



Introduction
Coronavirus disease 2019 (COVID-19), an infectious respiratory disease caused by a novel coronavirus (SARS-CoV-2), first emerged in Wuhan, China, in December 2019 [1]. The World Health Organization (WHO) declared COVID-19 a public health emergency of international concern (PHEIC) on January 30, 2020 [2], and deemed it a global pandemic on March 11, 2020 [3]. On May 5, 2023, after approximately 3 years and 3 months, the declaration of a PHEIC for COVID-19 was lifted due to a decrease in cases, stable healthcare systems, and high levels of population immunity [4]. Although the global risk level for COVID-19 remains high, a decision has been made to transition to a long-term management of it [5].
The main route of transmission for the coronavirus has been suggested to be person-to-person, mainly through saliva droplets and contact with contaminated surfaces [6]. In dental settings, it can spread when dental equipment generates aerosols or droplets that contain the saliva and blood of infected individuals. Aerosol particles are very small and can remain suspended in the air for a long time, allowing them to enter the respiratory systems of other patients or settle on the surfaces of dental equipment, leading to potential transmission of the virus [7]. In August 2020, the WHO recommended essential oral health services and the minimization of aerosolgenerating procedures (AGPs), with an emphasis on the use of personal protective equipment [8]. In December 2020, South Korea also advised using proper protective equipment, hand hygiene, surface disinfection, and ventilation [9]. Both guidelines suggested limiting nonessential dental visits and prioritizing essential treatments, especially for confirmed or suspected COVID-19 patients. These recommendations led to patients delaying or canceling dental visits, resulting in a significant decrease in both emergency and non-emergency dental appointments during the pandemic [10]. As a result, dental services have experienced significant disruptions worldwide [8,11-13]. Nonetheless, South Korea continued to provide routine dental care services without a lockdown throughout the pandemic period [14,15].
Only a few studies have considered the impact of COVID-19 on pediatric dentistry in South Korea by analyzing changes in dental service use among children and adolescents following the occurrence of the pandemic. Recent domestic research in South Korea on this topic was conducted using big data from the Health Insurance Review and Assessment Service [16-18]. Those studies investigated the period from January to August or December 2020, during the COVID-19 pandemic [16,17], or focused on dental trauma [18]. Additionally, they relied on publicly available statistical data from the Health Insurance Review and Assessment Service, which includes only items claimed through medical insurance. Apart from COVID-19, previous studies on patient distribution and practice patterns at the Pediatric Dentistry Department of Seoul National University Dental Hospital have also been conducted [19,20]. However, there has been insufficient research on the impact of COVID-19 on pediatric dental service use in South Korea until 2022, just before the PHEIC was lifted.
Therefore, our objective is to analyze the number of visits, patient age, gender, diagnoses, and treatments within the Pediatric Dentistry Department of Seoul National University Dental Hospital from 2017 to 2022, comparing and evaluating the periods before and during COVID-19 outbreaks. This research holds clinical significance for pediatric dentists and dental hospitals as it serves as a resource for predicting and managing patient dental visits during pandemics. Consequently, it can contribute to safeguarding the oral health of pediatric patients by emphasizing the need for health authorities and healthcare facilities to develop strategies for future pandemic situations.
Materials and Methods
This retrospective study was conducted with the approval of the Institutional Review Board of Seoul National University Dental Hospital (IRB No. ERI23030).
1. Subjects
This study included 75,439 individuals who visited the Pediatric Dentistry Department of Seoul National University Dental Hospital between January 1, 2017 and December 31, 2022. Patients whose data were not aggregated in the Order Communication System of Seoul National University Dental Hospital were excluded from this study.
2. Methods
The Order Communication System of Seoul National University Dental Hospital was used to aggregate data about the study subjects. The data cover the period from January 1, 2017, to December 31, 2022. In this study, the period from January 1, 2017, to December 31, 2019, is defined as the pre-COVID period, and the period from January 1, 2020, to December 31, 2022, is defined as the COVID-19 period.
From 2017 to 2022, we collected data on visit counts, patient age and gender, diagnostic codes, and prescription codes on a yearly basis. The age groups were defined as follows: 0 - 4 years for preschool children, 5 - 9 years for elementary school students in lower grades, 10 - 14 years for elementary school students in higher grades and middle school students, 15 - 19 years for adolescents preparing for high school and college entrance. Although specific age-related variations in COVID-19 infection among children and adolescents have not been documented [21], disparities in government policie [22-25] and the psychological state of patients and their caregivers in response to the pandemic [26] have been observed. Consequently, to examine age-related distinctions and compare them with previous research findings, patients were categorized into 5 age groups: 0 - 4 years, 5 - 9 years, 10 - 14 years, 15 - 19 years, and 20 years and older.
