



Introduction
Successful orthodontic treatment is achieved through accurate diagnosis and treatment planning. Key components within the diagnostic framework include tooth dimensions, arch form, and their corresponding measurements [1]. Model analysis has long been the recognized tool as well as the gold standard in orthodontics, since a patient’s information and treatment planning are derived from it [2].
Traditionally, plaster models have been used in tooth measurements along with digital calipers for model analysis [3]. However, the conventional process of impression taking, necessary for plaster model fabrication, has been associated with discomfort, gag reflex, and/or breathing difficulties, particularly among pediatric patients [4]. Even distraction techniques were employed in managing children during impression-taking to alleviate the gag reflex [5].
On the other hand, a recent trend has emerged towards the use of digital models and intraoral scanning, with reduced invasiveness, decreased discomfort, and increased efficiency [3,6-8]. In comparison to conventional and digital impressions, young patients expressed a preference for intraoral scanning regarding comfort and gagging, even though alginate impressions required shorter chairside time [9,10]. Numerous digital models are equipped with software programs that provide tooth measurements, assisting clinicians in treatment planning. For instance, Invisalign (Align Technology, Santa Clara, CA, USA) features its own ClinCheck Pro software (Align Technology), which offers tooth measurements for all dentitions. Nonetheless, it is imperative to evaluate and verify the accuracy of their estimations for further orthodontic applications.
Various studies have currently indicated that digital models are clinically reliable with diagnostic accuracy [1,11]. They also serve as an uncompromised alternative to traditional plaster casts for routine orthodontic measurements and treatment planning [6]. However, the existing literature has mainly focused on these evaluations within the context of permanent dentition, with limited independent investigations in children with mixed dentition. Obtaining digital models via intraoral scanning could be assumed to be highly necessary, especially in a pediatric dental setting with versatile use. Consequently, this study aims to investigate whether tooth and arch widths acquired using digital calipers on plaster models correspond with digital estimations obtained from digital models.
Therefore, the purpose of the present study is to evaluate the accuracy of predicted tooth widths and arch lengths obtained by two intraoral scanners (iTero Element Plus Series (Align Technology) and Trios 4 (3Shape, Copenhagen, Denmark)) compared to those measured by a digital caliper, assuming they demonstrate similar accuracy within the scope of mixed dentition.
Materials and Methods
Prior to the study, ethical approval was obtained from the Institutional Review Board (IRB) at Kyung Hee University Dental Hospital (IRB number: KH-DT23041). The procedures adhered to the relevant guidelines and regulations.
1. Samples
A total of 30 subjects (14 boys and 16 girls) seeking orthodontic treatment at the Department of Pediatric Dentistry of Kyung Hee University Dental Hospital from January 2021 to May 2023 were recruited. All participants had fully erupted central and lateral incisors as well as permanent first molars, indicating a mixed dentition stage. The sample size was determined for a power of 95%, with an alpha of 0.05 and an effect size of 0.80. The following eligibility criteria were used for exclusion: severe crowding, missing teeth, space maintainers, heavily restored teeth, large carious lesions or enamel defects that would affect the mesiodistal width of a tooth, abnormal tooth shape, and/or abnormal eruption path.
