


Ⅰ. Introduction
Congenital absence of teeth occurs frequently in abnormal tooth development. It is caused by failure of growth and of the differentiation of tooth germ[1]. The incidence of congenital absence of primary dentition was ≤ 0.5% in several studies[2-5]. The incidence of hypodontia ranged from 0.5% among Swedish children to 1.0% among all Caucasians[2]. In a study on tooth agenesis in 193 children with hypodontia of the primary dentition, Dauggard-Jensen et al.[6] confirmed that the congenital absence of primary molars, canines, and maxillary primary central incisors was rare.
Localized early eruption of permanent teeth can occur due to early extraction of deciduous teeth[7]. Early eruption of permanent teeth may also occur due to premature loss of primary teeth, if such loss occurs within 1 year before eruption. However, if the extraction is performed at a very young age, tooth eruption is delayed[8,9].
Ravn[10] showed that primary tooth agenesis was often followed by the agenesis of permanent successors. There is evidence that early loss of primary teeth can affect the eruption of successors, but the precise mechanism underlying the association between congenital absence of primary teeth and eruption of the subsequent permanent teeth is not clear[11,12]. Here, we report 2 rare cases of the early eruption of the permanent canines, combined with congenitally missing primary canines.
Ⅱ. Case Reports
1. Case 1
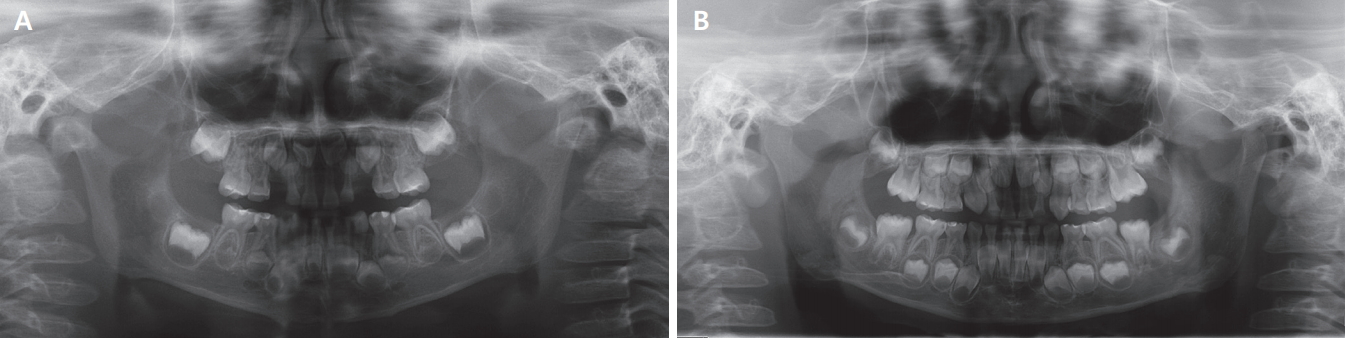
A 3-year-old boy presented to the department of pediatric dentistry, Kyungpook national university dental hospital with a chief complaint of a decayed right mandibular primary canine. He was moderately well nourished and had no history of any systemic disease. There was no family history associated with hypodontia. An intra-oral examination and parental history taking revealed congenital absence of both maxillary primary canines. No treatment was needed for the right mandibular primary canine, due to the absence of cavitation and possibility of remineralization. The initial panoramic radiograph revealed that the right and left maxillary canine tooth germs were located below the lateral incisor tooth germs. In terms of the developmental status of the permanent teeth in the anterior space, crown formation was complete to the cementoenamel junction, and root formation had commenced; spicules were apparent (Fig. 1A). At the 1-year follow-up, at the age of 4 years, the patient exhibited exposure of the right maxillary permanent canine tip, along with near-complete eruption of the left maxillary permanent canine. At his 3-year follow-up, at the age of 6 years, the crowns of both maxillary permanent canines were completely exposed (Fig. 2). The erupted maxillary canines were yellowish rather than bright blue-white in color, and the crown height was larger than the mesiodistal width. Further intra-oral examination and radiographic analysis showed that the central and lateral incisors had not yet erupted (Fig. 1B, 2). Considering the chronological age, all the teeth other than the maxillary permanent canines were at normal stages of growth (Fig. 1B). After eruption of the maxillary permanent canines, clinical examination revealed a right canine cross-bite (Fig. 2). The patient was scheduled for orthodontic diagnosis associated with a right canine cross-bite when he is old enough to cooperate. Also, periodic follow-up was planned to management of overall oral hygiene and check for development and eruption of adjacent permanent teeth.
