Clinical Usefulness of the Jones Jig Appliance for Alignment of Premolars and Molars: Case Reports
Article information

Trans Abstract
Early loss of the primary maxillary second molar can lead to complications in which mesial drift of the adjacent first molar (M1) can disturb eruption of the succedaneous second premolar (P2). This study reports two cases of space loss for P2 caused by early exfoliation of its predecessor. After the eruption of the first premolar, the Jones jig appliance was used to distalize M1 and regain space for the eruption of P2. The appliance was further utilized to align the palatally erupted P2 into the dental arch. In both cases, the space and corrected position of P2 were well maintained. Early exfoliation of the primary second molar caused by mesial encroachment of M1 is a common phenomenon, and pediatric dentists should attend to this during routine examinations. An appropriate intervention should be initiated when the primary second molar is lost during the mixed dentition period. If used with careful anchorage control, the Jones jig appliance can effectively resolve this problem.
Introduction
Distalization of maxillary molars is often required in the non-extraction treatment of Angle Class II malocclusion with minimal to moderate crowding. This can be achieved with both orthodontic and orthopedic actions by exerting extraoral forces from headgear. However, treatment using headgear largely depends on patient cooperation and can require a long period of time due to the use of intermittent forces [1]. Accordingly, various intraoral appliances for maxillary molar distalization have been developed to avoid the need for patient cooperation. In 1978, Blechman and Smiley [2] introduced repelling magnets; in 1991, Gianelly et al. [3] used superelastic nitinol coil springs on continuous arch wires; and in 1992, Hilgers [4] developed the pendulum appliance while Jones and White devised the Jones jig appliance [5]. In 1995, Karla [6] created the K-loop; and in 1996, Carano and Testa [7] invented the distal jet appliance.
The Jones jig appliance is a combination of a sectional jig assembly and a modified Nance holding arch (NHA). The NHA serves as anchor that usually connects the premolar on the molar distalization side to the contralateral premolar or molar. The sectional jig assembly, which is the active part of the appliance, consists of a 0.030-inch stainless steel wire with a sliding nitinol coil spring and eyelet tube. The distal part of the sectional wire is inserted into a double-slotted tube on the molar to be distalized. The nitinol coil spring is guided over the wire mesial to the molar and compressed by the eyelet tube, which is guided over the wire mesial to the coil spring. The eyelet tube is tightly ligated with a stainless-steel wire to a bracket welded onto the buccal side of the premolar band (Fig. 1). The jig assembly is activated every 4 weeks by compressing the coil spring from 1.0 - 5.0 mm on each activation [5]. The maxillary molar is distalized at a rate of approximately 0.83 mm/month [8], and the jig assembly is activated until Class I molar relationship is established.
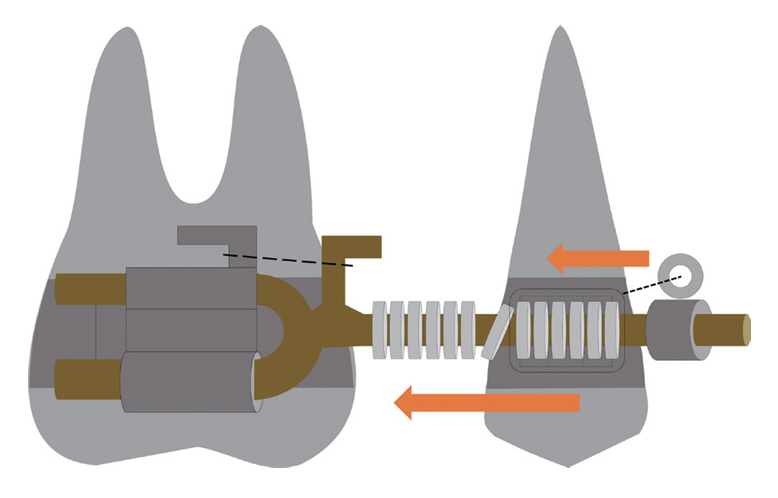
Schematic diagram of the Jones jig appliance. The distal end of the sectional jig assembly is inserted into a double-slotted tube welded onto the band of the maxillary molar. An elastic modulus (as marked by a thick dotted line) can be used to prevent displacement of the sectional jig assembly. Then, a nitinol coil spring is compressed by sliding an eyelet tube distally and tying it to the bracket welded onto the band of the maxillary premolar with a stainless-steel ligature wire (as marked by a thin dotted line).
