



ŌģĀ. Introduction
The first permanent molar is the largest and strongest tooth in the oral cavity and has well developed cusps and roots, which contribute to maintaining the vertical dimension of the face[1]. In addition, the first permanent molar can play an important role not only in providing maximum anchorage force during orthodontic treatment, but also in the mastication[1].
The prevalence of eruption disturbances of the mandibular first permanent molars is known as approximately 0.01%[2,3]. Eruption disturbances can cause multiple problems, such as malocclusion, short lower facial height, cyst formation, overeruption of the antagonist tooth, inclination and root resorption of adjacent teeth, and pericoronal inflammation[4,5]. The diagnosis and management of eruption disturbances are important, especially in children and young adults who are in stage of maxillofacial development.
The treatment plan of eruption disturbances of mandibular first molars should be chosen according to intraoral condition or patientsŌĆÖ circumstances. Various treatment techniques such as periodic observation, surgical exposure, orthodontic traction after surgical exposure, orthodontic traction with subluxation, surgical repositioning, and extraction can be applied[6,7]. Impaction of the mandibular first molar is diagnosed during the mixed dentition, and generally treated by orthodontic traction[8,9]. Among the treatment techniques, orthodontic traction following surgical exposure has the highest success rate[10]. But the patientŌĆÖs compliance does matter as the treatment time increase with a traction appliance being used[8,10].