2. Data acquisition
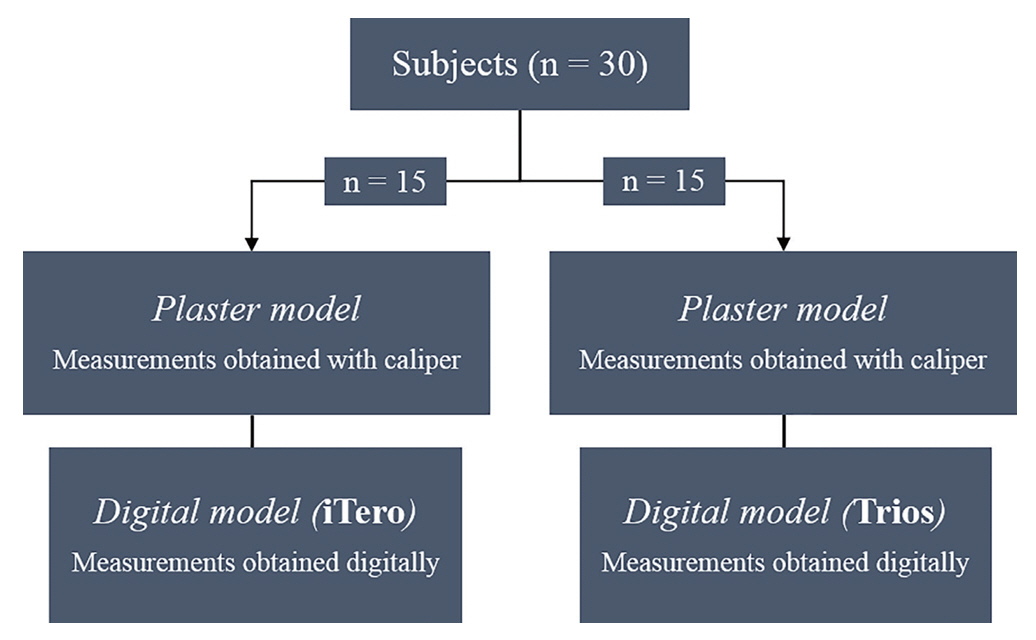
The participants were divided into two groups (Fig. 1). Each underwent both alginate impressions and intraoral scanning. Irreversible hydrocolloid impression material (Aroma Fine Plus, GC, Tokyo, Japan) was used for the maxillary and mandibular arches, which were then used for model fabrication with orthodontic stone (Ortho Stone, Snow Rock, Gimhae, Korea). Additionally, participants underwent intraoral scanning with either the iTero Element Plus Series or Trios 4 scanner. Before the start of the study, one examiner received training in the optimal use of both types of intraoral scanners, and the scans were generated according to the manufacturer’ s guidelines. The process began with the maxillary arch, followed by the mandibular arch, including the recording of maximum intercuspation. Upon completion of the scanning process, the data was saved as either stereolithographic (STL) files or electronically transmitted to ClinCheck Pro software.
3. Data processing and accuracy testing
1) Manual measurements
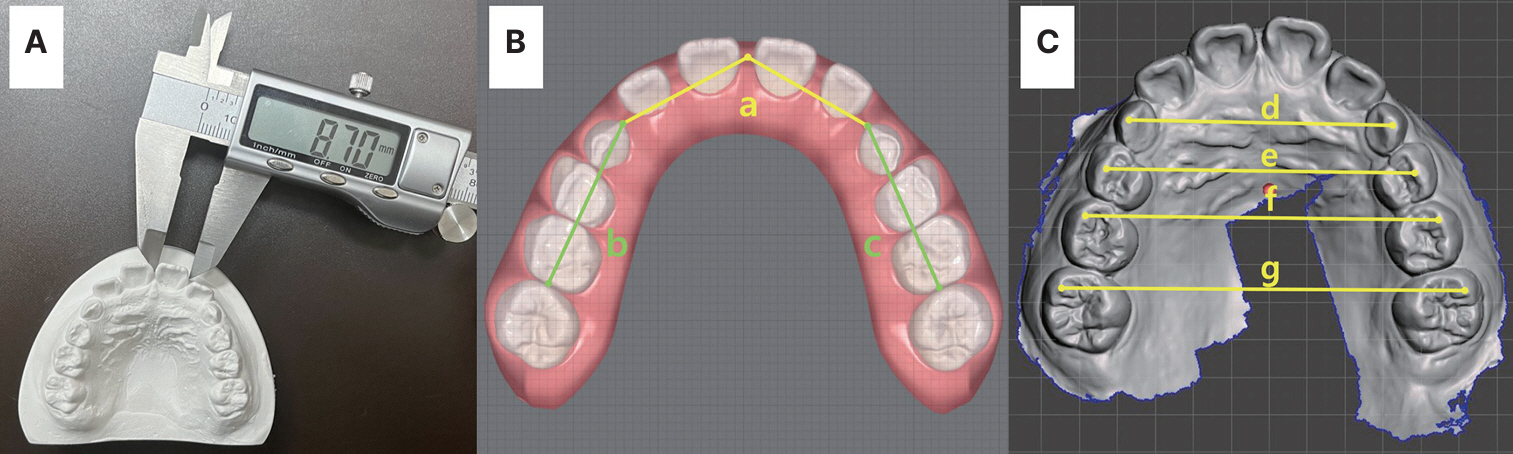
Using a digital caliper, the plaster models were manually measured in both groups (Fig. 2). In a room-light setting, two examiners conducted all the linear measurements of defined distances on each participant’s models while recording the values to the nearest 0.01 mm. Tooth width was defined as the distance between the most protruding mesial contact point and the most protruding distal contact point of the crown [12]. Intercanine width was the linear measurement of the two cusp tips of the right and left primary canines. Likewise, intermolar width was the distance between the two mesiobuccal cusp tips of the right and left primary molars [12]. Arch lengths were measured in 3 different sections; the anterior segment was the sum of the distances between the mesial points of both primary canines to the center of the most protruding mesial points of the central incisors. Right and left arch lengths were measured from the most protruding mesial point of the primary canine to the most protruding mesial point of the first permanent molar on each side. Measurements were taken on two separate occasions with at least one gap week in between. For future analysis, the average of the two recorded values was taken for each measurement (Table 1, 2).
2) Digital measurements
(1) Trios group