Premature loss of the primary maxillary second molar causes significant mesial movement and tilting of the adjacent first molar [9]. Space loss occurs fastest and in the greatest amount when the primary second molar is extracted before the eruption of the first molar. If left untreated, eruption disturbances of the second premolar can occur, leading to further development of malocclusion. Thus, space problems due to early loss of the primary second molar must be resolved in a timely manner. The Jones jig appliance can be used to regain space lost by mesial encroachment of the maxillary first molar. This report describes two cases utilizing the Jones jig appliance to distalize the maxillary first molar into its original position.
Case Reports
The publication of these case reports and any supplemental photographs was approved with the written consent of the patients’ legal guardians.
Case 1
A 5-year-old boy visited Seoul National University Dental Hospital for dental caries. His initial panoramic radiograph showed distal root resorption of both primary maxillary second molars due to mesial encroachment of the adjacent first molars (Fig. 2). After one year, both first molars erupted into their normal positions. While the left primary second molar remained stable, the right primary second molar showed increased mobility due to progressive root resorption (Fig. 3). Extraction of the right primary second molar and space maintenance with an NHA were performed.

Panoramic radiograph of the patient at age 5 on the first visit. Both primary maxillary second molars showed root resorption due to mesial encroachment of their adjacent first molars.
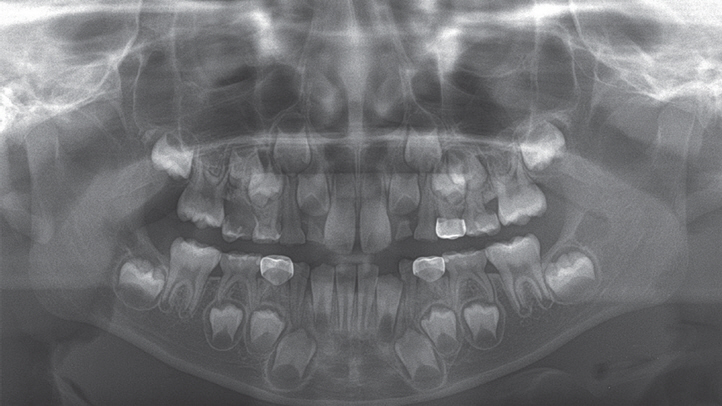
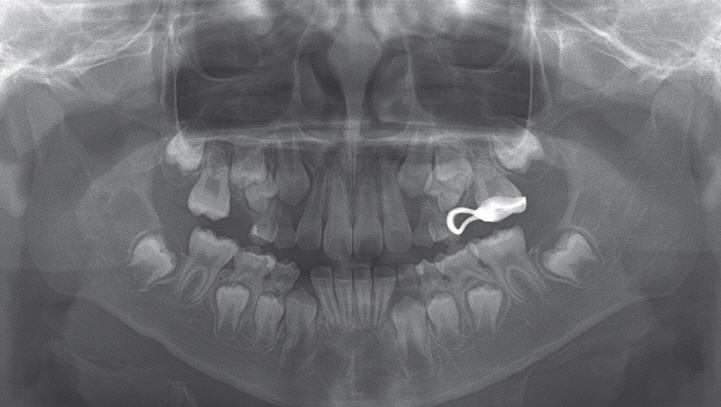
Panoramic radiograph of the patient at age 6. Root resorption of the left primary maxillary second molar ceased after the eruption of the adjacent first molar, while root resorption of the right primary maxillary second molar had progressed excessively.
More than one year later, the patient revisited our hos-pital with a broken arm of the NHA. The arm had been broken several months prior to the presentation. Due to the apparent mesial movement of the maxillary first molar (M1), the space for eruption of the maxillary second premolar (P2) was significantly decreased. However, distalization of M1 was not attempted until the maxillary first premolar (P1) erupted. The eruption space for P2 was completely lost, and about 2.41 mm eruption space deficiency for the contralateral P1 was observed. An NHA connecting P1 to the contralateral M1 was fabricated and installed. Initially, an open coil spring on a 0.016-inch nitinol wire was compressed between P1 and M1 to produce space for Jones jig installation (Fig. 4). One month later, the nitinol wire was exchanged for a 0.020-inch stainless-steel wire. However, the space between P1 and M1 was still inadequate for the placement of the Jones jig appliance.