This study aimed to introduce and describe the use of a novel traction appliance with a cantilever-type spring, in treatment of eruption disturbances of the mandibular first permanent molar.
ŌģĪ. Case Reports
This case report was approved by the Institutional Review Board (IRB) of Pusan National University Dental Hospital (IRB number: PNUDH-2020-019).
1. Case 1
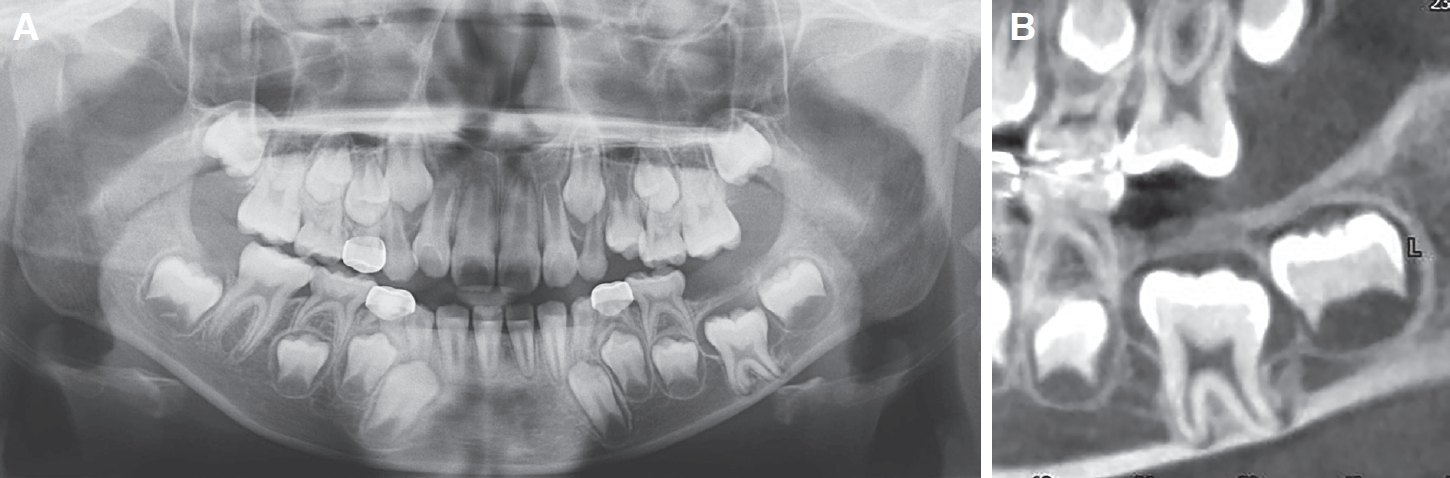
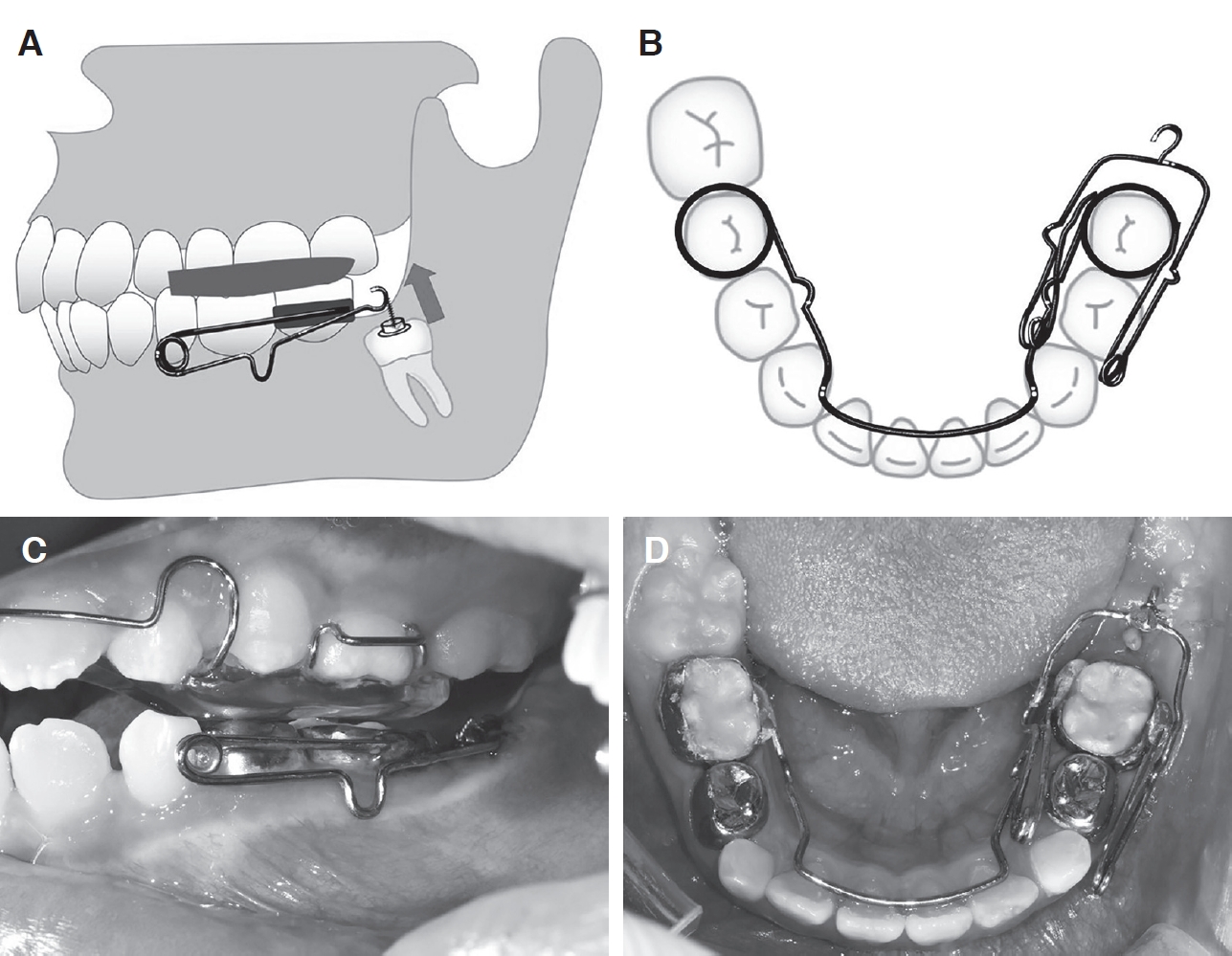
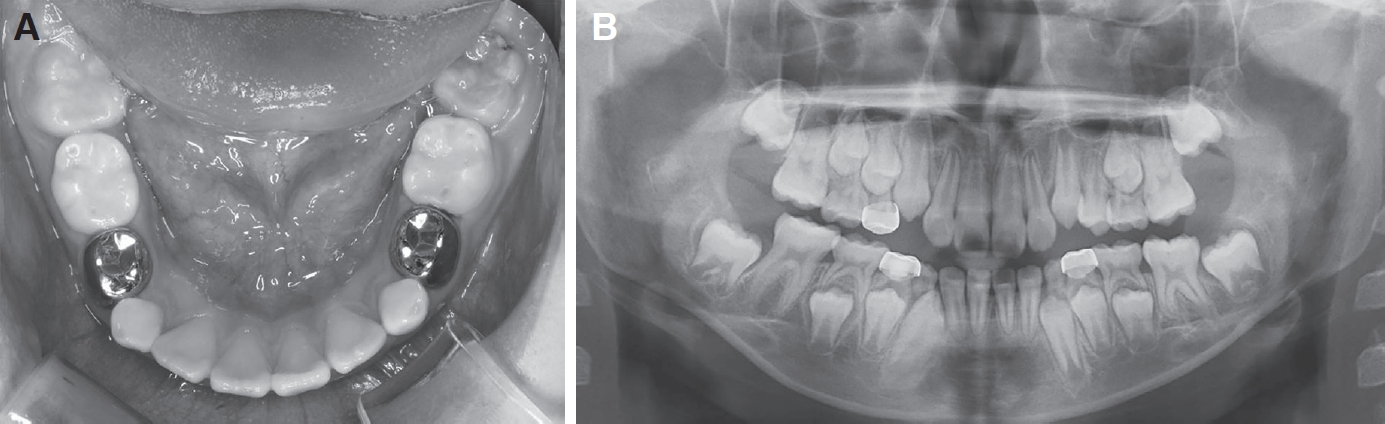
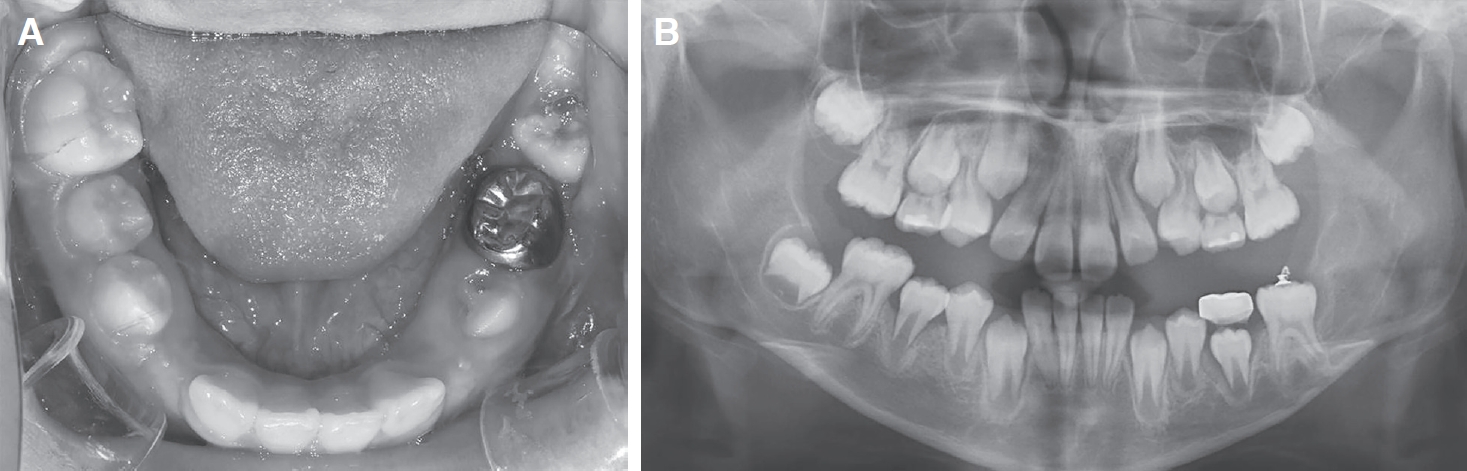
A 9-year-old boy visited department of pediatric dentistry in Pusan National University Dental Hospital with delayed eruption of the mandibular left first permanent molar. There was no medical or dental history. Oral examination assured the absence of the mandibular left first permanent molar (Fig. 1). On radiographic examination, panoramic image showed that the roots of the mandibular left first permanent molar and lower margin of mandible were in contact. The widening of follicular space around the coronal part of impacted tooth was also evident (Fig. 2A). Cone beam computed tomography (CBCT) image confirmed dilacerated roots of the impacted tooth because of the downward spatial deficiency (Fig. 2B). The patientŌĆÖ s compliance was evaluated as second grade by Frankl behavioral classification and isolation from saliva was expected as difficult during the chairside surgery. Considering the patientŌĆÖ s compliance and technical difficulties, surgical exposure was planned under general anesthesia. The bone covering the impacted tooth was eliminated to expose the crown and an orthodontic assembly consisting of a button and wire was attached. A lingual arch type fixed appliance including a cantilever spring was used in the mandible for the traction