The STL files of the Trios group were transferred and opened in Meshmixer software (Autodesk Inc., San Ra-fael, CA, USA) for creating digital models (Fig. 2). Subsequently, using an ImageJ software (National Institutes of Health, Bethesda, MD, USA), virtual measurements were conducted in the same way the plaster study models were measured. The examiner marked two points in the rendered image of the digital model, following the parameter definitions. The distances were automatically calculated to the nearest 0.01 mm (Fig. 2). The digital models were magnified for a sophisticated identification of the anatomical landmarks.
(2) iTero group
As the ClinCheck Pro software had the previously transmitted scan data via iTero, it provided the mesiodistal tooth widths as well as intercanine and intermolar widths to the nearest 0.01 mm. The arch length measurements were not conducted by the ClinCheck Pro, however; hence, ImageJ software was used in an equivalent manner as the Trios group models were virtually measured (Fig. 2).
For both groups, the grid tool was used for setting scale in the ImageJ program. For numerical standardization, all the acquired values were later rounded to the nearest tenth, since some parameters from the ClinCheck Pro offered measurements to the tenths of millimeters.
4. Statistical analysis
Statistical analysis was performed using the SPSS (IBM, Chicago, IL, USA) program and Excel 2013 (Microsoft Co., Redmond, WA, USA). The manual measurements on plaster models were used as a gold standard, and the digital measurement values were compared to them accordingly. Raw data were tested for normality through the Shapiro-Wilk test and did not present a normal distribution. Thus, non-parametric statistics were applied. The Wilcoxon-signed rank test was used for pairwise comparisons.
Results
Intraclass correlation coefficient values ranged between 0.998 and 0.999 for the plaster model in the Trios group and 0.999 and 1.000 for the plaster model in the iTero group, indicating excellent reliability. These values suggested that the reference method of using a caliper showed high consistency.
The means, standard deviations (SD), medians, and p values for comparing measurements of the plaster models to digital models (iTero and Trios groups) are shown in Table 1 and 2.
In the iTero group, there were statistically significant differences in all tooth width measurements between the plaster and iTero values, except for the maxillary left lateral incisors (UL2, p = 0.179), mandibular right central incisors (LR1, p = 0.285), and mandibular left central incisors (LL1, p = 0.073). The values from one group did not consistently exhibit higher or mandibular results compared to the other. However, all tooth width measurements taken by iTero exhibited larger SDs compared to those measured with the caliper (Table 1).