Intraoral photograph of the patient at the commencement of maxillary first molar (M1) distalization. Initially, an open coil spring was compressed between the maxillary first premolar (P1) and M1. A Nance holding arch was installed to connect P1 to the contralateral M1.
At 3 months, the Jones jig appliance was installed and activated by sliding the eyelet tube distally and ligating it to the bracket on P1 with a 0.014-inch ligature wire (Fig. 5). The appliance was re-activated every month by sliding and ligating the eyelet tube with a new ligature wire. At 7 months, sufficient eruption space for P2 was achieved; the Jones jig appliance was removed, and a passively-fit open coil spring on a 0.018-inch stainless-steel wire was inserted between P1 and M1 for retention (Fig. 6).
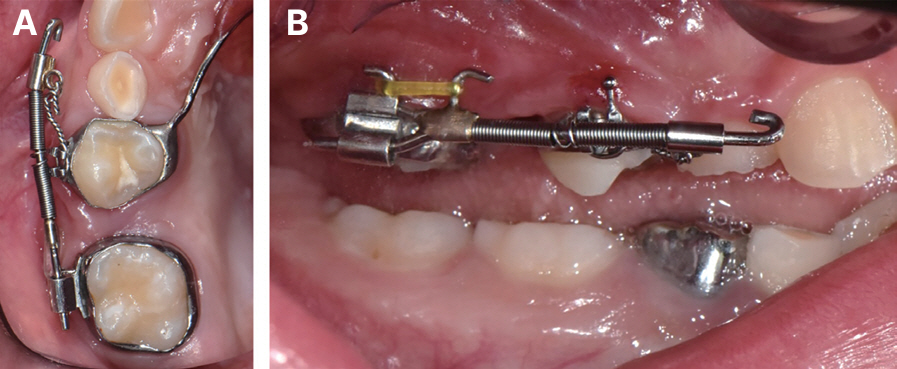
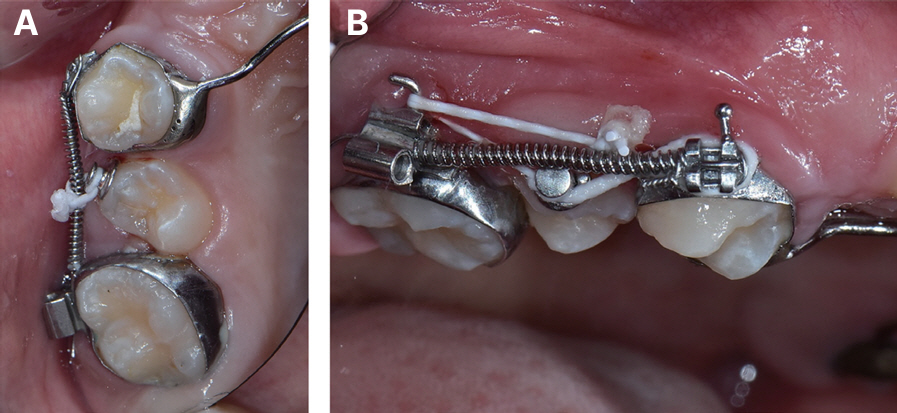
Intraoral photographs of the patient after installation of the Jones jig appliance. (A) A sliding eyelet tube was tied to the bracket welded onto the premolar band with a 0.014-inch ligature wire, (B) The distal part of the sectional jig assembly was inserted into a double-slotted tube welded onto the molar band, and an elastic modulus was engaged to prevent dislocation of the assembly unit.
Intraoral photographs of the patient after removal of the Jones jig appliance. To reduce discomfort from the bulky appliance, an open coil spring on a 0.018-inch stainless-steel wire was passively placed between the maxillary first premolar and the first molar for retention.
At 10 months, P2 erupted palatally. An orthodontic button was bonded onto its buccal surface, and buccal traction was initiated using an elastic thread tied to the open coil spring between P1 and M1 (Fig. 7). Since P2 moved into its normal position at 15 months, all appliances were removed. A positive buccal overjet of P2 and Class I relationship were established. Only 1.93 mm of space deficiency in the right canine was noticed (Fig. 8). Normal overjet and overbite were maintained, implying minimal anchorage loss of anterior teeth during distalization (Fig. 9). A panoramic radiograph taken 6 months after appliance removal showed P2 in its corrected position (Fig. 10).
