



Introduction
Crown restoration is one of the most common treatments for dental caries in primary teeth. Among crowns, stainless steel crowns (SSCs) are widely used be cause they protect the remaining teeth, can be delivered easily, and have economic advantages [1,2]. However, SSCs have the disadvantage of an unaesthetic appearance [3]. Researchers have observed a preference among both parents and children to restore their primary teeth using tooth-colored restorations [4-6].
Compared to other crowns, prefabricated zirconia crowns, which are used for primary tooth restorations with a tooth-colored appearance, are better in terms of biocompatibility, strength and esthetics [7,8]. However, zirconia crowns are thicker than SSCs and may be challenging to adjust, which calls for the need for passive sitting [9]. Prefabricated zirconia crowns have exhibited the utmost durability in clinical investigations; however, these crowns can cause wear on the opposing teeth [10,11]. Previous research has indicated variations in the prevalence of bruxism among children. However, in children with tooth grinding, zirconia restoration may not be effective for the opposing teeth [12].
With the advances in computer-aided design (CAD) technology, it has become easier to design crowns using computers. This can compensate for the limitations of prefabricated zirconia crowns, which are difficult to modify. Additionally, computer-aided manufacturing (CAM) technology has paved the way for three-dimensional (3D) printing methods, which extend beyond milling techniques and have been employed in various dentistry fields, such as prosthetics and surgery [13].
3D-printed resin or milled ceramic crowns are commonly used as interim crowns in dentistry. Ongoing developments are aimed at meeting the safety requirements for use in final prostheses [14,15]. However, the follow-up studies on restorations using such resins and ceramic materials are limited, and they have been rarely used for primary molars.
The degradation of restorative materials through wear is a significant phenomenon in clinical environments. It can pose physical risks through ingestion or inhalation of worn-out materials [16,17], and create esthetic issues [18]. The aim of this study was to assess the quantitative and qualitative wear of 3D-printed resins and milled ceramics for use in fixed primary molar prostheses. The null hypothesis postulated that there were no discernible differences in the extent of wear among the groups.
Materials and Methods
1. Specimen and Metal Die Fabrication
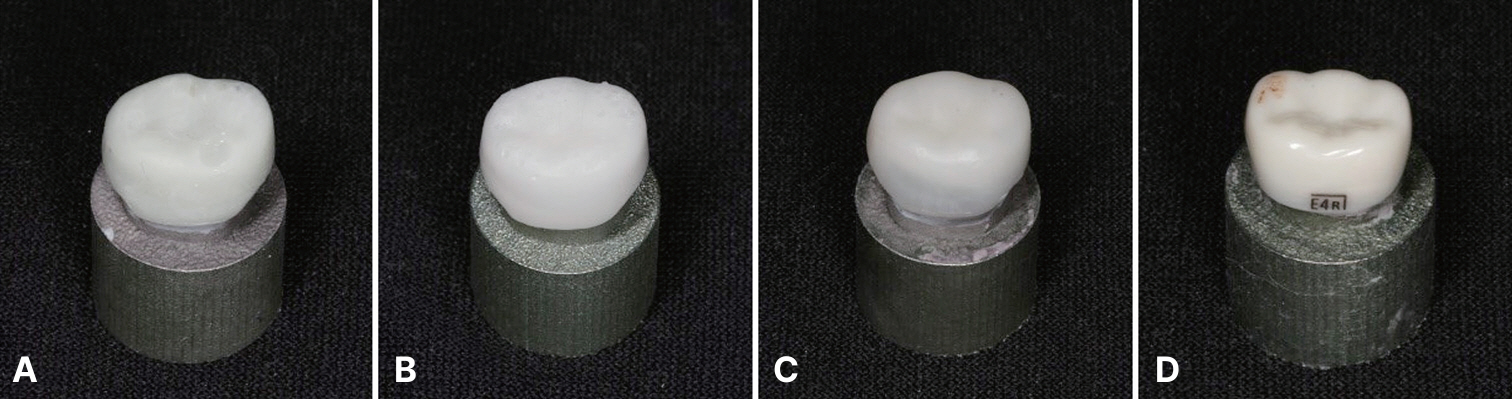
Two types of 3D-printed resin crowns (NXT, NextDent C&B MFH, NextDent B.V., Soesterberg, The Netherlands; GP, Graphy TC-80DP, Graphy Inc., Seoul, Korea), milled nano-hybrid ceramic crowns (MD, MAZIC Duro, Vericom, Chuncheon, Korea), and pre-made zirconia crowns (NS, NuSmile ZR, NuSmile, Houston, TX, USA) were fabricated (n = 12 for each group). The sample size was calculated based on previous research [19]. The inventory of materials used in this study is documented in Table 1.