of the mandibular left first permanent molar. A removable appliance with a posterior bite plate was used in the maxilla. It can prevent the overeruption of the maxillary left first permanent molar and create space for traction (Fig. 3A, 3C). The lingual arch of the traction appliance and the cantilever spring were made from 0.9 mm and 0.7 mm stainless steel wire, respectively (Fig. 3B, 3D). The traction force was approximately 150 g. The fixed appliance was removed when the impacted mandibular left first permanent molar had erupted into the oral cavity. The marginal ridges of the impacted molar and adjacent primary molar were comparable at that removal time (Fig. 4A, 4B). Both the mandibular fixed appliance and maxillary removable appliance were used for 3.5 months.
2. Case 2
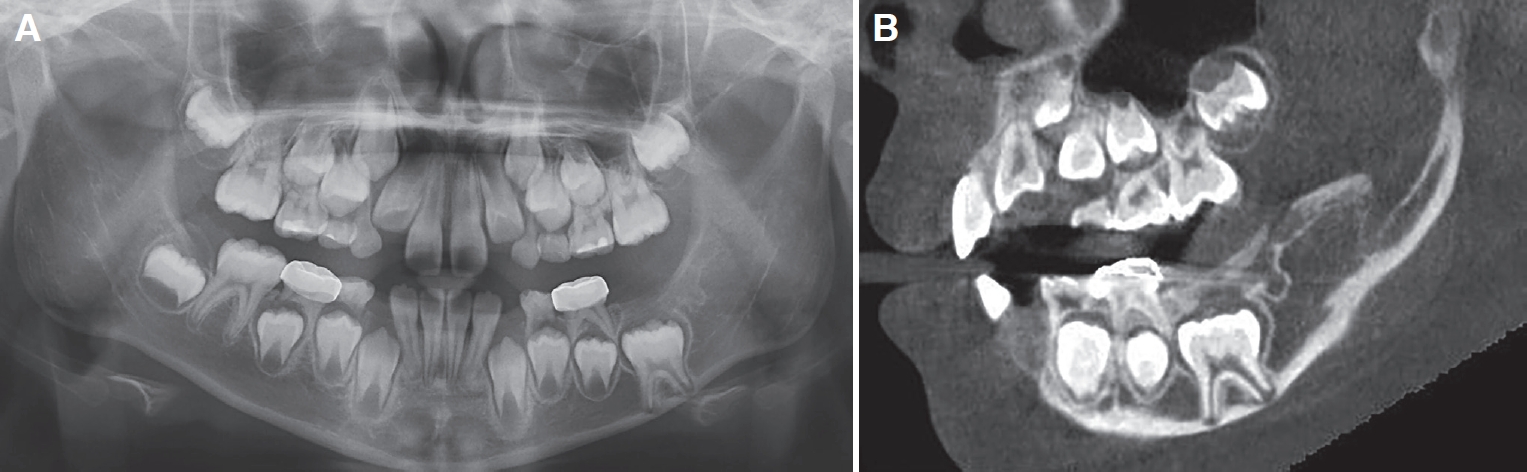
A 7-year-old girl visited department of pediatric dentistry in Pusan National University Dental Hospital with delayed eruption of the mandibular left first permanent molar. There was no medical or dental history. Clinical examination confirmed the absence of the first permanent molar in the left mandible (Fig. 5). On radiographic examination, impaction of the first permanent molar was evident and the second permanent molar was congenitally absent (Fig. 6A). On the CBCT images, a radiopaque material above the crown of the mandibular left first permanent molar was apparent. In comparison to the roots of the mandibular right first permanent molar, it was apparent that the roots of the impacted tooth were almost completely developed and in contact with the mandibular margin (Fig. 6B). This patient was treated according to the same protocol described in case 1 (Fig. 7A, 7B). Both the mandibular fixed appliance and maxillary removable appliance were used for 5 months (Fig. 8A, 8B).
