip length (LLL) : Length of Li to Si
The inclination of the maxillary incisors was calculated by measuring the angles of the long axis of the maxillary central incisor with the FH plane and with the NA line. The inclination of the mandibular incisors was calculated by measuring the angles of the long axis of the mandibular central incisor with the Go-Gn line and with the NB line. For the assessment of the inclination of the upper lip, the lower-nasolabial angle was measured with reference to the FH plane to eliminate any individual differences in nasal growth and inclination. Mentolabial angle was assessed by measuring the angles between Li, Si, and Pg’.
Since previous studies have shown that lip length and thickness can affect the inclination of the lips, the length and thickness of the upper and lower lips were measured. The thickness of the upper lip was measured as the length of the line connecting A Point and Sn, while the length of the upper lip was measured as the length of the line connecting Ls and Sn. The thickness of the lower lip was measured as the length of the line connecting B Point and Si, while the length of the lower lip was measured as the length of the line connecting Li and Si.
2) Statistical analysis
A single investigator used the Vceph™ 6.0 (Osstem Implant, Korea) to identify and measure landmarks on the cephalometric radiographs and to evaluate and record the results. Statistical analyses were conducted using Windows SPSS 18 (IBM, USA) with a significance level set at 5%. The Kruskal-Wallis test and Mann-Whitney test were performed, depending upon the classification of skeletal malocclusion. A Pearson correlation test was performed to investigate the correlations between the inclination of the incisors and the lower-nasolabial and mentolabial angles. Partial correlation analysis was performed to eliminate the effects of lip thickness and length, and a multiple regression analysis was performed to verify the correlation with various factors.
Ⅲ. Results
1. Comparison of the measurements depending upon the classification of skeletal malocclusion
Table 2 shows the means of all measurements in relation to the classification of skeletal malocclusion. FH to U1, which represents the inclination of the upper incisor, significantly differed between class Ⅱ and Ⅲ malocclusion groups, while U1 to NA significantly differed across all groups. IMPA and L1 to NB, which represent inclination of the lower incisor, significantly differed across all groups. L-nasolabial angle significantly differed between the class Ⅱ and Ⅲ malocclusion groups, while mentolabial angle significantly differed between class I and Ⅱ malocclusion groups and between class Ⅱ and class Ⅲ malocclusion groups.
2. Correlation between the inclinations of the incisors and lips in relation to the classification of skeletal malocclusion
FH to U1 had a significant negative correlation with Lnasolabial angle (r = -0.333, p < 0.001) in the skeletal class I malocclusion group, and U1 to NA had a significant negative correlation with L-nasolabial angle (r = -0.179, p < 0.05), suggesting that L-nasolabial angle is more strongly associated with FH to U1 than with U1 to N1. IMPA and L1 to NB were negatively (p < 0.01) and positively correlated with mentolabial angle, respectively. However, the latter correlation was not statistically significant, showing that the IMPA is more strongly correlated with the mentolabial angle than L1 to NB (Table 3).
FH to U1 had a significant negative correlation with Lnasolabial angle (r = -0.261, p < 0.01) in the skeletal class Ⅱ malocclusion group, and U1 to NA also had a significant negative correlation with L-nasolabial angle (r = -0.189, p < 0.05), suggesting that L-nasolabial angle is more strongly associated with FH to U1 than with U1 to N1. IMPA and L1 to NB were negatively correlated with the mentolabial angle; however, only the latter correlation was statistically significant (r = 0.489, p < 0.001), indicating that L1 to NB has a stronger correlation with the mentolabial angle than IMPA does (Table 3).
FH to U1 had a significant negative correlation with the L-nasolabial angle (r = -0.483, p < 0.001) in the skeletal class Ⅲ malocclusion group, and U1 to NA also had a significant negative correlation with the L-nasolabial angle (r = -0.308, p < 0.05), suggesting that L-nasolabial angle is more strongly associated with FH to U1 than with U1 to N1. IMPA and L1 to NB were negatively correlated with the mentolabial angle; however, the correlation was not statistically significant (Table 3).
Partial correlation analysis considering the thickness and length of the lips revealed a higher correlation coefficient with the inclinations of the upper incisors and lips than the inclinations of the lower incisors and lips, regardless of the classification of skeletal malocclusion. This suggested that the thickness and length of the lips have a greater impact on the inclination of the upper lips (Table 4).
3. Regression analysis for the correlation between the inclinations of the incisors and lips
Regression analysis revealed that FH to U1 has a significantly greater association with L-nasolabial angle than U1 to NA. Moreover, ULT had a significantly greater impact on L-nasolabial angle than U1 to NA in the skeletal class I malocclusion group. IMPA was more strongly associated with mentolabial angle than N1 to NB was, while LLT and LLL had no significant correlations (Table 5). The explanatory powers of the multiple regression model for L-nasolabial angle and mentolabial angle were 30.2% and 18.6%, respectively, in the class I malocclusion group.