Polyvinyl siloxane was used as the impression material for die production (Examix NDS; GC Corporation, Tokyo, Japan). The model used for the die was a size “4” NS zirconia crown designed for the mandibular primary second molar. An intraoral scanner (CEREC Omnicam, Sirona, Bensheim, Germany) was utilized to perform the scanning of the impression body, capturing its digital representation, and Co-Cr dies were fabricated through milling operations.
Dental CAD software (Exocad version 3, Gmbh, Darmstadt, Germany) was utilized for designing milled and 3D-printed crowns. All surfaces (lingual, buccal, proximal, and occlusal) were consistently 1 mm thick, and a cement space of 50 μm was specified.
MD crowns were milled using a milling machine (Ceramill Motion2, Amanngirrbach Corp., Charlotte, NC, USA). After the manufacturing process, a wash-out process was performed using ultrasonic cleaning systems (BioSonic UC50D, Waledent, Cuyahoga Falls, OH, USA) for 5 minutes to remove debris. The supported area was refined and shaped using a denture bur (MC079CE; NTI, Kahla, Germany). The polishing process was completed using a gray rubber silicone polisher (H340m; Eve Ernst Vetter GmbH, Keltern, Germany).
NXT and GP crowns were printed using digital light processing (DLP) printers (NextDent 5100, NextDent B.V.; Sprintray Pro95, Graphy Inc.), and the layer thickness was 100 μm. All the printed crowns underwent a post-printing cleaning to remove excess resin monomers using a cleaner for 3D-printed objects (Twin 3D Cleaner, Medifive), and a 3D-printed object washer (Twin Tornado, Medifive, Seoul, Korea). The first and second cleaning steps were carried out for 3 and 2 minutes, respectively. After cleaning, the specimens were allowed to rest for 10 minutes to evaporate any remaining ethanol residue. The crowns were subjected to post-curing using a post-curing machine specific to each manufacturer (LC-3DPrint box, NextDent, 3D systems, Rock Hill, SC, USA; CureM U102H, Graphy Inc.). For NXT, curing took place for 30 minutes at a temperature of 60℃, using UV light with wavelengths in the range of 315 - 550 nm. For GP, curing was performed for 30 minutes on the front and back sides of the specimen at temperatures ranging from 5 - 35℃, using UV light with wavelengths in the range of 390 - 410 nm. For the polishing method, the aforementioned procedure was followed.
2. Cementation of Crowns
The prepared dies were cemented with the crowns in place. The NS crowns used self-adhesive resin cement (RelyX™ U200 Automix, 3M ESPE, St. Paul, MN, USA), and the NXT, GP, and MD crowns were set using resin cement (RelyX™ Ultimate, 3M ESPE). To carry out cementation, a device capable of applying a force of 700 g was used, and the force was applied to the center of each crown for 5 minutes. During the application of force, curing was performed on all the surfaces (lingual, buccal, proximal, and occlusal) for 20 seconds. After cementation, the specimens were immersed in distilled water at a temperature of 37 °C and left to soak for 24 hours. Fig. 1 shows the images of the specimens prepared prior to the chewing simulations.
3. Chewing Simulation
A chewing simulator (CS-4.8, SD; Mechatronik, Feldkirchen-Westerham, Germany) was used, which was capable of simulating various chewing movements in the mouth. Before subjecting the specimens to chewing simulations, scanning was performed using a bluelight dental scanner (T310, Medit, Seoul, Korea). After scanning, the specimen was mounted on the lower part of the chamber, and a 6 mm-diameter steatite ball was installed on top of the chamber.
The simulation settings are listed in Table 2. The frequency was 1.6 Hz with a vertical load of 50 N, and a sliding motion of 0.7 mm for 6.0 × 105 chewing cycles under submerged conditions. The duration of the experimental cycles corresponded to a period of two and a half years of clinical use.
