



Introduction
The term “tooth eruption” often refers to the moment a tooth emerges into the oral cavity. However, it is defined as the process by which a tooth transitions from its developmental position within the alveolar bone to its functional position within the oral cavity and continues to erupt gradually throughout one’s lifetime, even after achieving occlusion [1]. If the process of tooth eruption does not occur properly, it can disrupt the formation of a normal dental arch and hinder facial growth [2]. Therefore, timely treatment is of utmost importance; a delay can complicate the treatment and lead to a poorer prognosis.
Age, tooth morphology, gender, and individual characteristics are some variables that affect the timing of tooth eruption [3]. Accordingly, it is necessary for a dentist to diagnose whether all permanent teeth follow a normal eruption process at the appropriate time [4]. Delayed tooth eruption (DTE), where teeth erupt later than the normal eruption period, can be clinically observed without the need for radiographic imaging. Timely discovery of DTE aids in the formulation of a comprehensive treatment plan [5]. DTE includes chronologic DTE, wherein eruption is delayed beyond the chronological age, and biologic DTE, wherein eruption is delayed despite the complete development of two-thirds of the root [5]. The treatment methods for DTE are categorized as follows: follow-up, space maintenance after primary tooth extraction, orthodontic traction, surgical exposure, replacement after extraction of a tooth with a delayed eruption (via autotransplantation, prosthetics, or implant), and space regaining [5-7].
The eruption process of mandibular premolars occurs vertically [8]. The prevalence of eruption disturbances among Koreans is 4.5%, with mandibular premolars accounting for 7.2% of these cases, and the leading causes are an abnormal eruption pathway and DTE [9]. The prevalence of eruption disturbances among Japanese individuals was 4%, with mandibular premolars accounting for 12.4% of these cases [10]. In addition, the prevalence rate of impacted mandibular premolars is reported to be 0.2% - 0.3% [11]. Disturbances in tooth eruption may lead to issues such as space loss, collapse of occlusion, and resorption of the adjacent tooth roots [6,12].
Therefore, this study aims to explore DTE to intervene at the appropriate time in cases of eruption issues with mandibular premolars. Clinically, the prevalence of DTE in permanent teeth was reported to be 4.3% [4]. Studies on DTE in permanent and retained primary teeth, eruption disturbances in mandibular premolars, and systemic conditions associated with DTE have been conducted previously [6,12-17]. However, the prevalence of DTE in mandibular premolars and the criteria for selecting treatment methods, apart from chronological age and degree of root development, remain unclear. The choice of each treatment method is determined by the clinician [4,5,7,12,17,18]. Therefore, the goal of this research is to investigate the prevalence, causes, average treatment duration, and distribution of dental conditions according to treatment methods in cases of DTE of mandibular premolars.
Materials and Methods
This study was conducted with approval from the Institutional Review Board (IRB) of Seoul National University Dental Hospital (IRB No: S-D20210029).
1. Study subjects
Patients aged 9 - 15 years with delayed eruption of mandibular premolars who visited the Seoul National University Dental Hospital and had panoramic radiographs taken from January 1, 2017, to December 31, 2020, were included in the study. Those with systemic conditions or genetic disorders [5,7] that could influence the tooth-eruption process were excluded.
2. Research Methodology
The following parameters were investigated using the patients’ electronic medical records and panoramic radiographs by a single dentist: age, gender, location of the tooth with DTE, stage of root development, stage of eruption, impaction depth, angle of inclination, causes of DTE, treatment methods, and treatment duration. In cases where previous treatment had failed, and a different treatment approach was adopted, the study focused on the final treatment method that was ultimately implemented.
The definition of delayed eruption followed the chronologic DTE criteria established by Suri et al. [5], which signifies the tooth has not erupted despite a period twice the standard deviation beyond the average eruption age of the specific tooth. Oh et al. established the preeruption stage as 0% of the eruption stage and the stage where occlusal contact was achieved as 100% of the eruption stage, defining eruption as the stage at 50% eruption [19]. Therefore, for the assessment of average eruption ages for each tooth, Oh et al. used the eruption stage as the reference point, setting it at 50%. In this study, we followed this definition as the basis for assessing eruption timing.
