



Ⅰ. Introduction
Restorative treatment of large carious lesion has been a challenge for dentists because of pulp sensitivity, microleakage, and secondary caries. Cavity bases can be used to reduce postoperative sensitivity and secondary caries in restoration of extensive carious lesions[1]. The cavity bases are used to provide a barrier or protective layer between the exposed dentin and final restoration[1]. Anusavice[2] defined a base as a layer of insulating, sometimes medicated, cement placed in the deep portion of the cavity preparation to protect the pulp from thermal and chemical injury. Ferracane[3] suggested that bases should be placed in a thick layer and must be strong enough to support a restorative material during its placement and function. Craig and Powers[4] stated that the cavity bases should protect the pulp from heat, mechanically support the restoration, and in many cases, play a role in replacing the dentin that was destroyed by caries or damaged during cavity preparation.
There are many studies on the properties of each base material, but there are only a few studies comparing the various base materials together. The aim of this study was to evaluate and compare the microleakages and compressive strengths of 5 base materials; Fuji II LCTM (FLC), Riva light cureTM (RLC), Pro-RootTM white MTA (WMTA), BiodentineTM (BD), and Well-RootTM PT (WRPT). And it was discussed whether each base material would be acceptable as cavity bases.
Ⅱ. Materials and Methods
The protocol was approved by the Institutional Review Board of Kyungpook National University Dental Hospital (IRB No. KNUDH-2020-03-05-00).
1. Subjects
In this study, 5 types of cavity base materials, FLC, RLC, WMTA, BD, and WRPT, were used, and composite resin(Filtek Z250, 3M ESPETM, USA) was used as a restorative material. Before restoration with the composite resin, ScotchbondTM (3M ESPETM, USA) was used as an etchant and AdperTM Single Bond 2 (3M ESPETM, USA) was used as an adhesive agent. Details of the study materials are described in Table 1.
2. Methods
1) Microleakage
(1) Specimen preparation
A total of 50 permanent premolar teeth with no dental caries and no discoloration were prepared. After removing all soft tissue and debris with an ultrasonic scaler, the teeth were cleansed with pumice and distilled water. After washing, all teeth were immersed in saline, and stored at room temperature. Cavities with a 5.0 mm width, 3.0 mm length, and 3.0 mm depth were formed on the buccal surfaces of the teeth with a #330 carbide bur for high speed engines. The depth of the cavities was confirmed using a thin rod marked with the length and a head length of the bur. The teeth with the cavity were classified into 5 groups according to the type of material used for the cavity bases, and the type of cavity bases was chosen randomly.
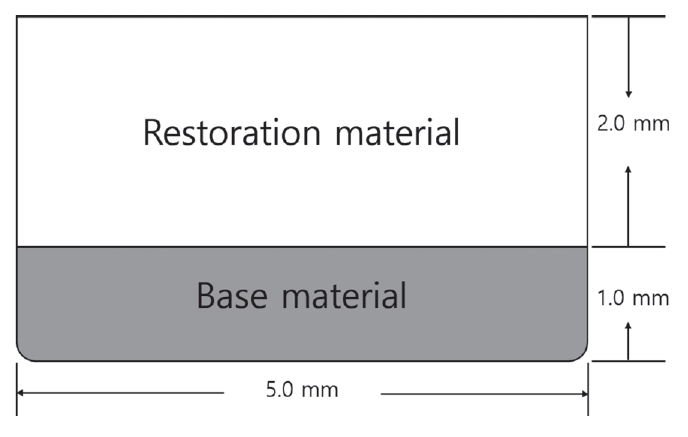
After making with a marking pen at a depth of 1mm of the cavities, the materials were used to fill 10 teeth in each group to a depth of 1.0 mm. The overfilled part was removed before a initial setting of the base materials using a cotton pellet and an explorer. FLC and RLC were mixed according to the manufacturer's instructions and light-cured for 20 seconds at 1200 mW/cm2 using an LED light curing unit (VALO LED, Ultradent, USA). WMTA and BD were mixed according to the manufacturer’s instructions. After filling, WMTA was wrapped with wet gauze and cured at 37°C and 100% humidity for 72 hours. BD was cured at 37°C for 15 minutes. WRPT was cured at 37°C for 30 minutes. The composite resin was then applied to a depth of 2.0 mm on top of the cavity base materials (Fig. 1). After setting of the base materials, all cavities were etched with 35% phosphoric acid for 15 seconds and rinsed for 10 seconds. AdperTM Single Bond 2, a fifth generation adhesive system, was applied and light-curing was carried out with a LED light curing machine (VALO LED, Ultradent, USA) with an intensity of 1200 mW/cm2 for 20 seconds. Then, FiltekTM Z250 was applied for final restoration of the rest of the cavity at a depth of 2.0 mm and light-curing was carried out with the same method for 20 seconds.