4. Quantitative/Qualitative Analysis of Wear Resistance
All the specimens were steam-cleaned before and after the chewing simulation, and model scan files were obtained using a light scanner. The specimens with observed fractures were excluded from the analysis. The scanned data before and after the chewing simulation were saved in STL format and subsequently imported into 3D inspection software (Geomagic control X, 3D Systems, USA). The amount of wear was measured by comparing the STL files before and after the chewing simulation, and the resulting value from the analysis was the root mean square (RMS) value. Visual representations of the 3D deviations were created through the generation of color maps. The ‘best fit alignment’ was performed to align a specific region of the test object with the corresponding region on the reference object and disregard other regions, thus resulting in superimposition. The maximum and minimum critical values, established at 50 μm (10 μm) and -50 μm (-10 μm), respectively, were used as the thresholds for determining significant deviations in the measurements. The RMS values were calculated using the following equation [20,21]:
where xobs represents the observed values and xmodel represents the modeled values at time i. In each analysis, the value of ‘n’ represents the total count of the measured points. The RMS values were utilized as a metric to quantify the magnitude of deviations between two distinct datasets relative to zero [21].
At the end of the wear test, a qualitative analysis was conducted to assess the observed changes and characteristics. The abraded part of the specimen was collected with a size less than 1. A thin layer of platinum particles, which measured 10 nm in thickness, was applied to the surfaces of the specimens and observed at magnifications of 150 and 1000 using field-emission scanning electron microscopy (FESEM, Hitachi S-4700, Hitachi High-Technologies Group, Schaumburg, IL, USA).
5. Statistical Analysis
The experimental data were subjected to analysis using statistical software (SPSS 25.0, IBM Corp., New York, NY, USA). The normality of the distribution was determined using Shapiro-Wilk test. The data was analyzed using one-way analysis of variance (ANOVA). To compare the volume loss between the groups, post-hoc analysis was performed using Bonferroni correction. The significance level was set at α = 0.05.
Results
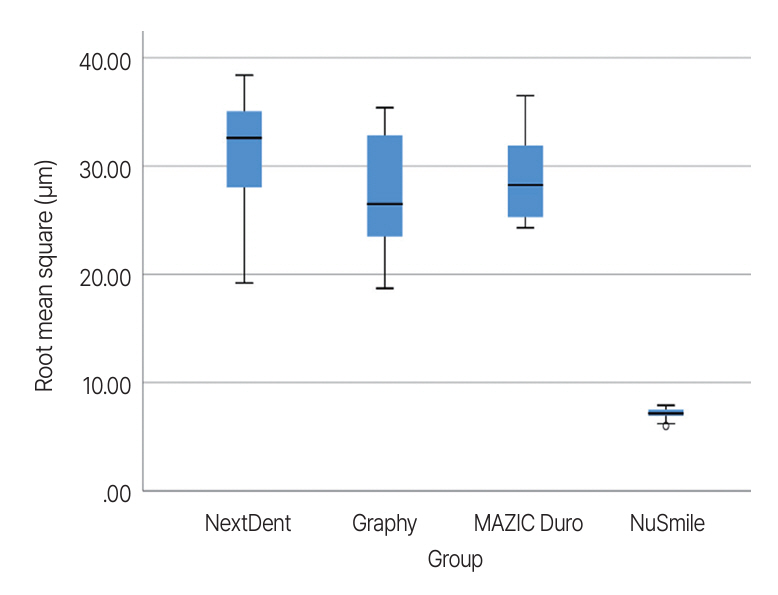
The means and standard deviations of the volume losses of the specimens after chewing simulations are shown in Table 3 and Fig. 2, respectively. The NXT group showed the greatest amount of wear at 31.20 ± 5.60 μm, followed by the MD group with 28.80 ± 4.0 μm, and the GP group with 27.40 ± 5.70 μm. The NS group showed the least amount of wear at 7.10 ± 0.60 μm, which is statistically significant (p < 0.05; Table 4). Except for the NS group, the remaining three groups show no statistically significant difference (p > 0.05; Table 4). In conclusion, the null hypothesis of there were no discernible differences in the extent of wear among the groups was rejected, except in comparisons among the experimental groups.
For three of the 48 specimens, the wear could not be accurately compared due to fracture. One GP specimen split lengthwise and fell apart, whereas two MD specimens fractured in the chipping pattern. The fracture patterns are shown in Fig. 3.