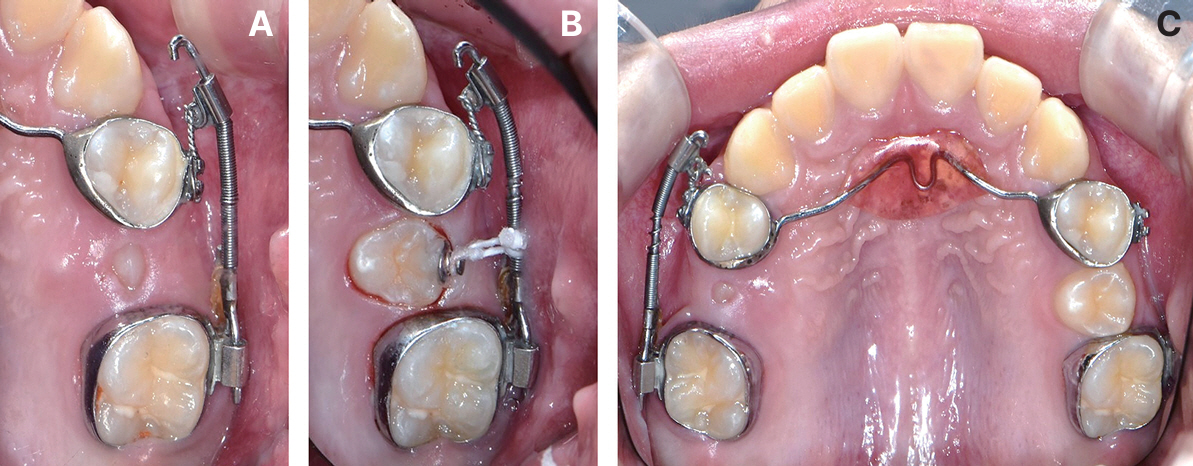
Intraoral photographs of the patient after the eruption of the maxillary second premolar (P2). (A) Since P2 erupted palatally, an orthodontic button was bonded onto its buccal surface and tied to the open coil spring with an elastic thread, (B) After 2 months, the distance between the button and the open coil spring was reduced substantially. An elastic thread was tied to the adjacent teeth in a ‘slingshot’ fashion.

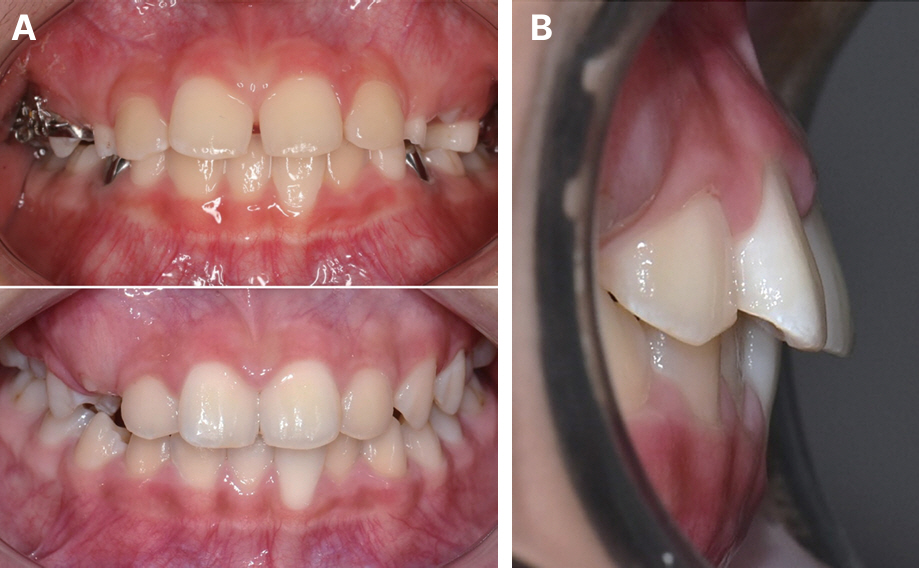
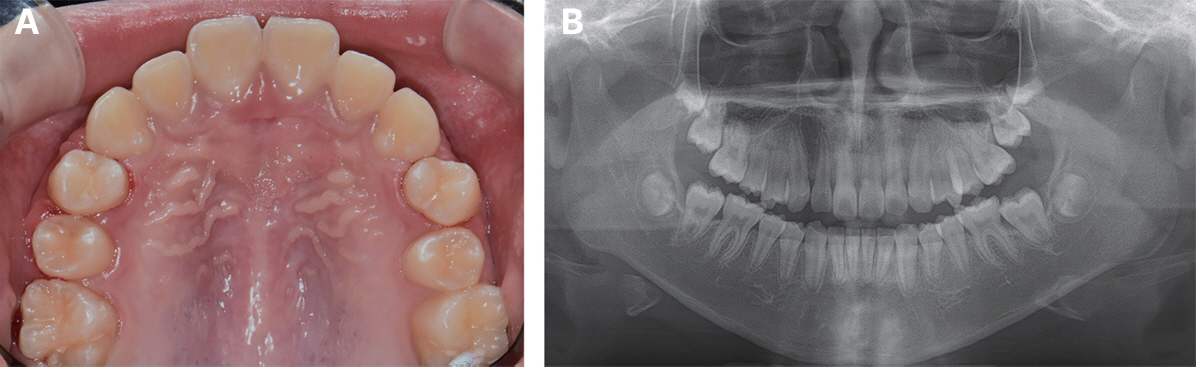
Intraoral photographs of the patient after removal of the appliance. (A) A positive buccal overjet of the maxillary right second premolar (P2) and Class I relationship were established, (B) P2 was aligned into its normal position in the arch. Space deficiency of the maxillary right canine was observed but was not due to anchorage loss during molar distalization. Mild irritation of the palatal mucosa was observed and resolved after a few days. Mild crowding of mandibular anterior teeth was present.
Intraoral photographs of the patient after removal of the appliance. (A) No significant change in overbite was observed, and (B) normal overjet was maintained.
Panoramic radiograph of the patient at age 10, 6 months after removal of the appliance. The maxillary right second premolar is well-maintained in its corrected position.
Case 2