1) Stages of root development
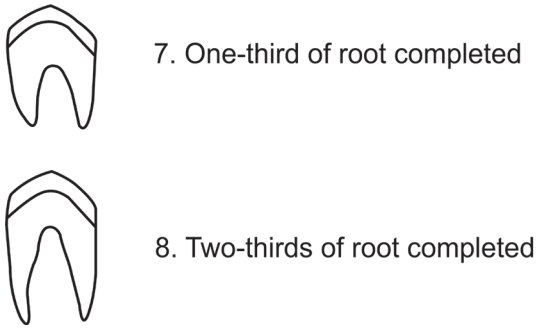
The stage of root development was assessed according to the Nolla method for the calcification stages of permanent teeth [3]. As mentioned in the study by Suri et al. [5], biological DTE is defined as teeth that do not erupt despite having formed two-thirds or more of the root. Following this definition, teeth with one-third or less root formation were classified as Nolla stage 7 or lower, and those teeth with two-thirds or more root formation were categorized as Nolla stage 8 or higher (Fig. 1).
2) Eruption stage
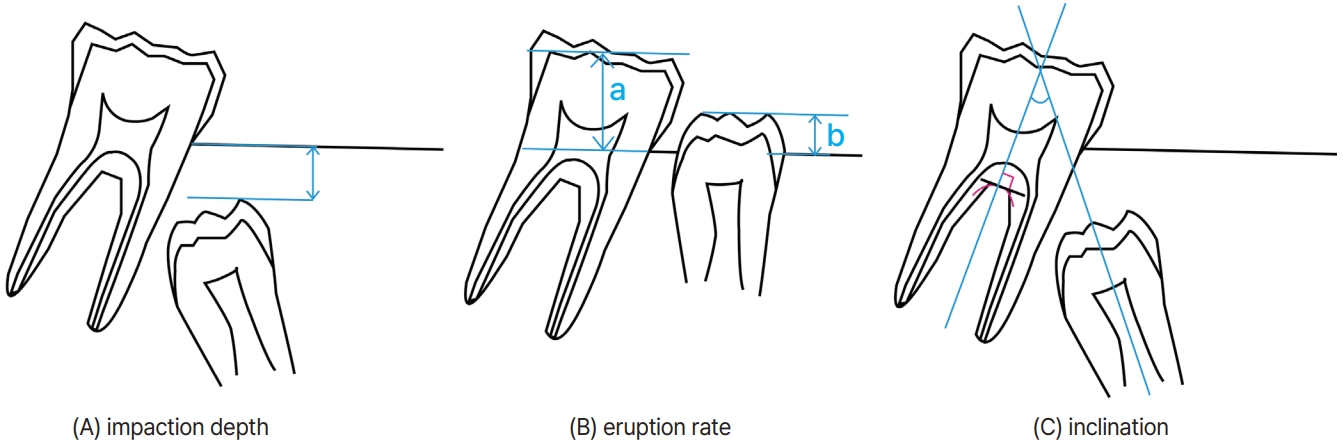
We defined the stages of tooth eruption as follows: impaction depth exceeding 1.0 mm beyond the pre-eruptive stage (stage 0); impaction depth within 1.0 mm of the pre-eruptive stage (stage 1); eruption stages 0% - 20% beyond the pre-eruptive stage (stage 2); and eruption stages 20% - 50% beyond the pre-eruptive stage (stage 3). The eruption of unerupted permanent teeth takes about 4 to 5 months to pass through 1.0 mm of alveolar bone in the premolar area [20]; therefore, stages 0 and 1 were divided based on an impaction depth of 1.0 mm for teeth. The impaction depth of the pre-eruption stage followed the definition by Ismail et al. [17], which is the distance between the most superior edge of the crown of the premolar and the mesial portion of the cemento-enamel junction of the first permanent molar. The eruption stages in teeth beyond the pre-eruptive stage were classified by the ratio of the clinical crown length of the premolar to that of the first molar, subsequently multiplied by a factor of 100 (Fig. 2). When the eruption rate was 20% or less, it was considered as a state where the cusp tip of the mandibular premolar was showing. When the eruption rate ranged from 20% to 50%, it corresponded to a condition where the occlusal surface of the mandibular premolar was observable. Therefore, we defined the boundary between stage 2 and stage 3 as an eruption rate of 20%.