Age and gender data were further analyzed for specific diagnostic codes, Z29.8 (need for other specified prophylactic measures), K02.1 (caries of dentine), and K07.4 (malocclusion, unspecified), because those codes represent more than 10% of cases each year. Treatments were categorized into 6 groups: preventive treatment, restorative treatment, pulp treatment, surgical treatment, orthodontic treatment, and trauma treatment. Each treatment group was investigated by aggregating the prescription codes for specific treatment procedures within each group. The specific procedures and corresponding prescription codes for each treatment group are listed in Table 1. Sedation was investigated using prescription codes for chloral hydrate, hydroxyzine, and midazolam, and general anesthesia was examined using the prescription code for endotracheal closed circuit general.
3. Statistical analysis
We used Excel 2019 (Microsoft Co., Redmond, WA, USA) to calculate basic statistics about the collected data. Chi-square test was used to measure the differences in age and gender between the pre-COVID and COVID-19 periods for all patients and those with diagnostic codes Z29.8, K02.1, or K07.4. In addition, a logistic regression analysis was used to determine whether COVID-19 correlated with significant changes in age groups or gender. A 95% confidence interval (CI) and a significance level of ╬▒ = 0.05 were considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 21 (IBM Corp., Armonk, NY, USA). In data processing, the count of dental visits encompassed all a patientŌĆÖs visits within a year, and patient numbers were tallied without duplication for demographic statistics. To mitigate variations in visit frequency due to specific diagnostic codes (Z29.8, K02.1, or K07.4), the analysis focused on patient counts rather than visit numbers.
Results
1. Number of dental visits
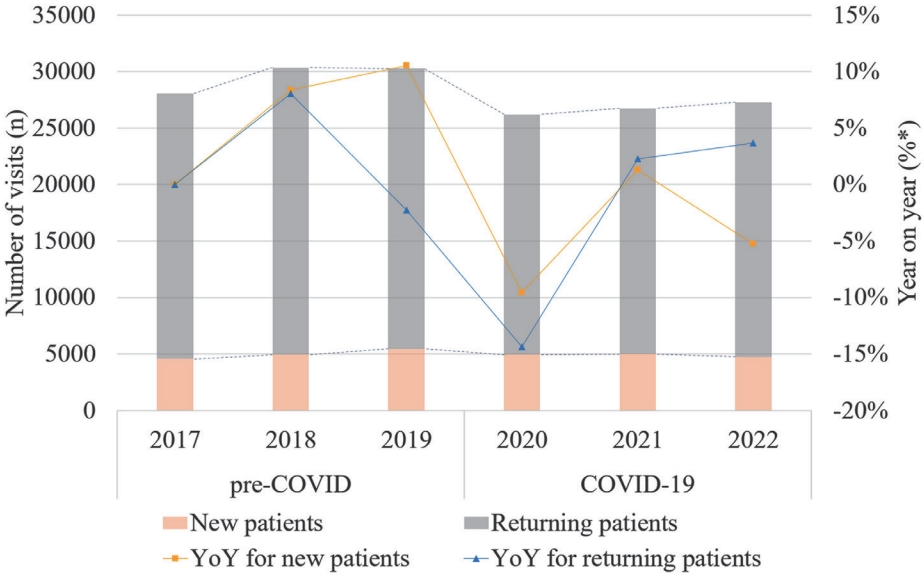
The visit count for new patients decreased by 1.85% during the COVID-19 period, compared with the pre-COVID period: a 9.54% decrease in 2020, followed by a 1.32% increase in 2021 and a 5.26% decrease in 2022. The visit count for returning patients decreased by 11.12% during the COVID-19 period, compared with the pre-COVID period: a 14.36% decrease in 2020, followed by a 2.27% increase in 2021 and a 3.65% increase in 2022 (Table 2, Fig. 1).