An 8-year-old boy visited Seoul National University Dental Hospital with exfoliation of both primary maxillary second molars. The right primary second molar had been exfoliated 1 - 2 months before his visit, while the left one had been extracted several months earlier and maintained with a band and loop (Fig. 11). Space regaining of both maxillary second premolars (P2) was later planned since the eruption space for both P2s was decreased. The remaining space was maintained with an NHA connecting both maxillary first molars (M1). A year and a half later, both maxillary first premolars (P1) erupted. The previous NHA was removed, and a newer one connecting both P1s was fabricated and installed. Since space between P1 and M1 was completely lost, an open coil spring on a sectional wire was initially compressed between P1 and M1 on each side (Fig. 12). None of the other teeth showed a space deficiency.
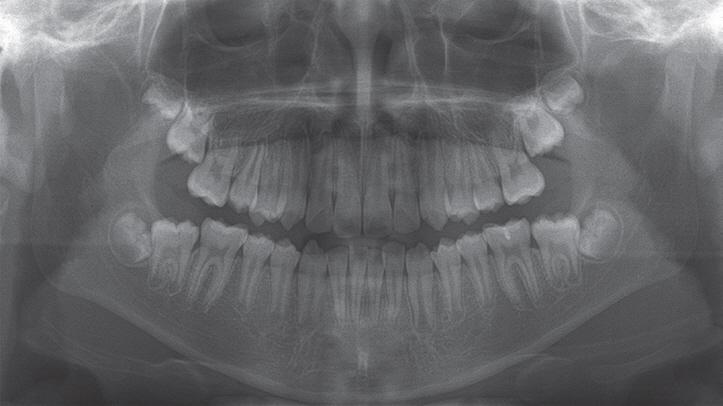
Panoramic radiograph of the patient at age 8 on the first visit. Both primary maxillary second molars had been exfoliated, followed by mesial migration of the adjacent first molars into the eruption space of the succedaneous second premolars. On the left side, the remaining space was maintained with a band and loop.

Intraoral photographs of the patient after the eruption of both maxillary first premolars (P1). Initially, an open coil spring on a sectional wire was compressed between P1 and the adjacent first molar on each side. A Nance holding arch connecting both P1s was fabricated and installed.