(2) Microleakage evaluation
After final restoration, all specimens were placed in deionized water for 24 hours and stored in a thermostat at 37°C. For thermocycling, all specimens were immersed in water baths at 5℃ and 55℃ for 30 seconds and a total of 500 rounds were performed.
To prevent dye penetration through the apical foramen, the apical foramen area was sealed with a composite resin. A nail varnish was applied on the entire surface of the tooth excluding the restoration surface and the surrounding 1.0 mm. For the evaluation of microleakages, all specimens were immersed in 2% methylene blue solution for 24 hours, rinsed, and dried.
To facilitate specimen observation, each tooth was cut into two parts: the crown and root. The crown part was then sectioned buccolingually using a TechCut 4™ Low Speed Saw (Allied, USA) to obtain two specimens for each tooth. The obtained specimens were observed under a stereoscopic microscope (× 30). Dye penetration of each specimen was scored from 0 to 3, and then classified and measured according to the following criteria. Two specimens obtained from one tooth were observed, and the higher score was recorded (Table 2, Fig. 2).
2) Compressive strength
(1) Specimen preparation
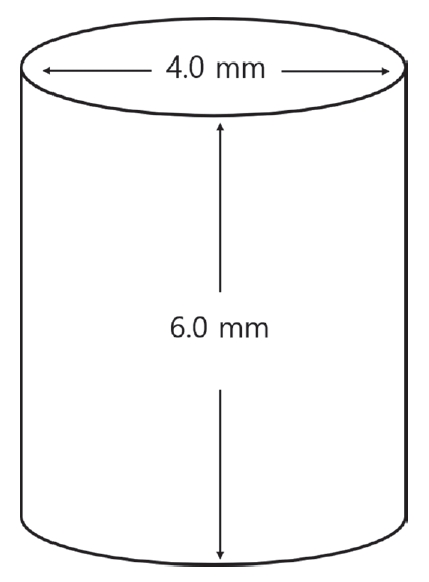
A total of 25 split stainless steel molds capable of producing cylindrical (6.0 mm high × 4.0 mm internal diameter) specimens were prepared. FLC, RLC and WMTA were mixed according to the manufacturer's instructions and were placed in split stainless steel molds at 5 pieces each (Fig. 3). Then, specimens were cured according to the same methods which were used in microleakage evaluation. BD was mixed according to the manufacturer’s instructions, applied to the other 5 split molds, and stored at 37°C for 48 hours. The remaining 5 split stainless steel molds were filled with WRPT and then stored at 37° C for 48 hours. After that, each specimen was separated from the split stainless steel mold.
(2) Compressive strength test
A universal testing machine (Instron 3366, Instron Corp., UK) was used to measure the compressive strength. The specimen was placed in a universal testing machine so that the load could be applied to the long axis of the specimen. The load was applied at a speed of 1.0 mm/min until a fracture occurred, and the maximum load value was applied until the specimen fracture was recorded.
Ⅲ. Results
1. Comparison of microleakages
In this study, after evaluating the degree of microleakages according to the base materials, the highest microleakage was observed in the RLC group and the lowest microleakage in the BD and WRPT groups (Table 3). The results of comparison among the 5 groups regarding microleakages are shown in Table 4.
2. Comparison of compressive strength
1) Mean value for compressive strength
Table 5 shows the compressive strength of the base materials measured in this study. The FLC group showed the highest compressive strength with an average of 189.04 ± 12.79 MPa. The WRPT group showed the lowest compressive strength with an average of 44.55 ± 6.55 MPa.
2) Comparison of compressive strength
The FLC group showed significantly higher compressive strength than all other groups (Table 6).