Ōģó. Discussion
The first permanent molar in the mandible initially erupts into the oral cavity at approximately 6 to 7 years of age, while the root only completes its development around 9 to 10 years of age[11]. On clinical examination, when the mandibular first permanent molar is not evident intraorally after 6 - 7 years of age, radiographic examination is essential to confirm a diagnosis of eruption disturbances. In addition, the relationship between tooth eruption and root development should be evaluated. Kokich and Mathews[12] and Johnson and Quirk[13] have reported that it is possible for an impacted tooth to erupt when the root is still developing. Also they pointed out that once the root apex is completely formed and closed, spontaneous eruption is difficult to occur. When considerable root development has taken place without eruption of the tooth into the oral cavity, eruption disturbances should be suspected. Generally, the distance between the roots of permanent molars and the inferior alveolar nerve is constant, it could be used as the basis for diagnosing eruption disturbances[11]. The CBCT images of both cases revealed that the roots of the impacted teeth were almost completely developed and located near the inferior alveolar nerve relative to the contralateral side.
According to Raghoebar et al.[4], eruption disturbances of permanent teeth can be classified into three categories. Impaction means cessation of eruption when there is a physical barrier in eruption path or the tooth is in abnormal position[4,14]. Primary retention refers to the case in which the tooth fails to