



Introduction
The first clinical sign of dental caries is a white spot lesion on the tooth surface caused by demineralization of enamel [1,2]. Initial carious lesions undergo dynamic stages of repeated demineralization and remineralization; however, if demineralization continues, it can progress to cavitation. Therefore, achieving effective remineralization before the initial carious lesion progresses can serve as a non-invasive method to maintain healthy dentition [2-4].
Among the various methods, the use of fluoride has proven to be highly effective in managing initial carious lesions [5-7]. Silver diamine fluoride (SDF) is an alkaline liquid containing fluoride and silver, with ammonia used for solution stability. The disadvantages of SDF include black staining of the tooth surface after application, unpleasant odor of the solution, and gingival irritation. To address the staining issue, a method has been proposed where potassium iodide (KI) is applied immediately after SDF application, which has been found to reduce staining on the enamel [8]. The unpleasant odor and gingival irritation of SDF are caused by the ammonia component, which can lead to additional steps and time for gingival isolation, causing discomfort to the patient. To overcome these problems, water-based silver fluoride (AgF), which does not contain ammonia and has a neutral pH, was recently developed. Although the remineralization effect of SDF has been demonstrated in previous studies [9,10], research on the initial carious lesion remineralization effect of water-based AgF is currently limited.
Among the methods used to evaluate the degree of lesion remineralization, microhardness measurements provide indirect evidence of mineral loss or deposition. If mineral loss occurs in the tissue, the size of the indentation increases. Microhardness measurement is relatively simple and fast, and it has been widely used to evaluate the degree of demineralization and remineralization in enamel [11]. Quantitative light-induced fluorescence (QLF) is a useful method for non-invasively evaluating the degree of remineralization by measuring the difference in fluorescence between sound and demineralized enamel. QLF has the advantage of being able to quantify the progress of early caries because it displays the difference in fluorescence and its area in numerical values. QLF has shown high accuracy and reliability as a diagnostic tool for early stage enamel demineralization in caries progression [12].
This study aimed to evaluate the effect of water-based AgF on remineralizing early enamel lesions by comparing it with other fluoride agents through microhardness and QLF measurements.
Materials and Methods
1. Specimen preparation
Eighty healthy bovine incisors without caries or defects were used. The periodontal ligaments and other contaminants on the surface were removed using a scaler, following which the teeth were soaked in distilled water, refrigerated at 4.0°C until the study, and used within 1 month of extraction. The root was removed at the cemento-enamel junction using a water-cooled model trimmer. The crown was cut to a size of 3.0 mm × 3.0 mm for microhardness specimens and 5.0 mm x 5.0 mm for QLF specimens and embedded in acrylic resin, exposing the labial surface. The specimens were polished using a specimen grinder (RB 209 MINIPOL, R&B Inc., Daejeon, Korea) with 320, 600, 1500, and 2000 grit silicon carbide abrasive papers to achieve a flat and uniformly ground enamel surface. For the QLF specimens, acidresistant nail varnish was applied twice to all surfaces, except for the 3.0 mm × 3.0 mm square enamel surface in the center.
2. Preparation of the artificial carious lesions
To induce artificial carious lesions in enamel, an acetic acid demineralization solution of pH 4.4 was prepared using 2.2 mM CaCl2, 2.2 mM KH2PO4, and 50 mM acetate. The specimens were stored in the demineralizing solution for 4 days at room temperature [13].
3. Classification of specimens and application of remineralization agents
Forty specimens each for microhardness and QLF testing were randomly classified into 4 groups of 10 each; the remineralization agents used are shown in Table 1. Group I was treated with AgF, where AgF 1.0 μL was uniformly applied to the specimens using a fine-sized microbrush for 10 seconds, followed by the uniform application of KI 2.0 μL for 10 seconds. After 3 minutes, the specimens were rinsed with distilled water. Group II was treated with SDF, where 1.0 μL of SDF and 2.0 μL of KI were applied to the specimens and rinsed in the same manner as Group I. The quantity of SDF was determined based on recommended clinical guidelines by adjusting the size of the specimen [14], and the amount of AgF was set to the same amount as SDF by referring to the manufacturer’s instructions [15,16]. Group III was treated with Sodium fluoride (NaF) varnish, which was applied for 10 seconds and dried for 30 minutes. Subsequently, the specimens were stored in distilled water for 4 hours and NaF varnish was removed using a toothbrush under running water. Group IV served as the control group and was rinsed with distilled water without any additional treatment.