2. Distribution of age and gender
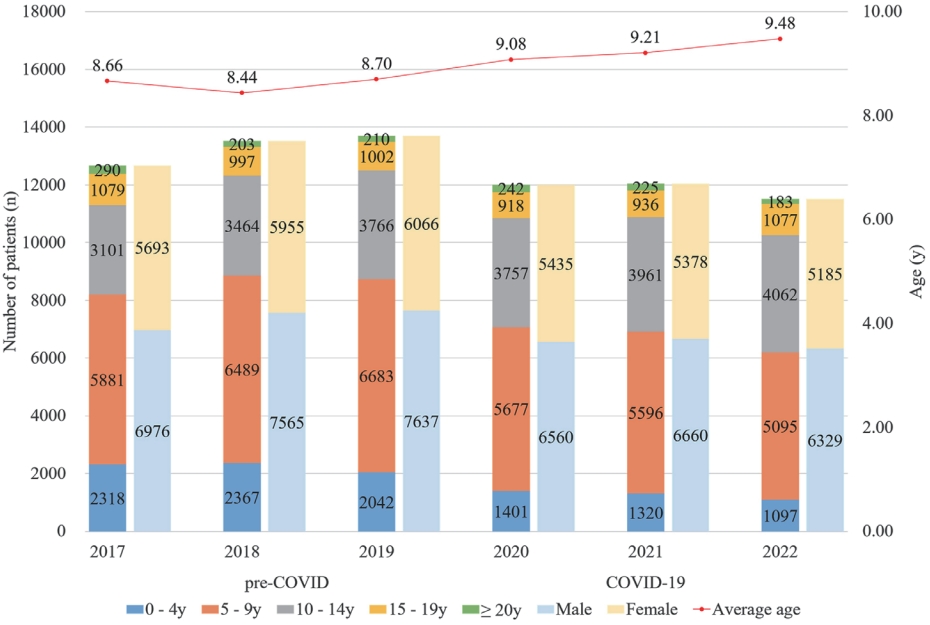
The age distribution, average age, and gender distribution of patients who visited from 2017 to 2022 are shown in Fig. 2. The changes in patient numbers for each age group compared to the previous year, as well as the shifts observed between the pre-COVID and COVID-19 periods, are presented in Table 3. During COVID-19, patient numbers decreased significantly in the following age groups, in order of age: 0 - 4 years, 5 - 9 years, 15 - 19 years, and 20 years and older, while the 10 - 14 years age group saw an increase. There was a statistically significant difference between the age groups in the pre-COVID and COVID-19 periods (Table 4, p < 0.0001). The 0 - 4 year-old age group was 0.615-fold less likely to visit in the COVID-19 period (adjusted odds ratio [AOR], 0.615; 95% CI, 0.548 - 0.689; p < 0.0001), and the 10 - 14 years age group was 1.234-fold more likely to visit in the COVID-19 period (AOR, 1.234; 95% CI, 1.106 - 1.378; p < 0.0001) than the 20 year and older age group (Table 5). The number of males and females did not differ significantly between the pre-COVID and COVID-19 periods (Table 4, p = 0.098).
3. Distribution of diagnoses
The distribution of diagnostic codes for all patients from 2017 to 2022 is shown in Table 6. Among them, Z29.8, K02.1, and K07.4 accounted for more than 10% each year. The age groups differed significantly between the pre-COVID and COVID-19 periods in each of those three diagnostic codes (Table 4, p < 0.0001). For Z29.8, the 0 - 4 years age group was 0.477-fold less likely to visit in the COVID-19 period (AOR, 0.477; 95% CI, 0.390 - 0.584; p < 0.0001), the 5 - 9 years age group was 0.762-fold less likely to visit in the COVID-19 period (AOR, 0.762; 95% CI, 0.630 - 0.922; p = 0.005), and the 15 - 19 years age group was 0.740-fold less likely to visit in the COVID-19 period (AOR, 0.740; 95% CI, 0.603 - 0.909; p = 0.004) than the 20 years and older age group (Table 5). For K02.1, the 0 - 4 years age group was 0.422-fold less likely to visit in the COVID-19 period (AOR, 0.422; 95% CI, 0.290 - 0.614; p < 0.0001) than the 20 years and older age group (Table 5). For K07.4, the 5 - 9 years age group was 0.658-fold less likely to visit in the COVID-19 period (AOR, 0.658; 95% CI, 0.475 - 0.912; p = 0.012) than the 20 years and older age group (Table 5). Among Z29.8, K02.1, and K07.4, only K07.4 showed a statistically significant difference between males and females in the pre-COVID and COVID-19 periods (Table 4, p = 0.004). For K07.4, females were 1.141-fold more likely to visit in the COVID-19 period (AOR, 1.141; 95% CI, 1.047 - 1.243; p = 0.003) than males (Table 5).