3) The angle of inclination of the mandibular premolar axis
The angle of inclination of the mandibular premolar axis followed the definition by Ismail et al. [17]. A perpendicular line drawn tangent to the most conspicuous portion of the bifurcation area of the root was described as the axis of the mandibular first molar, whereas the axis of the mandibular premolar was defined as the line connecting the apex and the top of the premolar’s most centered cusp (Fig. 2). The angle created between the mandibular premolar axis and the mandibular first molar axis, measured downwards, was designated as the angle of inclination of the mandibular premolar axis (Fig. 2) [17].
4) Etiology of DTE
The causes of delayed eruption were investigated and categorized into the following groups: non-specific findings, benign tumor, odontoma or supernumerary tooth, periapical or inter-radicular lesion, ankylosis of the primary molar, space deficiency, abnormal eruption pathway, and developmental anomaly. Periapical cysts and pericoronal odontogenic cysts associated with periapical or inter-radicular lesions were included within the periapical or inter-radicular lesion category.
5) Treatment methods
The treatment methods for DTE were categorized as follows: follow-up, space maintenance after primary molar extraction, space regaining, orthodontic traction, and surgical treatment. The procedures encompassed under the category of surgical treatment included the removal of odontomas, supernumerary teeth, adjacent malformed teeth, and benign tumors, surgical exposure without orthodontic traction (including gingivectomy), autotransplantation, and extraction of the affected tooth.
6) Treatment duration
A total of 412 teeth classified under DTE were investigated for the Nolla stage, eruption stage, and treatment duration based on the treatment methods, excluding cases where treatment was not completed during the specified period, or the patients did not return for treatment completion. However, teeth treated by autotransplantation or extraction were defined with a treatment duration of 0 and excluded from the statistical analysis for treatment duration.
7) Depth and inclination
The depth and inclination of teeth corresponding to the pre-emergent stages, stage 0 and stage 1, were investigated for their 95% confidence intervals (CI) based on the treatment methods. This analysis included the teeth treated by autotransplantation or extraction, which were excluded from the treatment duration analysis.
3. Statistical analysis
All radiographic image interpretations were performed by a single dentist to minimize inter-rater variability. A subset of 100 randomly selected panoramic radiographs from the study subjects was re-evaluated at a two-week interval to assess the intra-rater reliability of the researcher. Weighted Cohen’s kappa was used to evaluate the reliability of the developmental stage of each tooth. The intra-observer agreement was high, with a Cohen’s kappa of 0.968 (p < 0.0001), indicating substantial reliability.
The prevalence of delayed eruption of mandibular premolars was compared according to gender and location using the Chi-square test. The significance of treatment duration based on the root development stage, eruption stage, and treatment method was assessed using Student’s t-test and one-way analysis of variance (ANOVA). The statistical analyses were performed using SPSS software (version 26.0, IBM, Chicago, IL, USA).
Results
1. Prevalence
A total of 4,892 patients (2,321 females and 2,571 males) were examined; 254 patients (120 females and 134 males) were finally included in the study. The prevalence of mandibular premolar DTE among the 412 teeth with DTE examined in this study was 5.19%. While a slightly higher prevalence was observed in males, there was no statistically significant difference between genders (p= 0.94). Similarly, no statistically significant difference in prevalence was observed between genders for the mandibular first premolars and mandibular second premolars (Table 1, mandibular first premolar p= 0.76, mandibular second premolar p= 0.81).
Among a total of 17,546 mandibular premolars, the prevalence of DTE was 0.76% for mandibular first premolars and 4.39% for mandibular second premolars (p < 0.0001; Table 1). This difference was statistically significant. However, no statistically significant difference in prevalence was observed between the left and right sides for the delayed eruption of mandibular premolars (p= 0.92; Table 1).
2. Distribution of teeth with DTE according to the etiology and treatment methods
An investigation into the distribution of the causes of DTE among 293 treated mandibular premolars with delayed eruption revealed that non-specific findings accounted for the highest proportion at 78.84%, and cases attributed to benign tumors represented 1.37%, including ameloblastic fibro-odontoma and odontogenic keratocyst. The leading cause of DTE was periapical or interradicular lesions in primary teeth, accounting for 7.85%. Follow-up was the predominant treatment method for cases with no specific cause. Cases in which benign tumors, odontomas, and supernumerary teeth were identified as the cause of DTE underwent surgical treatment. DTE caused by periapical or inter-radicular lesions, an-kylosis of the primary molar, space deficiency, abnormal eruption pathway, and developmental anomalies in mandibular premolars was treated using various methods (Table 2).