4. pH cycling
To evaluate the effect of each agent used in the study on the remineralization of artificial enamel caries, pH cycling was conducted as previously described [13]. A remineralization solution with a pH of 7.0 was prepared using 20 mM HEPES, 1.5 mM CaCl2, 0.9 mM KH2PO4, and 150 mM KCl. A demineralization solution with a pH of 5.0 was prepared using 1.5 mM CaCl2, 0.9 mM KH2PO4, and 50 mM acetate. The pH of the remineralization and demineralization solutions was adjusted using potassium hydroxide (KOH). Specimens from each group were soaked in the demineralization solution for 3 hours and remineralization solution for 21 hours at room temperature, which was repeated for 8 days. A 30-second rinse with distilled water facilitated the transition between solutions, and each solution was replaced with a new solution every day.
5. Microhardness measurements
The Vickers microhardness (HMV) of enamel specimens was measured at 3 time points: before artificial caries preparation (baseline), after artificial caries preparation (lesion), and after remineralization agent application and pH cycling (post-treatment). The measurements were conducted using a Vickers microhardness tester (MMT-X7, Matsuzawa, Akita, Japan) by selecting 3 measurement points sufficiently far apart for each specimen under a load of 50 gf for 10 seconds. The average value of these measurements was calculated and used as the representative value for each specimen. The difference (ΔHMV) between microhardness values at the lesion and post-treatment time points was calculated.
6. QLF analysis
White light and fluorescent images were taken consecutively using a Qraypen C (AIOBIO, Seoul, Korea), a portable QLF diagnostic device, at 3 time points: before artificial caries preparation (baseline), after artificial caries preparation (lesion), and after remineralization agent application and pH cycling (post-treatment). To standardize the imaging process, the specimens were placed in a black box with an entrance on only one side, and images were taken from a 90-degree upward angle (Fig. 1). When capturing images at the lesion time point, all nail varnishes on the specimens were removed using acetone before image capturing. Before applying remineralizing agents and pH cycling, nail varnish was reapplied twice to all surfaces, except for the same 3.0 mm × 3.0 mm square area. Post-treatment images were obtained after removing the nail varnish using acetone. Images were analyzed using the QLF analysis program (QA2 software v.1.39, Inspektor Research Systems BV, Amsterdam, Netherlands). The ΔF average (%), which is the percentage of fluorescence lost in the lesion area compared to the fluorescence of normal enamel, was obtained in the analysis program. The difference in ΔF values between the lesion and post-treatment time points (ΔFpost-lesion) was calculated.
7. Statistical analysis
Statistical analyses were conducted using SPSS (version 29.0; IBM, Armonk, NY, USA). The normality of the microhardness and QLF values was assessed using the Shapiro-Wilk test. The microhardness and QLF values of all groups at all time points satisfied normality. One-way ANOVA was used to determine the differences in microhardness and QLF values among the 4 groups at baseline and lesion time points. Paired t-tests were used to assess the significant differences in the microhardness and QLF values before (lesion) and after (post-treatment) treatment for each group. One-way ANOVA was conducted to compare ΔHMV and ΔFpost-lesion between the 4 groups, followed by Tukey’s honestly significant difference test for post hoc analysis. The significance level for all statistical analyses was set at p < 0.05.