4. Distribution of dental treatments
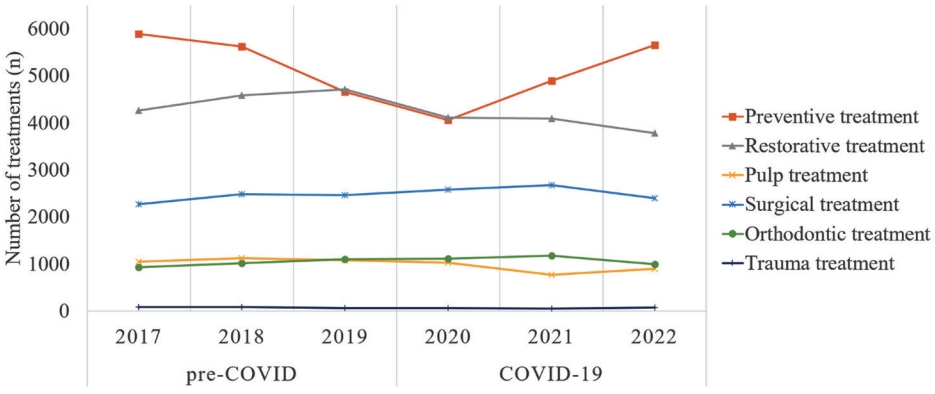
Compared with the pre-COVID period, the number of total treatment procedures decreased by 7.04% during the COVID-19 period. Preventive treatment, restorative treatment, pulp treatment, and trauma treatment decreased by 9.71%, 11.64%, 16.70%, and 18.62%, respectively, compared with the pre-COVID period. However, surgical treatment and orthodontic treatment increased by 6.04% and 7.78%, respectively, compared with the pre-COVID period (Table 7, Fig. 3).
5. Distribution of sedation and general anesthesia
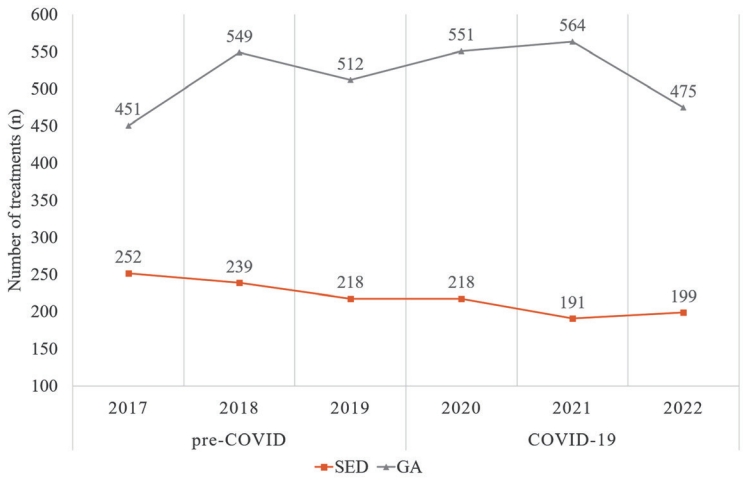
The use of sedation decreased by 14.25%, and the use of general anesthesia increased by 5.16% during the COVID-19 period compared with the pre-COVID period (Fig. 4).
Discussion
The first case of COVID-19 in South Korea was confirmed on January 20, 2020, and the country confronted the challenges posed by the pandemic, which subsequently led to the enforcement of social distancing measures starting on February 29, 2020 [25,27]. Afterward, the first vaccine dose was administered on February 26, 2021, and by October of the same year, the nationwide vaccination rate had achieved 70%. This milestone marked the initiation of a phased return to normalcy, commencing on November 1, 2021 [23,25]. However, the emergence of the highly transmissible Omicron variant on December 1, 2021, led to a renewed surge in confirmed cases, temporarily halting the phased return to normalcy. Nevertheless, in light of the increased public fatigue due to the prolonged pandemic, the paradigm shifted towards autonomous infection prevention rather than strict epidemic control [27,28]. Eventually, social distancing measures in South Korea were lifted on April 18, 2022 [27], and the WHO lifted the PHEIC declaration for COVID-19 on May 5, 2023 [4]. We conducted a thorough analysis of pediatric and adolescent dental service utilization before and during the COVID-19 outbreak to evaluate the pandemicŌĆÖs impact.