3. Distribution of DTE etiology according to the root developmental stage
Among the 293 teeth, 55 presented with root development at 1/3rd completion or less (Nolla stage 7 or lower), and 238 with root development at 2/3rd completion or more (Nolla stage 8 or higher). Nonspecific findings were predominant in both instances, and cases attributed to periapical or inter-radicular lesions were the most common. Variations in the order of high proportion causes were observed between Nolla stages 7 or lower and Nolla stages 8 or higher (Table 3).
4. Success rate by treatment methods
We investigated the success rate by treatment methods among 293 teeth, comparing cases where the treatment method was changed to a different one with cases where the treatment was completed using the initial method. The treatment method with the highest success rate was “space regaining,” which showed a 100% success rate. On the other hand, the treatment method with the lowest success rate was “orthodontic traction,” which exhibited an 80.00% success rate (Table 4)
5. Treatment duration according to the root developmental stage
Out of the 293 teeth, 7 teeth treated by autotransplantation or extraction were excluded, leaving 286 teeth for the treatment duration analysis. The total treatment duration for teeth with Nolla stage of 7 or lower was significantly (p < 0.0001) higher at 22.89 months than that for teeth with Nolla stage of 8 or higher (15.02 months; Table 5).
6. Treatment duration according to the eruption stage
The total treatment duration was 20.84 months for stage 0, 12.02 months for stage 1, 11.69 months for stage 2, and 8.28 months for stage 3, with significant differences observed between stages (p < 0.0001; Table 6).
7. Treatment duration according to the treatment method
The total treatment duration was 15.82 months for cases treated with the follow-up method, 16.33 months for those treated with space maintenance after primary molar extraction, 10.35 months for cases treated by space regaining, 15.97 months for those treated by orthodontic traction, and 17.87 months for cases treated with surgical treatment (Table 7). No statistically significant differences were observed between each treatment method (p= 0.43).
8. Distribution of impaction depth and inclination angle according to the treatment method
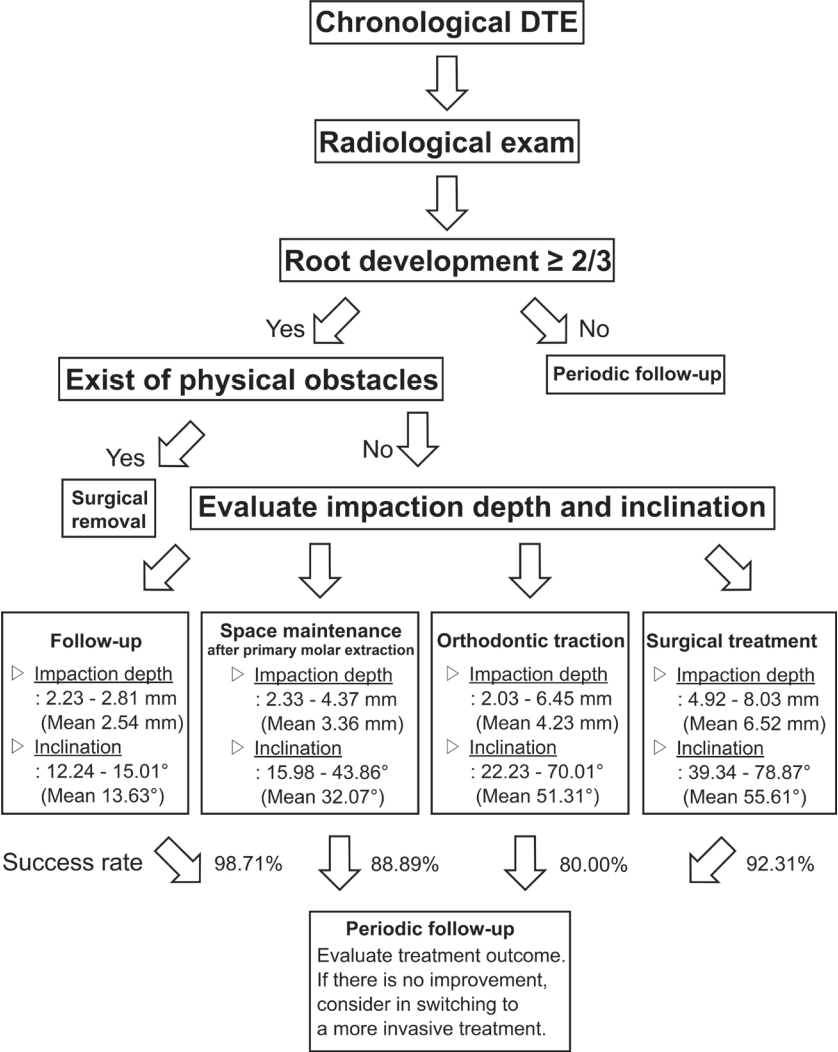
For cases corresponding to the pre-emergent stages, stage 0 and stage 1, a total of 235 impaction depths and inclination angles were examined upon treatment completion. In cases treated with the follow-up method, the 95% CI for impaction depth was 2.23 to 2.81 mm, and the inclination angle ranged from 12.24° to 15.01°. For cases where space maintenance was performed after primary molar extraction, the 95% CI for impaction depth was 2.33 to 4.37 mm, and the inclination angle ranged from 15.98° to 43.86°. In cases treated with space regaining, only three instances were applicable for statistical significance; therefore, the minimum and maximum values were determined instead of the 95% CI. The minimum and maximum values for impaction depth were 1.22 mm and 7.56 mm, respectively, while the minimum and maximum values for inclination angle were 3.25° and 54.71°. This value may have statistical errors due to a very small sample size. The 95% CI for impaction depth and the inclination angle in cases treated with orthodontic traction were 2.03 to 6.45 mm and 22.23° to 70.01°, respectively. The 95% CI for impaction depth for surgical treatment cases was 4.92 to 8.03 mm, and the inclination angle ranged from 39.34° to 78.87° (Table 8).