Ⅳ. Discussion
In the treatment of the large carious lesions, the cavity bases can be used to reduce postoperative sensitivity and secondary caries[1]. There are many characteristics required for the base materials. Sealing ability and compressive strength are one of them. In this study, the microleakages and compressive strength of 5 base materials were evaluated.
The marginal leakage is the precursor of secondary caries, staining of restoration, tooth discoloration, postoperative sensitivity, and pulpal pathology[5]. So, it is important to have a good marginal seal for the longevity of restorative material, thereby reducing the marginal leakage[5]. In this study, microleakages with 5 base materials was evaluated. In previous studies, BD exhibited less microleakage than conventional glass ionomer cement and MTA[6,7]. In this study, BD and WRPT showed the lowest microleakage and RLC showed the highest microleakage (Table 3). And the BD and WRPT groups showed significantly less microleakage than the FLC and RLC groups (p < 0.05). And the WMTA group showed significantly less microleakage than the RLC groups (p < 0.05). The consistency and handling property of the mixed materials might be one of the factors that affect these results.
The handling property is important for the convenience of the procedure in pediatric dentistry. The materials used in this study had different handling properties. FLC showed a high viscosity and good handling property so that it was possible to condense the material with an instrument. RLC showed low viscosity and poor handling property; therefore dense restoration was difficult. WMTA showed a sandy consistency and initial looseness after mixing, revealing a poor handling property[8]. BD can be well-aggregated and it easily adheres to the tooth surface; thus, it has a good handling property and sealing ability[7,9]. WRPT showed a good handling property so that it could be condensed using instruments during the filling process. In this study, BD and WRPT showed the lowest microleakage (Table 3). BD can achieve constant properties through auto-mixing and it has excellent handling property and sealing ability[7,9]. Auto-mixing method is not under the control of the operator, and the mixing regime is standardized by the manufacturer so that the functional properties of the mixed materials are constant[10,11]. WRPT is a pre-mixed type material that shows constant physical properties, and it is provided in the form of a syringe. Therefore, it can be easily applied to the desired area[6]. Moreover, WRPT has excellent handling property. Thus, it can be densely restored to the cavity. It is thought that these factors contributed in part to BD and WRPT showing the lowest microleakage. From the results of microleakage evaluation in the present study, it was confirmed that BD and WRPT were the base materials that have an excellent sealing ability. FLC showed significantly higher microleakage than BD and WRPT in this study (p < 0.05). FLC might show a difference in physical properties each time because it is a power/liquid type material and is mixed by hand. The physical properties of materials that use a traditional hand-mixing method may vary depending on the skill of the operator and mixing environments[11]. Also, because FLC is not available in syringe form, there is high possibility of the presence of voids inside the material during the filling process[12]. RLC is an auto-mixing and syringe-type material. Therefore, it can achieve constant properties and is easy to apply to the cavity. But, it showed the hightest microleakage in this study (Table 3). This result was attributed to the fact that RLC was difficult to condense in the cavity due to its low viscosity and poor handling property. The voids could have been present during the process of adjusting the base material to 1.0 mm height with a cotton pellet. This was supported by Nomoto et al. [10], who stated that a lowviscosity material encouraged more voids to be formed during mechanical mixing. From this result, it could be suggested that the material in the form of auto-mixing does not always show lower porosity and good properties. Therefore, when selecting a material, it is necessary to simultaneously consider other factors, such as the viscosity and handling property of the material and the environment in which the material is being used.