The total fertility rate (TFR) in South Korea has remained at record-low levels since the early 2000s, experiencing a continuous decline [29]. Despite these demographic trends, annual dental utilization among children and adolescents steadily increased, with a temporary decrease in 2020 due to the COVID-19 pandemic, which was not fully recovered in the subsequent years [30]. Shree et al. [31]ŌĆÖs study found that concerns about COVID-19 exposure risk resulted in a decline in dental visits, with approximately 50% of parents postponing their childrenŌĆÖs treatments. Nevertheless, over 95% expressed their willingness to return if they and their children were vaccinated. According to Son and Kim [16], nationwide dental visits for children aged 0 to 9 decreased by 16.3% during the first eight months of 2020, when COVID-19 emerged in South Korea, compared with the same period in the previous year, and visits for those aged 10 to 19 decreased by 9.2%. In our research, compared to 2019, the number of patients visiting the Seoul National University Dental Hospital in 2020 decreased by 18.88% in the 0 - 9 age group and by 1.95% in the 10 - 19 age group. In comparison to the results of Son and KimŌĆÖs research, a significant difference was observed in the higher age groups. According to Lee et al. [32]ŌĆÖs study, patients visiting university hospitals for surgical procedures and orthodontic treatment have been steadily increasing compared to local dental clinics. Surgical procedures are typically single occurrences, while orthodontic treatment requires regular and extended appointments. Consequently, it appears that older age groups receiving orthodontic treatment consistently maintained their visits to dental hospitals even during a pandemic. When analyzing dental visits for new and returning patients, both experienced substantial declines during the initial stages of the COVID-19 outbreak in 2020, followed by slight increases in 2021, the year when vaccinations were conducted [25,31]. However, in 2022, a distinct trend was noticed: new patient visits decreased, but returning patient visits increased. According to Seo et al. [20], the number of new patient visits to the Pediatric Dentistry Department at Seoul National University Dental Hospital has shown an increasing trend since 2010. However, the decline in new patient visits in 2020 and 2022 was due to COVID-19, and the smaller decrease in 2022, compared to 2020, can be attributed to the stability observed following the Omicron peak in March 2022, which led to the easing of social distancing measures [27]. The ongoing rise in returning patients from 2021 to 2022 can be attributed to the convenience of scheduling dental appointments in advance, unlike new patients. Despite the return to full in-person classes for students in 2022 and the readjustment to school life, which reduced dental visits during school hours [23,24], the returning patient reservation system enabled them to plan specific dates and times for their dental appointments.
During the pre-COVID and COVID-19 periods, there was no statistically significant difference in the number of visits between males and females (p = 0.098). On the other hand, there was a statistically significant decrease in visits from patients in the 0 - 4 year-old age group (p < 0.0001) during the COVID-19 period. Specifically, the 0 - 4 age group showed a slight increase in 2018 but has been continuously decreasing since 2019. The rapid decline that began before COVID-19 suggests that factors other than COVID-19 played a role in the persistent decrease in patient numbers in the 0 - 4 age group. An et al. [33] investigated whether the declining birth rate affected the demand for pediatric dental services. Despite a significant decrease in the number of births over the past decade, the study predicted that the number of pediatric dental patients would remain relatively stable and even slightly increase. However, this study had limitations as it focused on specific regions and tertiary institutions, and did not categorize patients based on criteria such as age. According to a study by Lee et al. [32] conducted on patients of the Pediatric Dentistry Department at Pusan National University Dental Hospital, the 0 - 3 age group accounted for less than 10%. Kim et al. [34] investigated the reasons for infants and young children visiting dentists, and the results showed that oral examinations, routine check-ups, and dental caries prevention accounted for over 90%. The increase in local pediatric dental clinics may have led to a decrease in younger patients seeking check-ups and care for dental caries at university hospitals. Analyzing the variation in the number of births by year revealed that the decrease in the number of births was relatively prominent in 2017 when compared to the preceding and subsequent years. When considering that the first stage of national oral health screening for infants and children is recommended around 18 - 29 months after birth and that the entire primary dentition is typically completed around the age of 2 years, the lower birth rate in 2017 might have influenced the decrease in the number of patients aged 0 - 4 years since 2019, approximately two years after 2017. Additionally, the lower likelihood of infants and young children visiting university hospitals may have had an extra impact. In contrast, there was a statistically significant increase in visits from patients in the 10-14-year-old age group (p < 0.0001) during the COVID-19 period. The Ministry of Food and Drug Safety (MFDS) approved the Pfizer vaccine for those aged 12 and above, with vaccination starting in October 2021 for children and adolescents [35]. Meanwhile, the regulations of the delayed commencement of school and the phased return to in-person classes were less stringent for senior high school students in comparison to elementary and middle school students [36]. Vaccination, reducing concerns about COVID-19 transmission compared to younger age groups, and the greater availability of time for dental care utilization, unlike older adolescents, may have led to the increase in the 10 - 14 age group.