Discussion
This study aimed to determine the prevalence, causes, treatment duration, and tooth condition in cases of delayed eruption of the mandibular premolars. In the current study, a prevalence rate of 5.19% for DTE in mandibular premolars was observed, with no statistically significant differences based on gender or side. Furthermore, consistent with previous studies [4,6,21], a higher prevalence of DTE in mandibular second premolars than in mandibular first premolars was observed. Although the prevalence reported in this study was higher than that (4.3%) reported by Johnsen in permanent teeth [4], a direct comparison between the two studies is challenging due to differences in the types of teeth examined. Additionally, Johnsen observed that delayed eruption predominantly occurred in mandibular second premolars and attributed the most common cause of DTE in permanent dentition to insufficient space for the eruption of succedaneous permanent teeth. The differences in findings between the two studies may be attributed to the fact that Johnsen’s study included all the permanent teeth, whereas this study focused solely on the mandibular premolars.
In the study by Henklein et al. [18], which focused on DTE in permanent teeth with Nolla stage 8 or higher, 70.7% of the DTE was observed in premolars; moreover, 68.7% of the cases were not associated with any specific reason, but featured retained primary teeth. Similar findings were observed in the current study, wherein 78.84% of the mandibular premolar DTE cases lacked a specific cause. In most instances, succedaneous permanent teeth erupt naturally; yet occasionally, primary teeth may impede the eruption of their permanent successors, leading to potential benefits from primary tooth extraction [22]. Mucosal barriers can contribute to DTE in cases where no specific cause is evident on the panoramic radiograph, and surgical removal of these teeth may facilitate the eruption of the permanent tooth [23,24]. A similar case was observed in the current study (Table 2).
Mandibular premolars with Nolla stage 7 or lower DTE indicate developmental delay. Several studies have indicated that odontogenesis of the mandibular second premolar exhibits significant variability [2,3]. Park et al. [25] investigated developmental delays in Korean patients aged 6 to 12 years and reported that after maxillary second premolars and maxillary second molars, mandibular second premolars exhibited the highest prevalence of developmental delay, with an overall prevalence of 0.84% for mandibular premolar DTE. Instances of initial enamel calcification at the age of 13 have been reported in the case of the highly variable mandibular second premolar [26,27]. Therefore, the longer treatment duration observed in teeth belonging to the Nolla stage 7 or lower group compared to those in the Nolla stage 8 or higher group may be attributed to the inclusion of teeth with developmental delays in the current study (Table 5).