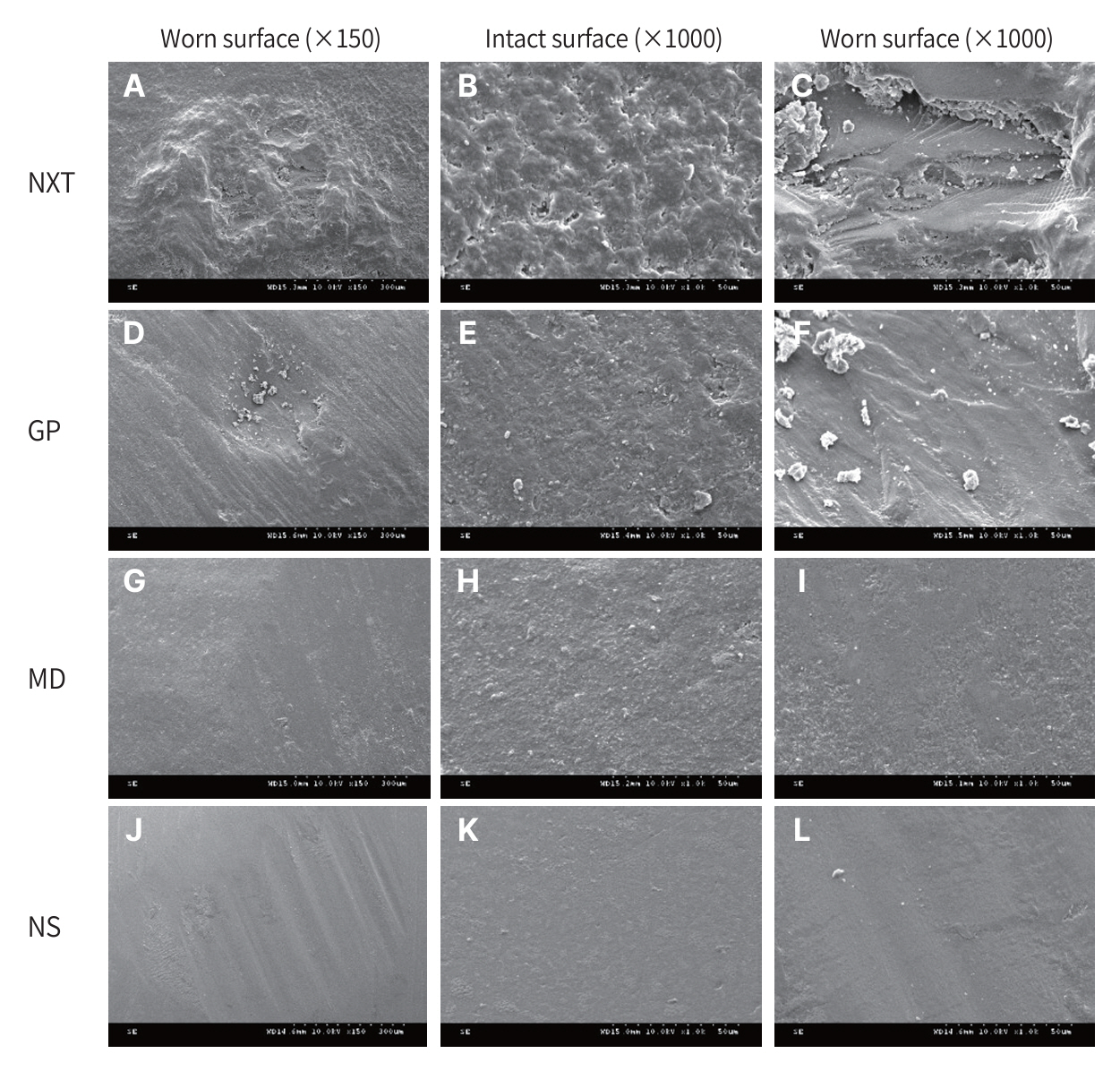
Fig. 4 displays the SEM images depicting the worn surface areas of the tested specimens. On the surface, which was not reached by the antagonist, the GP and NXT groups appear to be rougher than the NS and MD groups. On the abraded surfaces of the specimens, scratches aligned with the sliding direction can be observed. The abraded surfaces of the 3D printed NXT and GP groups exhibit the presence of detached layers. In contrast, only indentations in the sliding direction and compressed features are observed in the NS and MD groups, and no layers were observed.
Discussion
The aim of this study was to assess the wear resistance of tooth-colored materials used in crown restoration for primary molars. The findings of this study reveal notable variations in wear facets among the tested materials, with zirconia crowns exhibiting significantly lower wear volume loss compared to resin and ceramic crowns. These findings may indicate that zirconia crowns are more favorable in terms of durability compared to other crowns for fixed prostheses of primary teeth. Nonetheless, considering the significant amount of wear on the opposing teeth caused by zirconia crowns [22], resinbased crowns can relatively reduce it. In a similar previous study, zirconia crowns exhibited poor marginal integrity and high antagonist wear, while resin crowns demonstrated good performance in terms of wear and marginal quality when compared to SSCs [23].