One month later, sufficient space had been created on the right side for Jones jig installation. The appliance was installed and activated by sliding the eyelet tube and ligating it to the bracket on P1 in the manner described in the previous case. At 2 months, a left-side appliance was installed and activated in the same manner (Fig. 13). At 5 months, the left P2 erupted palatally. An orthodontic button was bonded onto its buccal surface, and buccal traction was performed using an elastic thread tied to the mainframe of the Jones jig appliance. The left P2 erupted into its normal position at 6 months, and the Jones jig appliance on the left side was removed. Similarly, the right P2 erupted palatally at 11 months. The same traction method as on the left side was instituted until a positive buccal overjet of the right P2 was established (Fig. 14). After one year of treatment, all appliances were removed upon eruption and alignment of both P2s into their normal positions. All teeth were well aligned with no space deficiency (Fig. 15). A recent panoramic radiograph showed that both P2s were well-maintained, and both maxillary second molars erupted without any specific eruption disturbances (Fig. 16).

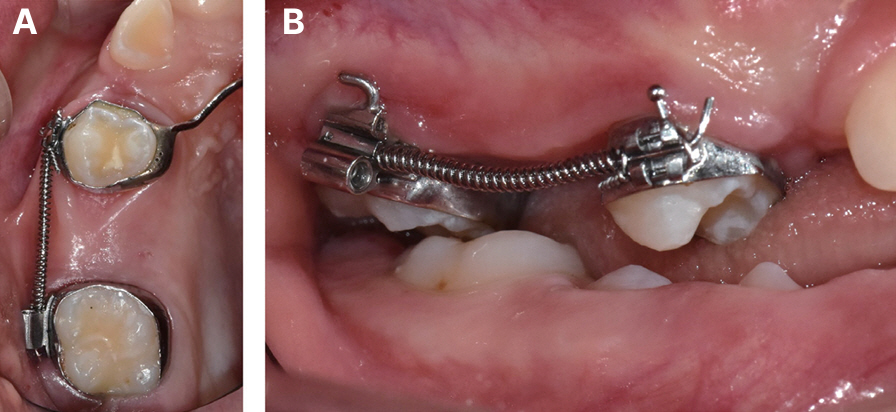
Intraoral photographs of the patient after installation of the Jones jig appliance. A sliding eyelet tube was tied to the bracket welded onto the first premolar band with a 0.014-inch ligature wire to activate the appliance for molar distalization.
(A) Intraoral photograph of the patient 2 months after installation of the Jones jig appliance. The buccal cusp tip of the second premolar (P2) was observed emerging from the palatal mucosa, (B) One month later, the occlusal surface was exposed. An orthodontic button was bonded onto the buccal surface of P2 and tied to the sectional jig assembly with an elastic thread for buccal traction, (C) The Jones jig appliance on the left side was removed since the left P2 was aligned into its normal position. Later, the right P2 also erupted palatally; buccal traction was carried out in the same fashion as on the left side.
(A) Intraoral photograph, (B) Panoramic radiograph of the patient after removal of the Jones jig appliance. Both second premolars were aligned into their proper positions in the dental arch.
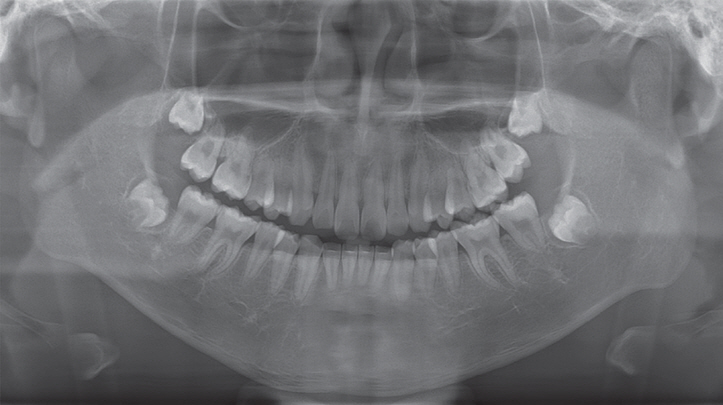
A recent panoramic radiograph of the patient, 2 years after removal of the Jones jig appliance. Both maxillary second molars erupted well without any specific eruption disturbances.