Physical obstructions, such as benign tumors, odontomas, and supernumerary teeth, should be removed to allow for the eruption of permanent teeth [5,7]. Cysts and benign tumors are commonly found in the canine and molar regions of the jaw [28], with odontomas being the most common odontogenic tumors within the oral cavity [29,30]. In the current study, the benign tumors included ameloblastic fibro-odontomas and odontogenic keratocysts, both of which are prevalent in the mandibular posterior region and can lead to impeded eruption of succedaneous permanent teeth, necessitating surgical removal [28,31]. Surgical treatment was performed for all cases involving benign tumors, odontomas, and supernumerary teeth in the present study. There are two main arguments regarding the treatment approach after the surgical removal of the physical obstacle along the eruption pathway. The first is that the tooth with delayed eruption should be exposed during the surgical removal of the obstacle [32], and the second suggests removing the obstacle and ensuring sufficient space for the succedaneous permanent tooth, thereby promoting spontaneous eruption [33]. Di Biase [34] supported the second approach, stating that if the dental follicle of the succedaneous permanent tooth is undamaged and adequate eruption space is ensured during surgery, 54% - 75% of the teeth would erupt spontaneously after 18 months. This aligns with the findings of the current study, where the duration of surgical treatment was 17.87 months.
Primary teeth with nonvital pulp often undergo cystic transformations, which can potentially cause delayed eruption in succedaneous permanent teeth. Thus, extraction of the nonvital tooth is necessary when symptoms arise [5,7]; this was one of the predominant causes of DTE in the present study (Table 2). The extraction of nonvital teeth can frequently lead to DTE in succedaneous permanent teeth. This phenomenon is often attributed to the premature extraction of primary teeth with nonvital pulp before the resorption of the roots, causing abnormal tissue changes in the upper region of the succedaneous permanent teeth and resulting in the formation of thick and fibrous gingiva [35]. As shown in Table 7, cases involving space maintenance after primary molar extraction exhibited longer treatment durations compared to follow-up alone, suggesting that this could be a contributing factor.
Ankylosis is the most common cause of delayed exfoliation of primary teeth and can lead to delayed eruption of succedaneous permanent teeth [36,37]. In a study by Kurol and Thilander [38], 73.1% of ankylosed primary teeth exhibited a mean or 6-month delayed shedding period without any intervention, and 23.1% showed a 12-month delayed shedding period, followed by an exchange with the succedaneous permanent teeth. Messer and Cline [36] reported that 62% of ankylosed primary teeth were naturally exchanged with succedaneous permanent teeth, whereas 38% required extraction. These findings suggest that space regaining should be performed in cases of insufficient eruption space due to tilting of the adjacent teeth caused by ankylosed primary teeth; additionally, orthodontic traction or surgical treatment might be necessary. In accordance with the treatment methods outlined in previous researches [36-38] for ankylosed primary molars, treatment methods were employed based on criteria such as eruption stage, impaction depth, and tilting of adjacent teeth. This encompassed follow-up, space maintenance after primary molar extraction, space regaining, and surgical treatment; however, only two out of seven cases with naturally erupted succedaneous permanent teeth were observed, which was lower than that seen in previous studies (Table 2). This phenomenon may be attributed to the nature of the university hospital setting, where patients who naturally experience eruptions are less commonly encountered.
Insufficient eruption space often results in an abnormal path of eruption for the tooth; occasionally, it can trigger a delayed eruption of the succedaneous permanent tooth, in which case adequate space for eruption must be created [39]. Most teeth with insufficient eruption space typically result in crowding as they erupt. However, in some cases where the lack of eruption space acts as a physical obstacle, and eruption may not occur naturally, it becomes necessary to create space through methods such as space regaining or extraction [5]. In this study, among the 12 cases with insufficient eruption space, six cases saw spontaneous eruption of the permanent successor teeth without any intervention. For four cases, space regaining was employed, and for two cases, extraction was performed to either secure eruption space or as a treatment method for the affected teeth (Table 2).