Products applied as a cavity bases require sufficient strength to withstand condensing stresses during filling of the restoration[13]. Compressive strength is one of the main physical properties of base materials. When used as a base material, the cement should have the capacity to withstand masticatory stress[5]. In this study, FLC showed significantly higher compressive strength than the rest of the groups. No statistical significance was observed among the other groups (Table 5, 6). According to the International Organization for Standardization (ISO) 3107, when zinc oxide eugenol is used as cavity bases, the compressive strength should be at least 25 MPa[14]. In ISO 9917-1, the compressive strength of glass ionomer cement, used for a cavity base/lining material, is specified to be at least 50 MPa[15]. In this compressive strength test, FLC had 189.04 ± 12.79 MPa and RLC had 64.14 ± 9.34 MPa, which satisfied the requirements. BD had a compressive strength of 57.04 ± 9.34 MPa, WMTA 53.58 ± 7.10 MPa, and WRPT 44.55 ± 6.55 MPa. Although there are no requirements presented in the international standard for calcium silicate-based materials, the experimental results satisfied the requirements as seen in the standards of ISO 3107 or ISO 9917-1[14,15]. Therefore, all materials in this study can be used as cavity bases. But, if the tooth receives large masticatory stress, such as a permanent molar, a base material with sufficiently high compressive strength would be more recommended[5]. Thus, it can be suggested that if the treated tooth receives large masticatory stress, the material that showed higher compressive strength, such as FLC, is more recommended. In this study, FLC showed the highest compressive strength. The compressive strength of BD in this study was 57.04 ± 9.34 MPa, which was lower than the value reported in previous studies[16]. It is presumed that there was a possibility for the existence of voids inside the specimen due to insufficient operator skills. It was reported that the compressive strength might differ due to the presence of the voids[17]. Grech et al. [18] reported that BD had low fluid uptake, low setting time, and superior mechanical properties. Camilleri et al. [19] reported that BD is more dense and less porous than MTA. According to these results, BD could be also considered as a base material in areas requiring high strength.
Due to the characteristics of pediatric dentistry, it is important to shorten the operation time when treating patients. Therefore, when using the base materials, the materials that have a short setting time and make it possible to complete the whole procedure in a single appointment are recommended. Among the materials used in this study, RMGICs, which can be light-cured immediately, can be used for 1-visit treatment. WMTA has a long setting time, so it cannot be used for 1-visit treatment. BD and WRPT have been promoted as having relatively short setting times, each 12 minutes and 25 minutes, respectively, according to the manufacturers. Although BD and WRPT have relatively short setting times than WMTA, the setting times of these materials are not short enough to be used for a 1-visit treatment.
In the treatment of the teeth affected by extensive caries, cavity bases can be used to reduce postoperative sensitivity and secondary caries. When selecting the base material to be used, many factors, such as the sealing ability, biocompatibility, and physical properties, should be considered. At the same time, in pediatric patients, other factors, such as patient cooperation, the convenience of the procedure and visit times for treatment, should also be considered. In this study, when considering the ease of handling and microleakages of the materials, BD and WRPT showed good results. But, when considering the visit times for treatment and mechanical properties, FLC was more suitable than other materials.
From the findings of this study, it was found that BD and WRPT showed little microleakages and good handling properties as base materials. And it was found that FLC has a short setting time and large compressive strength. But there are many other things that should be considered when selecting a base material. The clinician should know the characteristics of the material and be able to select the appropriate material according to the situation.
This study has some limitations. First, this study would not completely reproduce the oral environment. In this study, WRPT was not cured within 25 minutes, the time indicated by the manufacturer. So, the final restoration was proceeded after 30 minutes. It is thought to be because the environment in which the material is cured is not the same as the clinical conditions. Second, the effect of the final restoration was not considered when evaluating the microleakages. The microleakage on the enamel may be the effect of the final restoration, not the base materials, but this was not considered in this study. Although the composite resin was restored in the form of a single bulk filling to minimize the effect of the final restoration, the effect of the final restoration on the microleakage evaluation was not completely controlled. Third, due to insufficient skills to prepare specimens for the compressive strength evaluation, the experimental results of BD were lower than those of previous studies. Fourth, only the microleakages and compressive strengths of the base materials were evaluated in this study. There are many other factors that should be considered for selecting materials, such as biocompatibility, solubility, and sealing ability. Further studies on other factors that should be considered for selecting materials are needed.
Ⅴ. Conclusion
As a result of comparing and evaluating the microleakages and compressive strengths of 5 base materials. The lowest microleakage was observed in the BD and WRPT groups and the highest compressive strength was observed in the FLC group. Regarding compressive strength, all 5 base materials satisfied the international requirements.
From the findings of this study, it was found that BD and WRPT showed the lowest microleakage and good handling properties as base materials. And it was found that FLC has a short setting time and highest compressive strength. But there are many other things that should be considered when selecting a base material.
All materials used in this study can be used as the cavity bases, but each material has different properties. The clinician should know the characteristics of the material and be able to select the appropriate material according to the situation.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