Discussion
Eruption space loss for the maxillary second premolar (P2) due to early exfoliation of its predecessor is usually caused by mesial ectopic eruption of its adjacent first molar. This often occurs in the early mixed dentition period and can be related to various conditions such as cleft lip and palate, short maxilla, mesially inclined eruption pathway of the maxillary first molar (M1), overhanging crown margin of the adjacent primary second molar, and infraocclusion of the adjacent primary second molar [10]. An M1 mesially encroaching into the roots of its adjacent primary second molar may self-correct in certain cases. However, spontaneous correction may not occur in children older than 8 years, in cases of severe root resorption of the primary second molar, or with severely inclined M1 [11-13]. In both of our cases, early exfoliation of the primary second molars was caused by mesial encroachment of their adjacent M1s. In the first case, however, only the right primary second molar exfoliated, while the left one was maintained until its normal exfoliation stage.
Appropriate intervention in a patient with space loss due to mesial migration of M1 should be performed to prevent eruption disturbances of P2. If the primary second molar remains stable for use as an anchor tooth, early distalization of its adjacent M1 can be simply conducted using the Halterman appliance. Unfortunately, if the primary molar becomes mobile or exfoliates prematurely due to severe root resorption, distalization of M1 should be considered after the eruption of P1. The Jones jig appliance can efficiently and effectively distalize M1 during the late mixed dentition period through continuous force applied by an activated coil spring.
The movement rate of M1 is affected by the type and timing of movement. Movement is faster when the molars are distally tipped than when they are bodily moved. In our cases, distalization of M1 consisted of both distal tipping and bodily movement. The amount of distal tipping could be inferred by measuring the angular change of M1 in panoramic radiographs. Both cases showed distal tipping of M1 to a certain degree, but were not large enough to cause any eruption disturbances of the adjacent maxillary second molars (M2). This is shown in a panoramic radiograph taken after the eruption of M2 in our second case (Fig. 16). It is recommended to apply light and continuous force when using the Jones jig appliance to minimize the amount of distal tipping.
Faster movement also occurs before the eruption of M2 [14]. Distalization before the eruption of M2 results in more efficient movement of M1 and less anchorage loss than that after the eruption of M2 [14,15]. In another study comparing the distalization of M1 depending on the M2 eruption stage, distal movement of M1 mostly occurred in a bodily fashion when M2 was erupted, while distal tipping was more pronounced when distalization was performed before the eruption of M2. Distalization of M1 before the eruption of M2 was recommended since longer treatment times and heavier forces were needed after the eruption of M2 [16]. Although Bussick and Mc-Namara Jr [17] did not find any significant differences between the movement rate of M1 before and after the eruption of M2, they pointed out that a smaller increase in lower facial height and a smaller decrease in overbite were prevalent when distalization was performed before the eruption of M2. These studies, however, used nitinol coils or the pendulum appliance for molar distalization. Our literature search yielded few studies on the effect of the M2 eruption stage on the distal movement of M1 when using the Jones jig appliance.
The Jones jig appliance has several advantages over other intraoral distalizing appliances. One of them is that this appliance can aid in the alignment of the palatally erupted P2 [18]. In both of our cases, P2 erupted palatally even though sufficient eruption space was established. With other molar distalizing appliances, such as the pendulum appliance, distal jet, or the Keles slider [19], an additional appliance would be needed to align the palatally erupted P2. A severely palatally positioned P2 can cause crossbite, which leads to extrusion and deep overbite of P2. The development of a crossbite takes more effort to correct, so simple intervention during the eruption stage of P2 is a key benefit of this appliance. However, in some cases, P2 can erupt buccally, as reported in certain literature [20]. In these cases, the Jones jig appliance might disturb the eruption of P2. A cone beam computed tomography image would therefore be necessary to determine the buccolingual position of P2 and the appropriate type of intraoral distalizing appliance.
Another virtue of the Jones jig appliance is that both distal tipping and buccolingual rotation are reduced, since the round and edgewise wires of the distal part of the assembly fit tightly into the tube of M1 (Fig. 1). This aids in the bodily movement of M1, reducing relapse and the time needed for stabilizing the altered position of M1 [8]. In our cases, although not much concern was put about retention after treatment, the corrected positions of P2 and M1 were well-maintained.