The diagnostic codes Z29.8, K02.1, and K07.4 exhibited statistically significant differences by age group (p < 0.0001) before and during COVID-19. Z29.8 showed statistically significant decreases in the 0 - 4 years (p < 0.0001), 5 - 9 years (p = 0.005), and 15 - 19 years (p = 0.004) age groups during the COVID-19 period, compared with the pre-COVID period. Son and KimŌĆÖs research [16] revealed a substantial reduction in visits related to diagnostic code Z29 until August 2020, compared with the same period in 2019, with a 34% reduction in the 0 - 9 age group and a 9.2% reduction in the 10 - 19 age group. Our study aligns with that finding, with a 29.78% (1,969 patients) reduction in the 0 - 9 age group and a 12.97% (546 patients) reduction in the 10 - 19 age group, showing the largest decrease among the three diagnostic codes. In particular, the most significant decrease was observed in the 0 - 4 age group, while the 5 - 9 age group and the 15 - 19 age group showed similar decreases. The 10 - 14 age group experienced the least reduction. This suggests that visits to pediatric dental hospitals for regular checkups or preventive visits without any specific motivation decreased during the COVID-19 period, especially in very young children. K02.1 showed a statistically significant decrease in the 0 - 4 years age group (p < 0.0001), with a 51.44% (1,054 patients) reduction. Although not statistically significant, there were declines in the 5 - 9 years and 15 - 19 years age groups, with reductions of 16.92% (739 patients) and 10.98% (45 patients), respectively, during the COVID-19 period compared to the pre-COVID period. In contrast, Kim et al.ŌĆÖs study [17] reported an overall increase in dental visits related to dental caries across all age groups, as they calculated values while considering the impact of year-to-year population differences. Furthermore, our study specifically concentrated on cases under K02.1 (caries of dentine) at Seoul National University Dental HospitalŌĆÖs Pediatric Dentistry Department, while Kim et al.ŌĆÖs study examined all cases under the diagnostic code K02 (dental caries) nationwide. Nevertheless, during the COVID-19 period, both studies found a consistent order in the age groups seeking dental care due to dental caries: 10 - 14 years, 15 - 19 years, 5 - 9 years, and 0 - 4 years. The nationwide increase in dental visits for caries during the COVID-19 period in Kim et al.ŌĆÖs study could be attributable to the governmentŌĆÖ s restrictions on outdoor activities and the prolonged time spent at home, leading to an increased frequency of consuming cariogenic foods among children and adolescents [37]. Compared to other age groups, the significant decrease in the 0 - 4 years age group appears to be influenced by the choice of patients and their caregivers in this age group to visit local dental clinics rather than opting for a tertiary care center. This shift in preference may be attributed to reduced mobility and decreased use of public transportation during the COVID-19 period [25,38]. K07.4 showed a statistically significant decrease of 7.37% (107 patients) in the 5 - 9 years age group (p = 0.012) during the COVID-19 period compared to the pre-COVID period. Furthermore, although not statistically significant, there was a 12.07% (7 patients) decrease in the 0 - 4 years age group, while the 10 - 14 years age group saw an increase of 37.47% (679 patients), and the 15 - 19 years age group showed an 11.68% (62 patients) increase. Additionally, there was a statistically significant 1.14 times increase in females compared to males (p = 0.003). In Son and KimŌĆÖs study [16], patients diagnosed with K07 in the 0 - 9 years age group showed a decrease of 11.77% in 2020 compared to the previous year, while the 10 - 19 years age group exhibited an increase of 5.67%. Our research findings align with the observation of a decline in younger age groups and an increase in older age groups. However, our finding in the 10-19 age group, especially among those aged 10-14, showed a more significant increase. This can be attributed to the unique characteristics of university hospitals and the increased demand for orthodontic treatment compared to the past [39-41]. The pandemic has not dampened the demand due to infection control measures [42] and the characteristics of orthodontic treatment, such as short chair time, less use of high-speed turbines, and limited generation of droplets and aerosols [43]. Omran and Dowie [43] noted an increase in demand for orthodontic treatments during the COVID-19 pandemic, attributing it to the shift to online classes and meetings, which led to a surge in the use of video platforms, often referred to as the Zoom boom. This phenomenon has increased the desire for orthodontic treatments to enhance esthetics, particularly among older age groups and girls, as they spend extended periods viewing themselves on video. In a study by Yilanci et al. [44], the most significant advantage of undergoing orthodontic treatment during the pandemic was reported as the ability to conceal appliances like braces and wires with mask usage, in addition to reduced social interaction among individuals.