2. Case 2
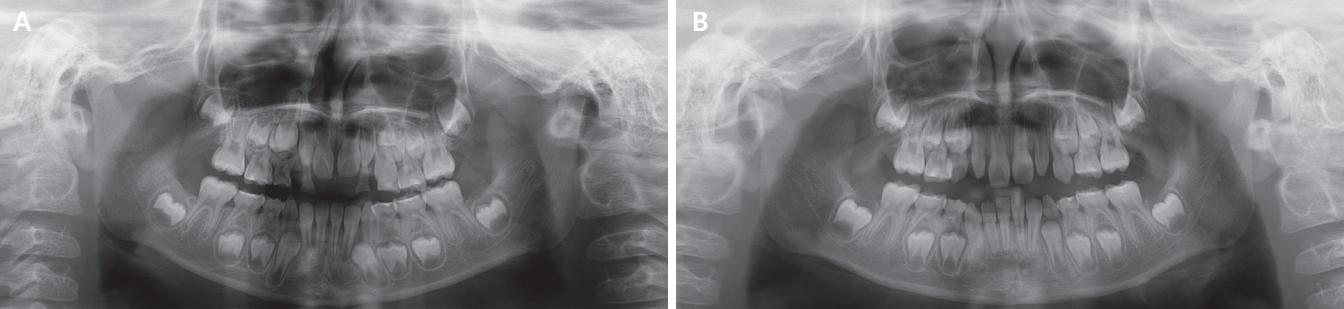
A 6-year-old female was referred from a local dental clinic with a chief complaint of early eruption of permanent teeth, with no medical history of any relevant systemic disease. Based on her parental history, we suspected congenital absence of the maxillary primary canines. There was no family history of congenitally missing maxillary canines. Clinical examination revealed mobility of the left maxillary first primary molar, caused by early eruption of the permanent teeth. Anterior crossbite was seen and maxillary lateral incisors were peg-shaped. Based on the clinical and radiographic findings, we diagnosed congenital absence of both maxillary primary canines and early eruption of the left maxillary permanent canine. The initial panoramic radiograph revealed that the root lengths of both maxillary permanent canines were larger than the crown heights. The root lengths of the maxillary incisors and the lateral incisors were equal to or less than the crown heights (Fig. 3A). We extracted the left maxillary primary molar without local anesthesia, because of mobility and discomfort. When the patient was reviewed 6 months later, the left maxillary permanent canine was fully erupted and a gingival bulge was evident at the right maxillary permanent canine. At the 1-year follow-up, at the age of 7 years, her right permanent canine crown was also fully exposed (Fig. 3B, 4). Intra-oral examination revealed that both maxillary permanent canines were erupted in the first primary molar space. Orthodontic diagnosis was performed due to an anterior cross-bite and an overall lack of space in the maxilla. Orthodontic treatment is scheduled to resolve the anterior cross-bite and space deficiency of the maxilla.
Ⅲ. Discussion
We report 2 cases exhibiting early eruption (at 4 and 6 years of age) of the upper permanent canines, preceded by congenital absence of the upper primary canines. Earlier studies found that normally developing maxillary permanent canines could erupt at any time between 9.3 and 13.1 years of age[13,14]. Therefore, permanent canine eruption was extremely early in our cases.
The average mesiodistal width of the maxillary primary canine is 6.71 mm in boys and 6.59 mm in girls[14]. Using the same measurement methods, the average mesiodistal width of the maxillary permanent canine is 8.11 mm in boys and 7.79 mm in girls[15]. The recommended measurement method was used in our cases. In the 1st case, the distance between the mesiodistal peaks of the contours of the right and left maxillary permanent canines was 7.85 mm and 8.02 mm, respectively. In the 2nd case, the contour height of the early erupted right and left maxillary permanent canines was 7.62 mm and 7.50 mm, respectively. Additionally, these early erupted canines were yellowish and their crown heights were longer than their mesiodistal widths; these are typical features of maxillary permanent canines.