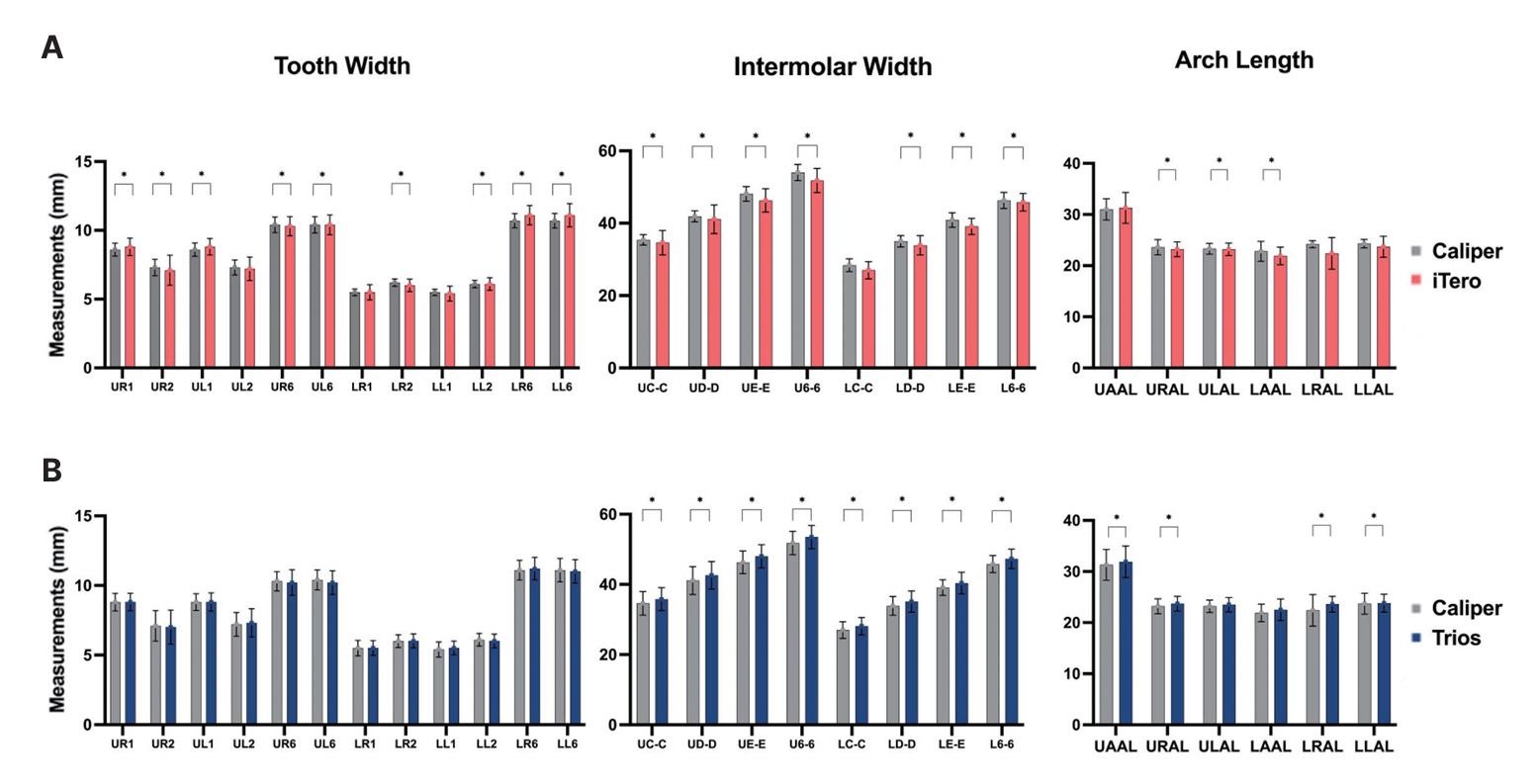
In the Trios group, all tooth width measurements showed disparities between the caliper and Trios values; however, none of these variations were statistically significant. All Trios tooth width measurements showed greater SDs than those measured with the caliper, with the exception of the maxillary right central incisors (UR1), mandibular right central incisors (LR1), mandibular left central incisors (LL1), and mandibular left permanent molars (LL6). The significantly differing measurements with wider SD variances in the caliper and iTero comparisons are noticeable in Fig. 3A. On the contrary, Fig. 3B shows a concordance in tooth width measurements between caliper and Trios values.