The differences in material composition among the three experimental groups are evident. NXT has fillers, whereas GP does not. The absence of fillers in GP may make it more susceptible to wear; however, it may have relatively good elasticity due to its network structure. On the other hand, MD can be considered a nanohybrid material with a resin matrix base and ceramic filler. However, despite these compositional differences, the amount of wear did not show statistically significant differences (p > 0.05).
In this study, a chewing simulator was used to determine the amount of wear in the crown specimens of a mandibular secondary primary molar. The clinical evaluation of wear can be a costly and time-consuming process. Additionally, it can be challenging to obtain precise measurements in clinical wear evaluations due to uncontrolled variables, including the variability of environmental factors and chewing forces [24]. Several mastication simulators have been designed to replicate wear processes that occur in the oral environment. These simulators provide notable advantages for conducting in vitro studies [25]. The chewing simulator used in this study is a device that reproduces mastication from occlusal contact to a sliding movement. In this study, the parameters for the wear test, including 6.0 × 105 cycles and 50 N force, were determined based on recommendations from previous studies in the field [26]. A steatite ball with a 6 mm diameter used as an antagonist is a recommended specimen that can replace the enamel in opposing teeth [27].
One GP specimen and two MD specimens were fractured after chewing simulations. The GP specimen fractured with a vertical crack line, whereas the MD specimens fractured in a chipping form. Examination of the SEM image of the GP specimen revealed interlayer bonding, with the accumulation of detachments and cracks potentially leading to the formation of a significant vertical crack [28]. The chipping observed in the MD specimens appears to be a fracture pattern that can arise due to the material characteristics of 76% nanoceramic particles incorporated within the resin matrix, exhibiting a degree of similarity to the brittle characteristics of ceramics [29].
Gingival health is a critical factor to be considered when restoring a crown, with surface roughness, marginal fit, and contour being the three primary factors influencing this aspect [30]. Although an accurate roughness measurement was not performed, the SEM images indicate that 3D printed resin groups exhibit rougher surfaces, particularly in areas subjected to wear, when compared to the milled ceramic and zirconia groups. However, due to the nature of CAD/CAM, adjustments can be readily made to the margin fit and contour of 3D printing and milling groups, thus offering potential advantages over prefabricated zirconia crowns.
This study has several limitations. First, the experiment was conducted in a submerged condition without thermal cycling, which could induce expansion, contraction, and additional aging effects on the materials, while also removing debris from the worn surfaces [28]. However, this does not reflect the oral environment, which includes temperature fluctuations and self-purification mechanisms.
Furthermore, because the exact timing of the fracture during the test could not be verified, it was challenging to determine the precise chewing cycle during which the fractures occurred. In the chewing simulation experiments that do not consider parafunction, it is difficult to determine the prognosis of resin crown restorations in children with bruxism. In the case of newly developed printing resins, it is challenging to achieve optimal roughness owing to the lack of standardization in the polishing process, which may have influenced the degree of wear and cracking.
The surface roughness of a crown can affect the crown fractures [31]. Resin crowns or ceramic crowns that have not undergone optimized surface polishing methods may exhibit lower fracture resistance owing to their rougher surfaces compared to prefabricated zirconia crowns.
Additionally, the difference in crown shapes could potentially influence the research results. Although the inner surface of the NS crown was the same as that of the experimental group, it is challenging to achieve the same thickness for both the experimental and control groups. In the earlier pilot study, resin crowns with thicknesses less than 0.7 mm often experienced fractures, making it difficult to observe the amount and wear characteristics. Additionally, when the thickness was less than 0.4 mm, significant errors occurred during the printing process. As a result, the crown thickness in the experimental group was uniformly set at 1.0 mm, leading to a difference in crown shapes between the experimental and control groups, which could impact the research outcomes.
This study compared resin and zirconia for material comparison purposes, but it is well known that zirconia exhibits excellent wear resistance. Comparing the wear between natural teeth and experimental materials would bring the research closer to real clinical applications.
Conclusion
The currently developed 3D printing resins and milling ceramics used for crown restorations were compared with prefabricated zirconia crowns, and they were found to have lower wear resistance and fracture resistance. Prior to clinical application, research on other physical characteristics such as roughness and discoloration should be conducted as a prerequisite. Even if applied clinically, demonstrating the same level of durability as a zirconia crown would likely be challenging.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