Results
1. Microhardness
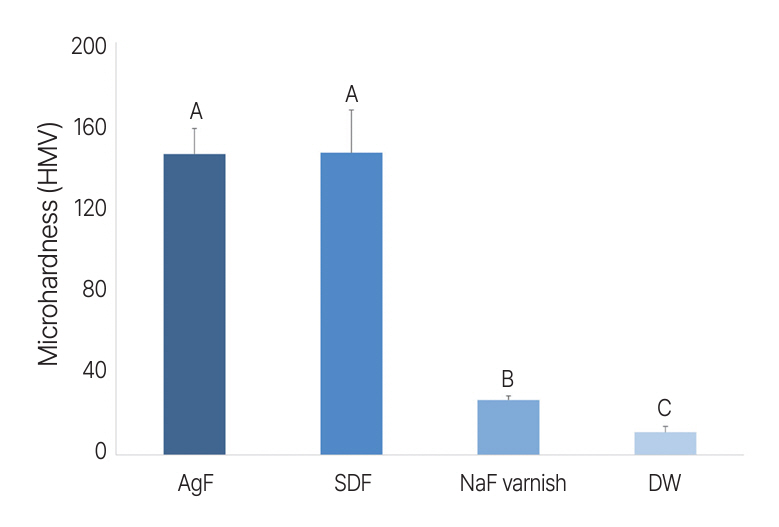
At the baseline and lesion time points, no significant differences were observed in the microhardness values between the 4 groups (Table 2). When comparing the microhardness measured at the post-treatment point with that at the lesion point, a statistically significant increase in microhardness was observed in all groups (p < 0.0001). When comparing the increases in microhardness values between the lesion and post-treatment time points (Δ HMV) among the 4 groups (Table 2, Fig. 2), the AgF and SDF groups showed the greatest increase in microhardness, with no significant difference between these 2 groups. The NaF varnish group exhibited a significantly greater increase in microhardness than the control group (p = 0.049) but showed a significantly smaller increase than the AgF and SDF groups (p < 0.0001).
2. QLF
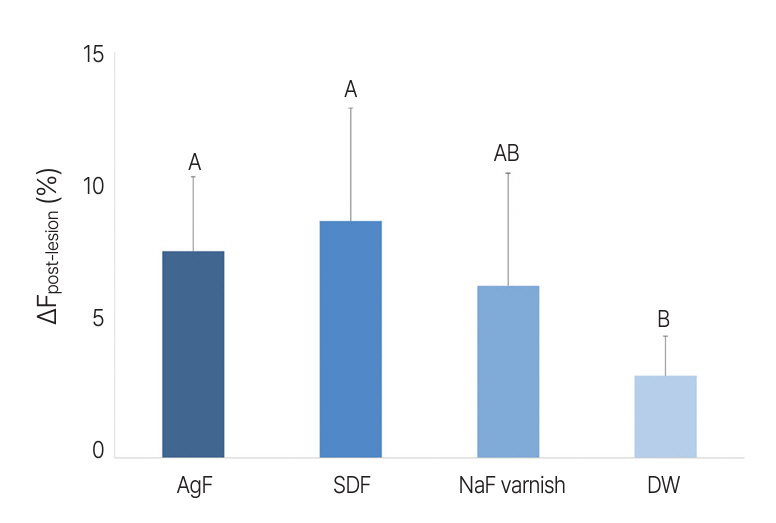
At baseline, the ΔF value of all specimens was 0, indicating a sound enamel surface. No significant difference was observed in the ΔF values at the lesion point between the 4 groups (Table 3). When comparing the Δ F measured at the post-treatment point with that at the lesion point, a statistically significant increase in ΔF was observed in all groups (p < 0.0001). When comparing the increases in ΔF values between the lesion and post-treatment time points (ΔFpost-lesion) among the 4 groups (Table 3, Fig. 3), the AgF and SDF groups showed a statistically significant increase in ΔF compared to the control group (AgF: p = 0.029, SDF: p = 0.005), with no significant difference between these 2 groups. The NaF varnish group showed a larger increase than the control group and a smaller increase than the AgF and SDF groups; however, the differences were not statistically significant.
Discussion
The remineralization effect of SDF on early carious lesions has been demonstrated in previous studies [17-19]. Although SDF has this advantage, it also has some disadvantages, including unpleasant taste, odor, and soft tissue irritation due to its ammonia content. Ammonia in SDF plays a role in increasing the pH and stabilizing the solution. To overcome these shortcomings of SDF, a water-based AgF solution without ammonia was developed. It does not have the unpleasant taste and odor associated with ammonia, which is beneficial to patients. While the pH of SDF is 11, the pH of water-based AgF is 7.4, which is closer to the physiological range [20]. Therefore, it is biocompatible for use in the oral environment. The application procedures and clinical guidelines for SDF and water-based AgF are the same, except that SDF requires a more thorough gingival barrier.