Furthermore, all intermolar width comparisons for both the iTero and Trios groups presented differences with statistical significance, except for the distances between the primary mandibular canines (LC-C, p = 0.426) of the iTero group. Wider SDs were evident in all iTero group parameters when compared to those of the caliper. In contrast, distances between the primary maxillary canines (UC-C) and the primary maxillary first molar (UDD) parameters showed smaller SDs in Trios than those of caliper. All other Trios parameters had larger SDs in comparison with those of the caliper.
For the arch length dimension, in the iTero group, the maxillary anterior arch length (UAAL) exhibited a smaller caliper value than that of iTero; however, it was not statistically significant. Conversely, all other variables demonstrated larger caliper values than those of iTero, with maxillary right arch length (URAL), maxillary left arch length (ULAL), and mandibular anterior arch length (LAAL) variables showing significance (p values = 0.013, 0.029, and 0.041, respectively). In the Trios group, all parameters had larger Trios values than those of the cali-per, but only the UAAL, URAL, LRAL, and LLAL parameters had statistical significance (p values = 0.027, 0.007, 0.003, and 0.047, respectively).
Discussion
Plaster models have been a conventional choice for assessing arch length and tooth width measurements in orthodontic diagnosis, representing the established standard for a long period of time. However, taking oral impressions has consistently presented challenges, particularly in pediatric patients. In addition to behavioral management, issues such as discomfort, gag reflex, and even instances of vomiting have been observed during the impression process [13]. In a recent trend, digital models created through intraoral scanning have emerged as a feasible alternative. With the aforementioned challenges either lessened or eliminated, Yilmaz and Aydin [13] reported a strong preference among pediatric patients for digital impressions over conventional methods.
With the consistent demand for orthodontic treatment among young patients, there is a need to assess accuracy not only in permanent dentition but also in mixed dentition. During this stage, when a thorough space analysis is carried out for the impending permanent teeth and phase one orthodontic treatment planning begins, the need for supplementary treatment diminishes. Essentially, treatments for pediatric patients revolve around accurate evaluation of primary teeth, associated spaces, and interarch space, thus emphasizing its significance. Numerous studies have evaluated permanent dentition digital models created with intraoral scans [1,3,6,7,11,14]. Nevertheless, the accuracy of digital scanning and digitally fabricated models for young patients with mixed dentition has received little investigation.
Invisalign is recognized as one of the most widely utilized clear aligner systems [15], while iTero serves as Align Technology’s equipped intraoral scanner. Trios, on the other hand, is acknowledged for its fast scanning capabilities and scanning accuracy [16]. To assess the accuracy of these two scanning systems, the present study utilized a caliper on plaster models as the standard. Moreover, to minimize measurement errors, two examiners conducted measurements twice. The mean of the caliper measurements was eventually used for the comparison.
According to Shailendran et al. [17], ClinCheck Pro systematically underestimated tooth widths with significant differences. Notably, a trend of greater underestimation was observed, particularly in posterior teeth. In contrast, Adobes et al. [18] reported the opposite, with ClinCheck Pro tending to display larger widths. Soto-Alvarez et al. [19] and Rajshekar et al. [20] found substantial agreement with no statistically significant differences between the cast and digital models. The findings of the present study, however, do not entirely align with previous research. Specifically, iTero (ClinCheck Pro) values displayed both higher and lower measurements compared to the caliper values, without a pattern or consistency. Also in the posterior segments, iTero values were found to be overestimated, accompanied by wider SDs, especially in the mandibular molars. On the other hand, Trios estimations exhibited no statistically significant differences compared to those of the caliper, indicating its high accuracy in measuring the mesiodistal distances of a tooth. However, both the iTero and Trios digital models demonstrated larger SD values, likely due to several factors. One notable factor is the inclusion of mild to moderate crowding cases in this study, which may have led to the overlapping points or surfaces, contributing to a broader range of measurement deviation. In addition, the digital models obtained through scanning may have exhibited distortions from the actual dimensions. Accurately replicating the original shape and form, especially in the overlaying interproximal and marginal areas, can be challenging. Thus, standardization by the clinician is imperative for minimizing errors and ensuring highquality digitally scanned data.