The number of preventive, restorative, pulp, and trauma treatments decreased, while surgical and orthodontic treatments increased during the COVID-19 period. Preventive treatment decreased in 2020, and this trend was observed in various countries, including Turkey, Brazil, and Germany [10,13,17,45]. According to Lyu and Wehby [46], bleeding gingivae showed the highest risk increase among the oral health problems, indicating deterioration in the oral hygiene of pediatric patients following the onset of COVID-19. With the rise in total dental visits in 2021 and 2022, preventive treatments were likely actively performed to enhance oral health following the prior yearŌĆÖs deterioration. In Kim et al.ŌĆÖs study [17], restorative and pulp treatments both decreased in 2020. In our research, restorative treatment decreased throughout the COVID-19 period, and pulp treatment decreased until 2021 but increased in 2022. The decline in restorative treatment during the COVID-19 period suggests a delay in dental caries treatment, implying the progression of dental caries [47,48]. This, in turn, raises the possibility of an increased need for pulp treatment, and as social distancing measures were eased in 2022, patients experiencing pain or extensive caries sought dental care. The rise in surgical and orthodontic treatments until 2021 can be attributed to the increased availability of time during the COVID-19 pandemic. This led to a heightened demand for surgical procedures such as supernumerary tooth extraction or odontoma removal involving postoperative recovery time, as well as orthodontic treatments requiring regular visits over an extended period. Furthermore, some patients might have chosen extraction of a primary tooth rather than pulp and restorative treatments, which generate aerosols [49], or untreated carious teeth worsened during the pandemic were subsequently extracted [47,48]. In 2022, as nationwide in-person schooling resumed, children and adolescents adjusted to regular school attendance [50], and during their adaptation to daily life, there was likely a decrease in demand for surgical and orthodontic treatments, in contrast to the previous year. Furthermore, patients with severely decayed teeth might have chosen pulp treatment rather than extraction in 2022. Trauma treatment did not show any notable difference in 2020 compared with the previous year. According to Son et al.ŌĆÖs study [18], the number of traumatic dental injury patients per 100,000 individuals decreased by 3.5% in 2020 compared with the average from 2017 to 2019. The primary distinction in the results between the two studies is attributed to the difference in the analytical approach. Son et al.ŌĆÖs study predominantly relied on diagnostic codes, whereas our study focused on prescription codes associated with trauma. Son et al. investigated the incidence of diagnostic codes, encompassing open wounds of the lips and mouth, dental fractures, and dental avulsions. In contrast, we specifically scrutinized treatment procedures, including luxation tooth reduction, avulsion tooth replantation, resin wire splinting, and trauma suturing. After 2020, the number of trauma treatments decreased in 2021 and then increased in 2022. The decrease in 2021 can be attributed to a reduction in outdoor activities for children and adolescents due to social distancing and outing restrictions. However, after those restrictions were lifted, outdoor activities presumably increased, which subsequently led to an increase in trauma cases during 2022.
When analyzing the use of sedation, a study by Seo et al. [20] from 2006 to 2015 found that the frequency of sedation procedures at Seoul National University Dental HospitalŌĆÖs Pediatric Dentistry Department remained rela-tively stable, with around 200 cases per year from 2012 onwards. However, in our study, we observed a gradual decline in the number of sedation procedures, from 252 cases in 2017 to 199 cases in 2022. Although the number of sedation procedures decreased by 14.25% during COVID-19, the number of sedation procedures during 2020 did not differ notably from that in the previous year. Therefore, the decline in sedation procedures can be attributed to the decreasing trend observed from 2017 to 2022. The pattern of general anesthesia use fluctuated over the years. During the COVID-19 period, it increased by 5.16% compared with the pre-COVID period. 2020 and 2021 witnessed a rise in the number of general anesthesia procedures, reaching the highest level in 2021 with 564 cases. The increase in surgical procedures, which often require general anesthesia, might have contributed to the higher use of general anesthesia during those years. In a study by Han et al. [51] on dental treatments under general anesthesia, it was reported that surgical procedures occurred twice as frequently under general anesthesia compared to dental caries treatments in cases classified as ASA grade 1. In contrast, 2022 saw a 15.78% decrease in the use of general anesthesia compared with the previous year. Similarly, the decline in the number of surgical procedures in 2022 aligns with the reduction in the use of general anesthesia, suggesting a possible correlation between the two. However, further research is needed to investigate the specific types of dental treatment performed under general anesthesia during the COVID-19 period to better understand this relationship. In countries that experienced lockdowns during the COVID-19 period, some restrictions were imposed on dental treatment under general anesthesia, and the number of cases decreased compared with the pre-COVID period. However, with the cessation of lockdowns, the number of dental treatments under general anesthesia gradually recovered to their pre-pandemic levels [52-54]. On the contrary, South Korea had no lockdown periods, and the impact observed in certain other countries, where general anesthesia procedures were restricted, did not seem to have occurred.
