



Ⅰ. Introduction
In the early 21st century, orthodontics switched from the Angle paradigm to the soft tissue paradigm. The soft tissue paradigm emphasizes the ideal soft tissue proportions, functional occlusion, and soft tissue movements[1]. In this respect, facial anthropometry is important to provide an accurate diagnosis and a treatment plan for individual patients. It is needed for estimating facial growth and evaluating the results of the treatment and efficiency of the surgery in dentistry[2-4].
There are many methods to acquire patients’ facial data ; photography, cone-beam computed tomography (CBCT), and three-dimensional (3D) imaging system[5,6]. The 3D face analysis uses ultrasound, laser scanning, magnetic resonance imaging, contact digitization, stereophotogrammetry and white light system[5-7].
Although photography, the traditional approach, is the easiest way, it is likely to have perspective distortions subject to the angle and distance of view of the image[2]. Despite CBCT can obtain the 3D soft tissue images, CBCT exposes the subjects to radiation. CBCT also cannot retain information on the color and texture of the subjects’ soft tissue[8,9].
The use of 3D imaging systems was recently introduced in the field of medicine to obtain 3D images. It can simulate facial changes following treatments. It can also store integumentary information of the soft tissue. There is no direct contact with the facial surface, avoiding modifications of the soft tissues, which may cause errors in direct measurements[ 6,7,10,11].
In dental field, 3D photogrammetry is commercially available for orthodontic treatments[5,9-13]. The Morpheus 3D® scanner (Morpheus Co., Seoul, Korea) is a 3D photogrammetry device using a structured light system. It uses light emitting diode (LED) light to create 3D images based on data, obtained 3 times for 0.8 seconds[14].
The purpose of this study was to evaluate the accuracy and the precision of 3D images obtained from the 3D imaging system of children’s facial soft tissue by comparing 16 linear measurements. In addition, the study aimed to confirm the children’s error range compared to adults’ error range and determine the reliability of 3D imaging for children.
Ⅱ. Materials and Methods
1. Subjects
The inclusion criteria were 15 children with normal facial growth and development between the ages of 6 to 15 (Table 1).
The purpose of the study was explained to the guardians of all the subjects, following which they signed the consent form. The study was, performed at the Department of Pediatric Dentistry, Kyung Hee University Hospital at Gangdong, Seoul, Korea. It was conformed to approved international review board(IRB) protocols (IRM No : KHNMC 2018-11-009-002).
2. Data capture technique
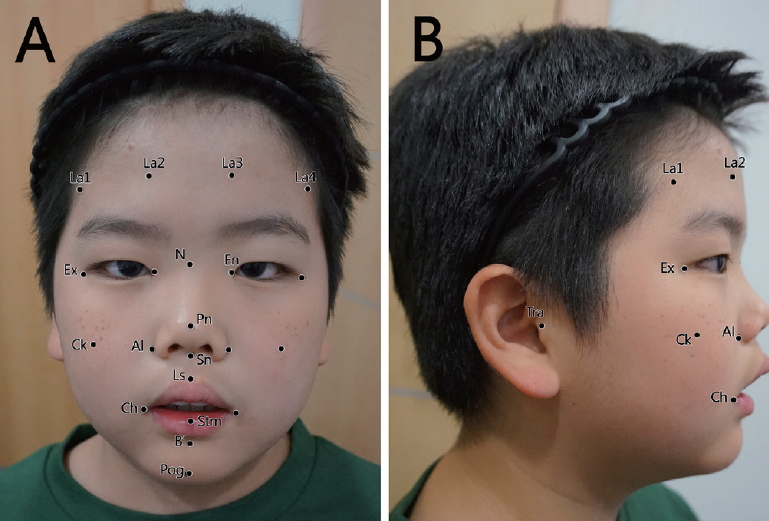
Twenty-three landmarks were pointed on the face of each subject using pencil eyeliner (Fig. 1). The labeled points were followed by the standard anthropometric landmarks defined by Farkas (Table 2). La1 - 4 were defined as the points 4.0 cm above each Exocanthion (Ex) and Endocanthion (En) on the subject’s forehead[2]. Sixteen linear measurements were directly obtained 2 times using an electronic caliper (Fig. 2). The linear distances comprised of 8 horizontal and 8 vertical measurements.