Regarding intermolar widths and arch length parameters, Rosseto et al. [21] found no differences in both the intercanine and intermolar widths. Other comparative studies, on the contrary, have indicated significant disparities in mandibular intermolar widths and arch perimeters [6,22-28]. The findings of the present study are consistent with the majority of existing literature, indicating significant statistical differences in all intercanine and intermolar width values between both groups, except for the LC-C in the iTero group. Despite the concentration of existing literature on permanent dentition, the current study focuses on mixed dentition, yielding similar outcomes. This pattern is particularly noticeable in mixed dentition, presumably due to the complexity associated with scanning the small oral cavity, leading to a higher probability of major and minor errors. One reason for the LC-C parameter to show no statistical significance would be attributed to its comparative ease of access during scanning, in contrast to other interarch parameters.
Notably, RAL and LAL in the iTero maxilla and those in the Trios mandible showed statistically significant differences. It is plausible to assume that during intraoral scanning, only the tooth and the adjacent tissues are captured, resulting in the scanner’s automatic calculation. Subsequently, the hard palate and/or the tongue space in between could cause disparity from the actual size. Leifert et al. [25] further suggested that the increased variability and decreased accuracy in the maxillary space can be attributed to the greater difficulty in repeatedly defining the same reference points. Moreover, the more inclined maxillary teeth could bring additional complexity to the process of establishing these points [25].
Despite the factors mentioned above, the majority of authors who identified statistically significant differences between intraoral scanned digital models and plaster models concluded that the differences were not clinically significant [29,30]. Numerous studies support the idea that tooth width differences of less than 0.5 mm are not clinically meaningful, accounting for common errors among clinicians [24,31,32]. Therefore, provided that the mesiodistal dimension of the tooth remains within 0.5 mm difference, digital models could potentially serve as a viable alternative to plaster models with an acceptable degree of accuracy.
However, from the standpoint of pediatric dentistry, even a small amount of space can significantly affect orthodontic treatment procedures for young patients compared to adults. The transitional state of mixed dentition implies an ongoing pattern of continuous growth, wherein the concept of available and required spaces can significantly influence the direction of orthodontic planning for young patients. For crowding problems in the mixed dentition phase, clinicians may leverage leeway space during the transition to permanent dentition [33]. Especially, patients with severe crowding in mixed dentition often benefit from a serial extraction approach. Thus, accurate evaluation and diagnosis play a pivotal role in treatment planning, especially if the measurements fall within the borderline range for assessing the severity of crowding. Cases involving maxillary or mandible expansion, congenitally missing teeth, and abnormalities in tooth shape or size, such as peg lateralis, heavily rely on accurate measurements, especially for growing patients. While numerous authors have discussed the clinical significance of accuracy, pediatric dentists should assess issues concerning tooth dimensions more closely.
The current study has limitations that should be mentioned. A larger sample size with various intraoral scanners may provide a more precise resolution to the research inquiry. Furthermore, as this study solely included dentition with mild to moderate crowding, the findings were limited to this context and did not account for differences in cases of severe crowding, severe curve of spee, or abnormal tooth shapes. Grünheid et al. [34] explained the “shape assumption” method of intraoral scanners, whereby these pertinent software systems use proprietary algorithms to automatically fill in any uncaptured, indistinct, or missing data, thus introducing the possibility of inaccuracies. Therefore, undertaking broader studies encompassing a range of malocclusion cases and a more extensive sample size would yield deeper insights and enhanced scrutiny, not only concerning accuracy but also with regards to pediatric orthodontic planning.
Conclusion
While digital models could serve as viable alternatives to plaster models due to their clinical insignificance, it is important for pediatric dentists to remain attentive to minor deviations in digital model measurements and analysis. A comprehensive assessment of these variations is crucial to ensuring accurate orthodontic treatment planning and, consequently, successful orthodontic results for young patients in mixed dentition.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