According to a literature overview conducted by Checchi et al. [55], patients should undergo a preliminary evaluation, which entails checking their body temperature and conducting a brief survey to ask about any fever, respiratory problems such as cough or difficulty breathing, and recent contact with individuals who might have been exposed to infection within the past two weeks. Patients who answer affirmatively to any of these survey questions and have a body temperature exceeding 37.5┬░C should be isolated at home or hospitalized. Patients are advised to avoid dental treatment unless it is an emergency or until they meet the criteria for quarantine release. Additionally, even if they have recovered from COVID-19, it is recommended to wait 30 days after the resolution of symptoms before seeking dental care. Furthermore, patients who answer affirmatively to any of the survey questions but have a body temperature below 37.5┬░C are advised to refrain from dental treatment for at least 14 days. Therefore, teledentistry has emerged as an innovative method that minimizes the risk of cross-infection, and its potential usefulness in future pandemics is recognized [56]. During the lockdown, which was implemented by dental associations worldwide, including the Centers for Disease Control and Prevention (CDC) and the American Dental Association (ADA) [57-61], dentists adopted teledentistry, offering regular dental care through telephone or video consultations. They assessed cases for emergency needs and provided necessary dental treatment when required [62,63]. In future situations like the COVID-19 pandemic, it is crucial to stress the importance of continuous oral care to patients and their guardians. Pediatric dentists can effectively use teledentistry through platforms like YouTube or KakaoTalk channels for remote dental consultations for children and adolescents during pandemics. Additionally, dental practitioners should minimize AGPs and employ infection prevention measures. To prevent infection, it is advisable to avoid AGPs such as the use of 3-way syringes, high-speed handpieces, ultrasonic scalers, and nitrous oxide and oxygen sedation. If possible, priority should be given to the use of rubber dams, low-speed handpieces, atraumatic restorative techniques like the Hall technique, fissure sealants, silver diamine fluoride, and remineralizing agents. Additionally, extraoral radiographies such as panoramas or cone-beam CT scans should be preferred over intraoral radiography. Developing pandemic preparedness manuals and negative pressure isolation rooms are essential steps for health authorities and healthcare facilities to prevent the spread of infectious diseases [55,64].
On May 5, 2023, WHO lifted the PHEIC declaration for COVID-19. As a result, Seoul National University Dental Hospital abolished the mandatory use of KF94 masks for healthcare workers starting June 1, 2023. Instead, they now selectively choose appropriate personal protective equipment based on their assessment of patient contact areas and potential sources of infection. As a retrospective analysis, this study has several limitations. First, since this study analyzed data from a single institution, the results of this study cannot be applied to trends in all dental patients in the country. Second, patient dental visitation can be influenced by factors other than COVID-19, so results cannot be generalized as being solely due to COVID-19. Third, the study period only included data up to 2022, and we were unable to conduct research on the post-pandemic period after the declaration of PHEIC for COVID-19 was lifted. Preventing oral health risks during the pandemic is crucial, as neglect and delays in treatment can lead to worsened oral health, potentially necessitating more extensive procedures in the long term. Therefore, it is necessary to conduct a follow-up study on changes in dental visitation and dental treatment patterns after the pandemic, including the number of patients, their chief complaints, as well as diagnostic and treatment details. Furthermore, we suggest additional research at other university hospitals and private pediatric dental clinics. This study would provide valuable insights into changes in dental services induced by the pandemic. When compared with data after the end of COVID-19, it could serve as a useful and specific reference for dentists and dental hospitals, aiding in the development of strategies to safeguard the oral health of children and adolescents during future pandemic situations.
Conclusion
In conclusion, the COVID-19 pandemic influenced various aspects of pediatric dental service use at Seoul National University Dental HospitalŌĆÖs Pediatric Dentistry Department. The total number of visits decreased, especially in 2020, affecting patients across all age groups except for those 10 - 14 years old, with no significant gender difference. Specific diagnostic codes showed varying trends, with Z29.8 and K02.1 exhibiting decreases in most age groups and K07.4 having mixed results. From 2020 to 2022, preventive, restorative, pulp, and trauma treatments decreased, whereas surgical and orthodontic treatments increased. Moreover, sedation use decreased and general anesthesia increased after COVID-19 compared with the pre-pandemic period. These findings highlight the dynamic changes in pediatric dental care that occurred during the pandemic. This study holds clinical significance as a reference for predicting and managing changes in the overall patterns of pediatric dental patient visits during future pandemics. Pediatric dentists can perform teledentistry for non-face-to-face dental consultations and treatments to maintain oral health in children and adolescents during pandemic periods. Health authorities and healthcare facilities can develop pandemic preparedness manuals and establish negative pressure isolation rooms, which are crucial tools in preventing the spread of infectious diseases.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