erupt even when the tooth is in good position before eruption or no physical obstacles is in eruption path. Conversely, secondary retention refers to the case in which the tooth does emerge into the oral cavity, but fails to erupt further. It is the main etiological factor of tooth ankyloses. Depending on the etiology of the eruption disturbance, different treatment approaches are required[4]. In case 1, follicular widening was observed, while in case 2, a radiopaque material was evident above the impacted molar. Both cases were diagnosed as impaction, an eruption disturbance due to a physical obstacle.
Treatment of an impacted mandibular first permanent molar involves surgical exposure of the tooth, removal of the physical barrier prohibiting eruption, and periodic follow-up. When the tooth still fails to erupt, orthodontic traction and surgical repositioning can be applied[15-17]. Surgical extraction of the impacted tooth may be considered when all of these trials failed and additional pathological findings were observed[8]. Nielsen et al.[9] have reported that normal eruption of mandibular first molars with an eruption disturbance could be possible when diagnosed and treated early. In particular, when the root apex was not completely closed and the hard and soft tissue covering the tooth was surgically removed, spontaneous eruption can be expected. In cases presented here, the root development of impacted teeth was almost completed compared to the contralateral molars and the roots were dilacerated being close with lower margin of mandible. Those clinical and radiographical signs confirmed that immediate intervention including surgical exposure and orthodontic traction was unavoidable.