In cases of abnormal eruption pathways of maxillary canines, research suggests that not only the impaction depth but also the angle of inclination of the impacted crown can impact the prognosis and treatment duration [40]. A similar report exists for mandibular second premolars, providing treatment recommendations based on the depth and inclination of impaction [17]. As shown in Table 6, a lower eruption stage was associated with longer treatment periods. Furthermore, in Table 8, an increasing trend in the impaction depth and angle of inclination was observed with more invasive treatment methods, similar to the findings by Ismail et al. [17]. However, the previous study [17] classified based on the maximum value of the impaction depth and angle of inclination for each treatment method, whereas in this study, the 95% CI was calculated for each treatment method, and the minimum and maximum values were recorded in cases of insufficient sample size; additionally, the mandibular first and second premolars were included. Due to the insufficient sample size, statistical errors may occur as we were unable to calculate the 95% CI for the impaction depth and inclination in space regaining. Premolars often erupt and sometimes even erupt in a distal direction [41], with cases of restoration of normal eruption direction, highlighting the need for evaluating the eruption patterns at intervals of 3 - 6 months [42]; this may be due to the presence of the gubernacular cord [43]. The gubernacular cord is a structure of the dental lamina. It undergoes apoptosis, and the remains of the cord are organized into strands that align together. These strands are located in proximity to the reduced epithelium of the enamel organ and extend towards the oral mucosa. This, in conjunction with the coronal osteoclast action and apical osteogenesis of the dental follicle, guides tooth eruption [43]. Therefore, even in cases of ectopic eruption of mandibular premolars, the guidance provided by the gubernacular cord might help restore the normal eruption pathway.
In several studies [5,42], when a deviation of 90° or more from the normal eruption pathway was observed, autotransplantation was suggested as a viable option. In addition, it was suggested that a more invasive treatment approach should be considered if spontaneous positional improvement is not observed during regular radiographic observations. As seen in Table 4, the success rates of all treatment methods, excluding space regaining, ranged from 80.00% to 98.71%. Furthermore, when the initial treatment method proved ineffective, more invasive treatment options are available. Therefore, clinicians should always consider revising their treatment plans with a more invasive approach if there is no improvement in the chosen initial treatment method. However, the choice of treatment was left to the dentist’s discretion, and apart from studies like Ismail et al. [17], very few have proposed treatment methods based on the depth of impaction or angle of inclination of the tooth [5,7,17,44]. The state of root development in the affected tooth, as per the definition of biological DTE, plays a crucial role in determining the treatment approach. However, since there is currently no globally agreed-upon guideline for the treatment of mandibular premolar DTE, clinicians rely on their experiential judgment in clinical practice. Factors such as the tooth’s eruption stage, impaction depth, inclination angle, developmental stage, and root development status also influence the treatment decision. The lack of statistically significant differences in the treatment duration based on the treatment methods in Table 7 may be due to differences in the selection criteria for the treatment methods. Therefore, based on the 95% CI for impaction depth and inclination associated with each treatment method, we have proposed a guideline for the selection of treatment methods for mandibular premolars’ DTE in Fig. 3.
This study has several limitations. The study population consisted of patients from university hospitals, which may limit the generalizability of the findings to the broader population of children and adolescents in Korea. Additionally, being a retrospective study, investigations of the eruption timing and treatment duration were based on panoramic radiographs taken at predetermined intervals, which could potentially introduce discrepancies compared to the actual eruption timing and treatment duration. Furthermore, panoramic radiographs have limitations in providing a three-dimensional view of the tooth position and angle of inclination, suggesting the need for follow-up studies utilizing computed tomography scans to obtain more comprehensive information. Moreover, the relatively small sample size for each treatment method underscores the necessity for future follow-up studies involving larger and more diverse patient groups.
Conclusion
According to this study, the prevalence of DTE in mandibular premolars among Korean children was 5.19%. Establishing an appropriate timing for diagnosis and treatment planning is crucial for addressing DTE in mandibular premolars. Dentists can determine treatment methods based on the cause of DTE, developmental stage of the tooth, depth of impaction, and angle of inclination. This study reveals that the treatment duration for delayed eruption of mandibular premolars tends to increase with the increase in the impaction depth and angle of inclination of the tooth; moreover, the lower root developmental and eruption stages, the higher the treatment duration. Thus, the range of impaction depth and inclination angle according to the different treatment methods may aid in determining the appropriate treatment for DTE. Furthermore, there is a need to discuss objective and agreed-upon criteria for the treatment of delayed eruptions of mandibular premolars.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