In the skeletal class Ⅱ malocclusion group, FH to U1 had the strongest association with L-nasolabial angle, followed by ULT, ULL, and U1 to NA. Unlike in the class I malocclusion group, N1 to NB had a greater impact on the mentolabial angle than IMPA did (Table 6). The explanatory powers of the multiple regression model for L-nasolabial angle and mentolabial angle were 21.9% and 37.6%, respectively, in the class Ⅱ malocclusion group.
In the skeletal class Ⅲ malocclusion group, FH to U1 had the greatest impact on L-nasolabial angle, and the remaining variables had similar levels of impact. Results pertaining to mentolabial angle were similar to those in the class I malocclusion group (Table 7). The explanatory powers of the multiple regression model for L-nasolabial angle and mentolabial angle were 44.3% and 15.6%, respectively, in the class Ⅲ malocclusion group.
Multiple regression results in relation to skeletal classification were similar across all three groups; however, ULL had no significant impact on the L-nasolabial angle in class I malocclusion while it had significant impact on L-nasolabial angle in class Ⅱ and class Ⅲ malocclusion. Further, N1 to NB was a stronger predictor of mentolabial angle than IMPA was in class Ⅱ malocclusion. The multiple regression model for class Ⅲ malocclusion had the strongest explanatory power for Lnasolabial angle while that for class Ⅱ malocclusion had the strongest explanatory power for mentolabial angle.
Ⅳ. Discussion
Because children and adolescents exhibit continuous growth and development, choosing the appropriate time for orthodontic treatment , although very important, is difficult.
Since the introduction of cephalometric radiography to the field of dentistry, it has become possible to evaluate patterns of facial growth and changes in growth with age. This is useful for predicting growth in orthodontics[16,17].
It has been known for a long time that changes in the hard tissue related to growth or orthodontic treatment are associated with soft tissue changes. As the hard tissue is necessarily covered by the distinct anatomical structure of the soft tissue, consisting of skin and muscles, the specific location of the hard tissue itself is not fully visible externally. Thus, in addition to analyzing the relatively static hard tissue, it is important to closely analyze the individual’s soft tissue before initiating the treatment, since this provides the face with its unique character[18]. In particular, changes in the inclination of the incisors affect the protrusion of the profile, and since this is a crucial aspect of orthodontic diagnosis and aesthetic considerations, it is essential to understand the relationship between these two properties. Riedel[19] analyzed cephalometric radiographs in order to study the response of the soft tissue to orthodontic treatment and found that the soft tissue profile was affected by the maxillary and mandibular basal bones, skeletal protrusion, and the relationship of the basal bones with the maxillary and mandibular incisors; additionally, the profiles of the soft and hard tissues are also closely related. However, Burstone[20] reported that these are not always closely connected because of individual differences in the thickness of the soft tissue covering the bones. Likewise, Subtelny et al .[18] reported that not all parts of the soft tissue show consistent changes in response to the growth of the hard tissue that forms its base. In addition, longitudinal studies on soft tissue growth have explained the soft tissue profile in terms of the supporting skeletal structures; they have also shown differences in soft tissue growth between boys and girls. Therefore, for orthodontic diagnosis, it is important to verify the extent of the association between the hard and soft tissues.
Numerous studies have been conducted, with diverse results, for analyzing the soft tissue profile in relation to orthodontic tooth movement because this aspect is critical for establishing orthodontic treatment plans and achieving satisfaction in treatment outcomes. However, according to Rudee et al .[8], orthodontic treatment produces a change in the lip area and an overall improvement in the profile. Therefore, such an outcome should not be taken for granted without first evaluating normal growth-related changes in each part of the soft tissue profile. In this regard, Nanda et al .[15] investigated soft tissue changes by age and sex in male and female participants aged 7 - 18 years with normal class Ⅰ occlusion. They observed that the nasolabial angle showed a slight increase, but the variation by age was large. In contrast, non of the participants did not show significant age-related changes in the mentolabial angle, despite considerable diversity in the size differences between ages. These results may be due to the fact that the nasolabial angle is affected by the protrusion of the alveolar process, the thickness of the lips, and especially the nose, which results in a large variance. Conversely, the mentolabial angle is affected by both the maxillary and the mandibular incisors, and the uncertainty in the landmark could be responsible for the abovementioned result[8,21,22]. In addition, Andersen et al .[21] reported that the nasolabial angle is larger in female than in male children due to differences in nose growth. However, Lo and Hunter[23] reported that the nasolabial angle hardly changed regardless of growth, that changes in the nasolabial angle were unrelated to bodily movement of the maxillary incisors, and that the nasolabial angle increased due to the inclinational movement. Chung et al .[24] reported that male children have a longer nose and overall profile than their female counterparts, while their soft tissue profile has slightly less curvature. With age, both male and female children show greater protrusion and linearity in the lower face, but slightly more curvature in the overall soft tissue profile.