There are several types of traction appliances such as removable intermaxillary traction appliance, traction appliance using a miniplate as a skeletal anchorage, and modified Halterman appliance used for traction of impacted mandibular first molar. Removable intermaxillary traction appliance is easy for clinicians to manufacture and for children to keep good oral hygiene. But the disadvantage of this appliance is that it demands high level of patientsŌĆÖ compliance[18]. In the case of a traction appliance using a miniplate, it has the benefits of obtaining skeletal anchorage, but can cause discomfort due to inflammation around the miniplate. Also, additional surgery to remove the plate is required[19]. The modified Halterman appliance is easy to manufacture and less affected by patientsŌĆÖ compliance. But it is mainly used for distal traction of the mandibular first molars that are impacted mesially[20,21].
In these cases, the position of the double helix of the appliance was designed to be located between the mandibular deciduous canine and the deciduous first molar to apply traction force upward. Load deflection rate (LDR) is reflected so that a light force can be continuously applied by forming a Uloop and a double helix[22]. According to Romeo, an extrusion force of 165 g is sufficient for a posterior tooth[23]. Based on this, approximately 150 g of force was applied to the impacted tooth by adjusting the U-loop in this study.
According to Jo et al.[10], the traction period required in the eruption of impacted mandibular permanent first molar was an average of 15.6 months, having the longest traction period compared to those of other teeth. In the study of Seo et al.[24], a fixed traction appliance was selected more than a removable one. The average traction time with a fixed appliance was 7.4 months and it took 1.7 months less compared to using a removable appliance in that study. In the present case report, traction force was applied for 3.5 and 5 months, respectively. A fixed traction appliance was selected in both cases to reduce the influence of patientsŌĆÖ compliance.
In order to use a fixed traction appliance to treat a mandibular first permanent molar with an eruption disturbance, a mandibular second deciduous molar with intact roots are essential. Posterior bite plate can make traction space and prevent the overeruption of the antagonist tooth. The traction appliance described in this study has a shorter treatment period and requires relatively less patientsŌĆÖ compliance than that of conventional traction appliances. In addition, this appliance provides continuous traction force through direct connection with the ligature wire and can control the force by adjusting the U-loop.
Simplifying the design of the traction appliance is recommended as it is bulky and complicated, making it difficult to keep good oral hygiene.
Surgical exposure was planned under general anesthesia because mandibular first molars in these cases were deeply impacted and patientsŌĆÖ compliance were highly demanded. For this reason, it is better to perform the surgical procedure at a dental hospital equipped with general anesthesia equipment.
Compensatory intrusion and root resorption of the mandibular second deciduous molars were observed in both cases. Especially in case 2, root resorption of the mandibular second deciduous molar occurred rapidly. The appliance had to be removed when the mandibular left first permanent molar had only partially erupted. Park et al.[25] also reported that occlusal force, oral habit, and increased overbite can lead abnormal rapid root resorption of primary teeth. Therefore, comprehensive evaluation by clinical examination is necessary whether the roots of deciduous second molar are intact and the patient has oral habits or not. When rapid root resorption of the mandibular deciduous second molars used as anchorage is expected, another traction method should be tried.
ŌģŻ. Summary
Eruption disturbances of the mandibular first permanent molar are very rare and can cause multiple problems in occlusal development. Early diagnosis and guidance of impacted tooth into the correct position are very important. In the present case report, a fixed cantilever-type appliance was used in children with intact mandibular second deciduous molars to guide the eruption of the mandibular first permanent molars into the oral cavity. This appliance reduced the influence of patientsŌĆÖ compliance on treatment outcome and induced the eruption of the impacted mandibular first permanent molar within a short time. In the treatment of eruption disturbances of mandibular first permanent molars in a mixed dentition, this appliance can be an efficient alternative to the traditional treatment options.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