The subject sat on a stool in front of the Morpheus 3D device with molar-bite occlusion, sealed lips and relaxed facial muscles. The facial images of each subject were captured 3 times from 3 different angles (front, left, and right), and merged into a single 3D image using the 3D imaging program. Two sets of 3D images were acquired, and the same 16 linear measurements were acquired from both 3D images. All 3D data acquisitions and measurements were performed by a single operator.
3. Data analysis
Prior to analysis, the data were evaluated using the Shapiro-Wilk test, to determine the normality of distribution. For normally distributed values, the paired t-test was performed. For the other values, the Wilcoxon signed-rank test was performed. All tests were conducted using the SPSS software, version 18.0 (SPSS Inc., Chicago, IL, USA).
Accuracy
The mean values of each measurement from the direct measurement and from the 3D image were compared to determine the accuracy of the scanner.
Precision
For the precision test, 2 sets obtained from direct measurement and 3D image were compared using 3 precision estimates : Mean absolute difference (MAD), relative error magnitude(REM), and technical error of measurement (TEM). The MAD, the mean absolute value of each measurement; it is easy to calculate and is commonly used for estimation of precision. The REM is the value obtained by dividing the MAD by the mean value and multiplying it by 100. The REM compensates for the error in relation to the size of the measurements. The TEM is the standard deviation calculated using the following formula :
Ⅲ. Results
1. Accuracy
When the mean values of each measurement in the direct and 3D images were compared, 7 of the 16 measurements were found to be significantly different. There were no statistically significant differences in the other 9 of the 16 measurements. The mean difference of all the measurements ranged from 0.1 mm to 1.4 mm. The average of all the mean differences was 0.9 mm (Table 3).
2. Precision
The precisions results were compared using MAD, REM and TEM. The MAD ranged from 0.26 mm to 0.96 mm for direct measurements and from 0.41 mm to 1.27 mm for 3D photogrammetry. The mean values of MAD were 0.69 mm for direct measurement and 0.72 mm for 3D photogrammetry. The REM of direct measurements ranged from 0.75% to 6.76% with a mean value of 2.44% and 3D photogrammetry ranged from 0.59% to 4.50% with a mean value of 2.32%. All the TEM was below 1.00 mm except Lt.Tra-Ck in 3D photogrammetry (1.13 mm). The mean value of TEM in direct measurement was 0.62 mm and in 3D photogrammetry was 0.66 mm (Table 4).
Ⅳ. Discussion
Currently, 3D photogrammetry is commercially available and is used in medical fields associated with facial surgeries for facial changes[6,15]. It is more intuitive compared to the other methods, even when there are marked variations in the appearance. For instance, in the dental field, orthodontic treatment can lead to facial changes. Recently, following orthodontic treatments, evaluation of facial changes on the soft-tissue level is performed. Children, like people in general, are concerned about their facial appearance following orthodontic treatments.
In pediatric dentistry, a study was conducted on 3D imaging for children with an orofacial cleft. Babies usually undergo surgeries for cleft repair when they are young. The precise records of facial data before and after the surgery are necessary. It is possible to improve the treatment plan using 3D images owing to the better comprehension of the facial anatomy. Thus, it is useful for the follow-up evaluations of the patient’s facial condition[12].
There are 2 ways to obtain 3D facial images ; laser-scanning system and white light system. In the early stages of 3D photogrammetry, laser scanning technique was used more frequently. However, direct radiations from the laser can harm the patients’ eyes. Therefore, it is being supplemented by white light system. The white light system is divided into stereophotogrammetry and structured light system. In stereophotogrammetry, 2 cameras obtain images from different angles simultaneously and form a 3D image through the triangulation algorithm. In structured light system, the scanner projects points, lines, and patterns formed by light, and calibrates the 3D image using the distortion of the projections. The white light system poses no harm to the human body[5,7,16].
The purpose of this study was to determine the accuracy and precision of the 3D device by comparing 16 linear measurements in children. The 15 children between the ages of 6 to 15 were asked to be participated and 8 boys and 7 girls were included (Table 1). The children in this age often undergo orthodontic treatments that may cause facial morphologic changes[17-19]. The lower age limit was chosen to be 6 years because students begin elementary school at 6 years of age in general. The upper age limit was decided based on the Nolla stage of teeth. The final Nolla stage is the 10th grade, in which children are 15 years of age on average[20].