However, the action of SDF in stopping the progression of carious lesions may be attributed not only to the high fluoride concentration and silver components but also to its alkaline nature. This alkaline property is favorable for remineralization and may inactivate collagen degradation enzymes [21]. Therefore, it can be questioned whether neutral-pH AgF is as effective as SDF in remineralizing early carious lesions. The results of this study showed that the SDF group and AgF group exhibited similar increases in microhardness and ΔF with no statistically significant differences.
The SDF used in this study contained 39,004 ppm fluoride [22], and the AgF contained 42,429 ppm fluoride [23]. Fluoride reacts with calcium ions on the tooth surface and exists in the form of calcium fluoride, which then dissolves to form fluorapatite, thereby acting on remineralization [17]. The number of calcium ions on the tooth surface may have been limited by the laboratory environment used in this study. If the fluoride concentrations of SDF and AgF were sufficiently high to exceed the capacity of calcium ions, resulting in the generation of calcium fluoride without a significant difference, the remineralization effect would remain consistent, regardless of the pH of the solution. Additionally, the alkaline property of SDF, which inactivates collagen degradation enzymes and stops the progression of caries, may be more significant in dentin containing 18% collagen than in enamel containing more than 95 wt% mineral [24,25]. Therefore, in early enamel lesions, the pH difference between AgF and SDF may not have had a significant effect on remineralization.
In this study, the AgF and SDF groups showed a significantly greater increase in microhardness than the NaF varnish group. In QLF testing, the AgF and SDF groups showed a greater increase in ΔF than the NaF varnish group, although no statistical significance was observed. According to previous studies, a higher fluoride concentration leads to a greater remineralization effect in early enamel caries [26,27]. The NaF varnish used in this study contained a lower fluoride concentration of 22,600 ppm than AgF and SDF [28], which may have resulted in a smaller remineralization effect. In addition, NaF varnish is viscous, whereas AgF and SDF solutions are flowable. This may have led to an increased amount of fluoride being absorbed into the demineralized enamel in the AgF and SDF groups. The liquidity of AgF and SDF allowed for full contact of AgF and SDF with the enamel surface, and fluoride ions could have penetrated the enamel relatively quickly. In contrast, the viscosity of the NaF varnish may have slowed the penetration of fluoride ions into the enamel. To simulate the actual clinical conditions, the varnish was applied, dried for 30 minutes, stored in distilled water for 4 hours, and then removed. This process may have limited the time for which the NaF varnish was in contact with the tooth surface, resulting in a low remineralization effect [17].
The control group, Group IV, exhibited a statistically significant increase in microhardness and ΔF. This result can be attributed to the pH cycling, which was intended to simulate remineralization in the oral cavity.
The limitations of this study include that the progression of carious lesions was assumed to be related only to pH changes in the oral cavity, which differs from the actual oral environment. Moreover, the study used a chemical system and lacked biological components; therefore, the antimicrobial effect of silver in remineralization was not included. Future in vivo studies evaluating the remineralization effect of water-based AgF in clinical environments and their antimicrobial activity against various cariogenic microorganisms are needed. The pH cycling period for this study was 8 days. Studies setting several pH cycling periods, including longer periods, are also needed to compare the differences in remineralization effects between different fluoride agents over time.
Conclusion
Within the limitations of this study, water-based AgF and SDF demonstrated the greatest remineralization effect on enamel lesions with no statistically significant differences between the two. Owing to the ammonia base, SDF is alkaline and may cause mild soft tissue irritation and unpleasant taste and odor to the patients. Waterbased AgF has a significantly lower pH than SDF, making it more biocompatible for use in the oral environment. Water-based AgF is clinically valuable for remineralizing enamel lesions, with the advantages of no risk of tissue burn and improved taste and smell.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