Hypodontia in the primary dentition is often followed by agenesis of the permanent successor[10,16]. However, the current cases showed clinical and radiographic evidence of maxillary permanent canines. There are many studies related to congenital absence(or hypodontia) and maturation of adjacent teeth in the permanent dentition. According to Ruiz-Mealin et al.[17], significant delay in dental age was found in a group with developmental absence of at least 1 primary or permanent tooth. However, another study found no significant difference in the eruption time of teeth in patients with dental agenesis compared to a control group[18]. There are a few studies on the effect of congenitally missing primary teeth on the eruption time of the succeeding permanent teeth. The mechanism of early eruption of the permanent canines in our cases was not clear, so we considered the possible mechanisms based on the features observed in these cases.
Both cases showed congenital absence of the primary canine before early eruption of the maxillary permanent canine. There is controversy about the loss of space when a primary canine is congenitally absent. Shenoy et al.[19] reported a case of impacted maxillary permanent canines due to loss of space after congenital absence of primary canine. However, in a case report by Lee et al.[20], there was no loss of space when the maxillary right primary canine was congenitally missing. Loss of space is an important local factor for maxillary canine impaction. As in our first case, preservation of space may influence early eruption of the maxillary permanent canines.
Many genetic factors and signaling molecules are associated with eruption and tooth development[21,22]. Genes such as PAX9, MSX and WNT10A are known to be associated with tooth agenesis and timing of developmental events[23,24]. Considering that early eruption was limited to the maxillary permanent canines and congenital absence of primary canine, the canine developmental genes may have played a role.
The maxillary canines normally develop at a high location in the maxilla, have a long path of eruption, and erupt into the oral cavity after the neighboring teeth[13]. In our 1st case, the panoramic radiograph taken at 3 years of age showed that the permanent canine tooth germ was positioned lower than normal, below the central incisor tooth germ (Fig. 1A). This low location of tooth germ may be a factor in early eruption of permanent canines.
In our cases, root development of the maxillary canine was particularly rapid compared to that of the adjacent teeth. The permanent teeth remain in certain positions within the alveolar bone until the completion of crown development. After the initiation of root development, the teeth then move rapidly toward the occlusal surface[21]. Thus, it is possible that the early eruptions we report are attributable to early root development.
In our 2nd case, the patient’s lateral incisors were pegshaped. It is well established that morphologic anomalies of the maxillary lateral incisors are closely associated with maxillary canine impaction and displacement[25]. Previous studies showed that the presence of smaller- sized lateral incisor roots is an improtant etiological factor in maxillary canine impaction and displacement[26,27] According to the guidance theory, which suggests that the root of the maxillary lateral incisor plays an important role in inducing normal eruption of the maxillary canine, it is possible to explain that the position of the premature eruption of the maxillary canine was displaced below the first primary molar and the timing of eruption was earlier than normal development[26].
Many reports have described impaction and eruption disorders of the maxillary permanent canines, but early eruption of the maxillary canines is uncommon. Eruption of a permanent mandibular canine in a 5-year-old boy with a congenital absence of the primary canine was reported by Turnbul and Lai[12]. Similar to our 1st case, the space that would have been occupied by the missing mandibular primary canine was not lost and malocclusion was not observed. Madhu[7] also reported early eruption of a maxillary permanent canine in a 7-year-old girl. However, the primary canine was not congenitally missing.
Eruption disorders may change the eruption sequence, create spatial problems, and, when unilateral, result in occlusion asymmetry[28]. In our 1st case, a cross-bite with the mandibular primary canine was apparent, and both maxillary canines erupted before the maxillary central and lateral incisors, resulting in a lack of anterior space. In our 2nd case, the canine erupted below the maxillary primary first molar, triggering the need for later follow-up and treatment in the context of premolar eruption.
In conclusion, early eruption of maxillary permanent canines against a background of congenitally missing maxillary primary canines is rare. Various explanations are possible, but additional studies are required to define the relevant mechanism. Although this condition is uncommon, patients may experience various complications; their dentists must be careful and knowledgeable.
Ⅳ. Summary
In this report, 2 cases of early eruption of the maxillary permanent canines, at ages 4 and 6 years, respectively, were described. Both cases had a history of congenitally missing primary canines. Early eruption of the permanent canine is not common, however, when such eruption occurs, it may change the tooth eruption sequence and create spatial problems. Thus, increased attention should be paid to the possibility of early eruption followed by congenital absence of primary teeth.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