In the accuracy test, 7 measurements were significantly different(Table 3, p < 0.05), which were En-En, Rt.Tra-Ck, Lt.Tra- Ck, Sn-Ls, Sn-Stm, Stm-Pog, and Stm-B’.
The device error in the merging process of the images and error based on the children’s facial expression might have caused the significant difference. The 3D images using 3 photographs were created through the registration and merging processes. During this process, the overlapping areas of the images were connected. When the landmark was located in this area, small distortion might have occurred[5]. In this study, the increased error in the 3D images could be attributed to the location of the Ck landmarks in this overlapping area.
The 4 measurements that were significantly different were located around the lips ; Sn-Ls, Sn-Stm, Stm-Pog, and Stm-B’. Compared to adults, children are easily distracted. In addition, the muscles around the lips are involved in many facial expressions. It is challenging to keep them sufficiently still to obtain 3 images with the same facial expression, especially in children. We believed that this might have caused the increased error in measurements in the accuracy test.
The same study that was performed in adults revealed that the mean difference in the accuracy of the 3D images was 0.75 mm, compared to the 0.9 mm obtained in this study for children[5]. The MAD, REM, and TEM values of 3D photogrammetry were compared with the same values of direct measurements to evaluate the precision of 3D photogrammetry. The mean MAD values of 3D photogrammetry and direct measurements were 0.72 mm and 0.69 mm, respectively, and the difference was 0.03 mm. Differences in the TEM and REM values were 0.04 mm and 0.12%, respectively. The precision of 3D photogrammetry was almost equivalent to that of the direct measurement. However, the values were higher than the values in the same study on adult[5]. The mean MAD values of 3D photogrammetry and direct measurements in adults were 0.38 mm and 0.31 mm respectively. The values in adults were smaller than that in children.
In this study, 3D photogrammetry in children had sufficient accuracy and precision to be used in clinical settings. The mean difference in accuracy was under 1.0 mm, and the 3D precision level was almost that same as that in direct measurements. However, the accuracy and precision were not as high as in adults. The gap in the mean differences between children and adult was 0.15 mm in the accuracy test. The precision in children was also slightly lower than that in adults, which meant that 3D images of children had lower repeatability. In the clinical environment, errors are more likely in cases of children. More specific instructions are required to obtain accurate 3D images of children. These include instructions on the general posture, facial expression, occlusion, and lip position. In the future, devices or merging programs that yield 3D images in shorter time periods should be developed to reduce the error for children.
Recently, both parents and children are more interested in their appearances. Moreover, many authors claimed that early orthodontic interventions could produce a more significant improvement for skeletal class II or class III malocclusion in children[17,19,21]. In this regard, children before adolescence have more opportunities for orthodontic treatment that can result in facial change. They want more intuitive data that can be simulated prior to the treatment. Therefore, this study could expand the utilization of 3D photogrammetry for children’s facial changes. Based on this study, further studies could be performed for facial changes with growth and evaluation of orthodontic and orthopedic treatment results in children’s soft tissues after providing more detailed instructions.
The limitations of this study were the absence of age categorization for the subjects and the small number of subjects. In future studies, the error range should be verified based on the children’s age category. It should be determined if the younger children tend to have larger mean differences between 3D and direct measurements. Studies with more subjects are also required. Nonetheless, this study verified that the children’s 3D facial images obtained using the 3D imaging system could be put into practice with accuracy and precision after providing detailed instructions.
Ⅴ. Conclusion
The 3D surface-imaging system using the 3D scanner had accuracy and precision of children’s soft tissue. The total average of accuracy was 0.9 mm and the precision of 3D photogrammetry was almost equivalent to that of direct measurements. However, the accuracy and precision in this study were lesser than those observed for adults. Therefore, when the clinicians understand the likelihood of errors in cases of children and provide specific instructions regarding the posture for acquiring exact images, the 3D device could be useful for investigating children’s facial growth and development. Furthermore, the 3D surface-imaging system could be a valuable method for evaluating the results of orthodontic and orthopedic treatments. Future studies are required to verify if there are tendencies for errors based on children’s age category with more subjects. Also 3D devices should be developed in future to reduce for more accurate and precise 3D images of children’s face.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