A characteristic feature of patients whose primary maxillary second molar has been exfoliated earlier than its normal exfoliation stage is that the adjacent M1 rotates mesio-palatally around its palatal root. This can be noticed in the first case before treatment (Fig. 4). Since the line of action lies buccal to the center of resistance, M1 is rotated disto-buccally during distalization [21]. This is one of the differentiated advantages of the Jones jig appliance over palatally acting distalizing appliances such as the pendulum.
Clear aligners have several advantages over conventional intraoral distalizing methods, including the Jones jig appliance. M1 can be distalized up to 2.0 - 3.0 mm without causing significant distal tipping [22]. Also, clear aligners provide better control of the occlusal vertical dimension, while an increase in lower facial height is present when using the Jones jig appliance [23]. Despite these advantages, we recommend using the Jones jig appliance over clear aligners for two reasons. 1) The treatment effect when using clear aligners highly depends on patient cooperation. 2) The amount of distalization required to create space for the eruption of P2 exceeds the normal range created by clear aligners.
Loss of anchorage is of main concern when using intraoral distalizing appliances. This manifests as mesial movement of P1 and protrusion and extrusion of the upper incisors, causing an increase in overjet. A superimposition image of the pre-treatment and post-treatment lateral cephalometric radiographs is essential to accurately compare the positional and angular changes of the premolars and incisors. Unfortunately, we did not take any lateral cephalometric radiographs of the patients. Instead, some post-treatment intraoral photographs showed that protrusion and extrusion of the incisors were minimal (Fig. 9).
Jones and White [5] reported no anchorage loss when using the Jones jig appliance, while Gulati et al. [8] reported 1.05 ± 0.87 mm mesial movement of P1 and 1.10 ± 0.83 mm increase in overjet. Brickman et al. [24] showed mesial movement of 2.0 mm and mesial tipping of 4.76o of P1. However, overjet increase and incisor labioversion were not as severe as those of other intraoral distalizing appliances, such as repelling magnets, nitinol coil springs, or the pendulum appliance. Conflicting results were shown in another study in which mesial tipping was greater when using the Jones jig appliance [25], and a separate analysis of tooth movement when using the Jones jig appliance revealed that only 46% of the space created between M1 and P2 was due to distalization of M1 [26]. In the latter study, however, M1 and M2 were simultaneously distalized, which could have contributed to greater anchorage loss.
The resistance to anchorage loss depends on several factors, such as distalization force [8], the size and number of teeth incorporated in the anchorage unit [25], the lack or inconsistency of contact points between spaced or severely crowded anterior teeth, and the shape of the palatal vault [26]. In cases where there are insufficient teeth to incorporate into the anchorage unit, miniscrews implanted in the anterior paramedian region can be used to reinforce anchorage [27]. The use of J-hook headgear or Class II elastics has been proposed [24] but would require patient cooperation, negating the advantage of intraoral appliances.
Temporary anchorage devices (TADs) provide absolute anchorage and can thus minimize unwanted tooth movements. According to a systematic review, inter-radicular TADs result in less distal tipping but also less amount of distalization. Meanwhile, distalization using palatal TAD-supported appliances showed greater distal tipping [28]. Depending on our clinical experience, children of school age lack bone quality for stability of TADs. Thus, using TADs over the Jones jig appliance has few advantages for molar distalization in the mixed dentition period.
When using the Jones jig appliance, it may be beneficial to position the double-slotted tube of M1 gingivally to minimize distal tipping. Since the center of resistance is located near the trifurcation of the root, a shorter distance to the line of action will cause lesser distal tipping of M1 [8]. Shetty et al. [29] pointed out that patients should be told to follow up for breakage of the ligature wire connecting the eyelet tube to the bracket on P1. A broken ligature wire is not easily detectable by patients, and repeated break-offs might cause relapse, extending treatment time. This was prevented using a 0.014-inch Kobayashi wire, which is usually used with up-and-down elastics during the finishing stage of fixed orthodontic treatment. In neither of our cases did the patient present with a broken ligature wire.
Summary
Both of our cases demonstrate distalization of the maxillary first molars and eruption guidance of the maxillary second premolars using the Jones jig appliance. Characterized by many advantages and with precise anchorage control, the Jones jig appliance can be effectively used for molar distalization, especially for space regaining of the maxillary second premolar. The intervention decision of patients with early exfoliation of the primary maxillary second molar is important to prevent further malocclusion in the mixed dentition period.
Notes
Conflict of Interest
The authors have no potential conflicts of interest to disclose.