Several studies have also evaluated the association between the soft tissue of the lips and the inclination of the maxillary and mandibular incisors. Wylie et al .[25] reported that the uprighting of the mandibular incisors has little effect on the protrusion of the lower lip, while there is a moderate correlation between uprighting of the maxillary incisors and protrusion of the upper lip. Bloom et al .[10] investigated the correlation between changes in the incisor inclination and the lip inclination before and after orthodontic treatment and found that changes in the inclination of the maxillary incisors affected both the upper and lower lips, while changes in the inclination of the mandibular incisors mainly affected the lower lip. Ramos et al .[26] discovered a significant correlation between posterior movement of the maxillary incisors and changes in the inclination of the upper lip. Rudee et al .[8] also studied changes in the lips in relation to posterior movement of the incisors due to orthodontic treatment. They identified a strong correlation between changes in the inclination of the maxillary incisors and in the upper lip, a moderate correlation between the inclination of the maxillary incisors and the lower lip, and a strong correlation between the inclination of the mandibular incisors and the lower lip. In contrast, Waldman et al .[27] reported that there was no significant correlation between the actual tooth movement and changes in the soft tissue in the horizontal plane. The findings of this study partially support previous reports. With the exception of skeletal class Ⅱ malocclusion, the inclinations of the upper and lower incisors had a significant negative correlation with the inclinations of the upper and lower lips, respectively. The inclinations of the lower incisors and lips were positively correlated only in skeletal class Ⅱ malocclusion.
Initially, in order to predict the response of soft tissues to changes in hard tissues, investigators used the ratio between movements of the soft tissue and corresponding movements of the hard tissue[8,9]. However, Bloom[10] claimed that, since there was a strong correlation between treatment of the hard tissue and changes in the soft tissue, it should be possible to use methods such as regression analysis or scatter plots. Denis and Speidel[28] compared the standard error when using ratios, simple regression analysis, or multiple regression analysis as methods to predict the soft tissue profile in adult patients and reported that ratios were the least accurate, while multiple regression analysis was the most accurate. In this study, multiple regression analysis was used , but in the future, it will be necessary to analyze various other measurements and perform a multiple regression analysis that includes more contributing factors.
This study used the lower-nasolabial angle instead of the nasolabial angle. There have been various reports suggesting that the nose has a major influence on the measurement of the nasolabial angle. For example, Sheideman et al .[29] reported that the nasolabial angle decreases slightly with age due to the downward growth of the nose, and Fitzgerald et al .[30] consistently emphasized the effect of nasal development in the analysis of the nasolabial angle. Therefore, in order to minimize the influence of nasal growth, the lower-nasolabial angle was used, which is measured relative to the FH plane, for comparison with the inclination of the maxillary incisors.
This study has clear limitations as it was a cross-sectional study, and subjects were selected at random, rather than only those with perfect occlusion. Meanwhile, using the FH plane as a reference for maxillary measurements eliminated some possibility of variance due to individual differences. As can be observed in the results, performing a partial correlation analysis that accounted for lip thickness and length yielded a more significant result than the Pearson correlation analysis for the inclinations of the incisors and lips. This shows that the inclination of the lips are affected by various factors, suggesting that an even stronger association between the variables could be obtained by performing a multiple regression analysis that includes factors other than the incisor inclination and the thickness and length of the lips. Other variables that could be added to the regression model include the functional pressure of the soft tissue, patterns of growth, changes in the nose, and growth of the maxilla and mandible.
Ⅴ. Conclusion
This study aimed to investigate the correlation between the inclinations of the incisors and lips in mixed dentition. The findings verify that the inclination of the incisors has an impact on the inclination of the lips irrespective of skeletal malocclusion. Moreover, the impact of incisor inclination is lesser on the lower lip than on the upper lip, with the exception of skeletal class Ⅱ malocclusion, in mixed dentition. Furthermore, we verified that the thickness and length of soft tissue has a more decisive effect on the inclination of the upper lips compared to that on the inclination of the lower lips. These findings suggest that changes of forms near the lips may be predicted to some extent based on the changes in incisor inclination in children with mixed dentition.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






